Genes
This page describes gene-specific information. PyPGx currently supports genotyping of a total of 88 pharmacogenes.
In order to provide the most accurate information, this page borrows heavily from the works of the Clinical Pharmacogenetics Implementation Consortium (CPIC) and the Pharmacogenomics Knowledge Base (PharmGKB). All curated contents published by CPIC and PharmGKB are available free of restriction under the CC0 1.0 Universal (CC0 1.0) Public Domain Dedication and the Creative Commons Attribution-ShareAlike 4.0 International License, repsectively.
Many of the genes are known to have structural variation (SV) including gene deletions, duplications, and hybrids. Please read the Structural variation detection page for more details.
Some genes have a genotype-phenotype table available from CPIC or PharmGKB. Please read the Phenotype prediction page for more details.
Below is a summary table:
Gene |
Variants |
SV |
Phenotype |
PharmVar |
CPIC |
Function |
GRCh37 |
GRCh38 |
Notes |
|---|---|---|---|---|---|---|---|---|---|
ABCB1 |
✅ |
Disposition |
|||||||
✅ |
✅ |
✅ |
Disposition |
||||||
ACYP2 |
✅ |
Metabolism |
NM_138448.4 was used as the main transcript. |
||||||
ADRA2A |
✅ |
Absorption |
NM_000681.4 was used as the main transcript. |
||||||
ADRB2 |
✅ |
Target |
NM_000024.6 was used as the main transcript. |
||||||
ANKK1 |
✅ |
Metabolism |
NM_178510.2 was used as the main transcript. |
||||||
APOE |
✅ |
Efficacy |
NM_000041.4 was used as the main transcript. |
||||||
ATM |
✅ |
Efficacy |
NM_000051.4 was used as the main transcript. |
||||||
BCHE |
✅ |
Efficacy |
NM_000055.4 was used as the main transcript. |
||||||
BDNF |
✅ |
Efficacy |
NM_001709.5 was used as the main transcript. |
||||||
✅ |
✅ |
✅ |
Target |
||||||
✅ |
✅ |
✅ |
Target |
||||||
COMT |
✅ |
Metabolism |
|||||||
✅ |
✅ |
Metabolism |
|||||||
✅ |
✅ |
Metabolism |
|||||||
✅ |
✅ |
Metabolism |
|||||||
✅ |
✅ |
✅ |
Metabolism |
CYP2A6 has pseudogene (CYP2A7). |
|||||
✅ |
✅ |
Metabolism |
|||||||
✅ |
✅ |
✅ |
✅ |
✅ |
Metabolism |
CYP2B6 has pseudogene (CYP2B7). |
|||
✅ |
✅ |
Metabolism |
|||||||
✅ |
✅ |
✅ |
✅ |
Metabolism |
|||||
✅ |
✅ |
✅ |
✅ |
Metabolism |
|||||
✅ |
✅ |
✅ |
✅ |
✅ |
Metabolism |
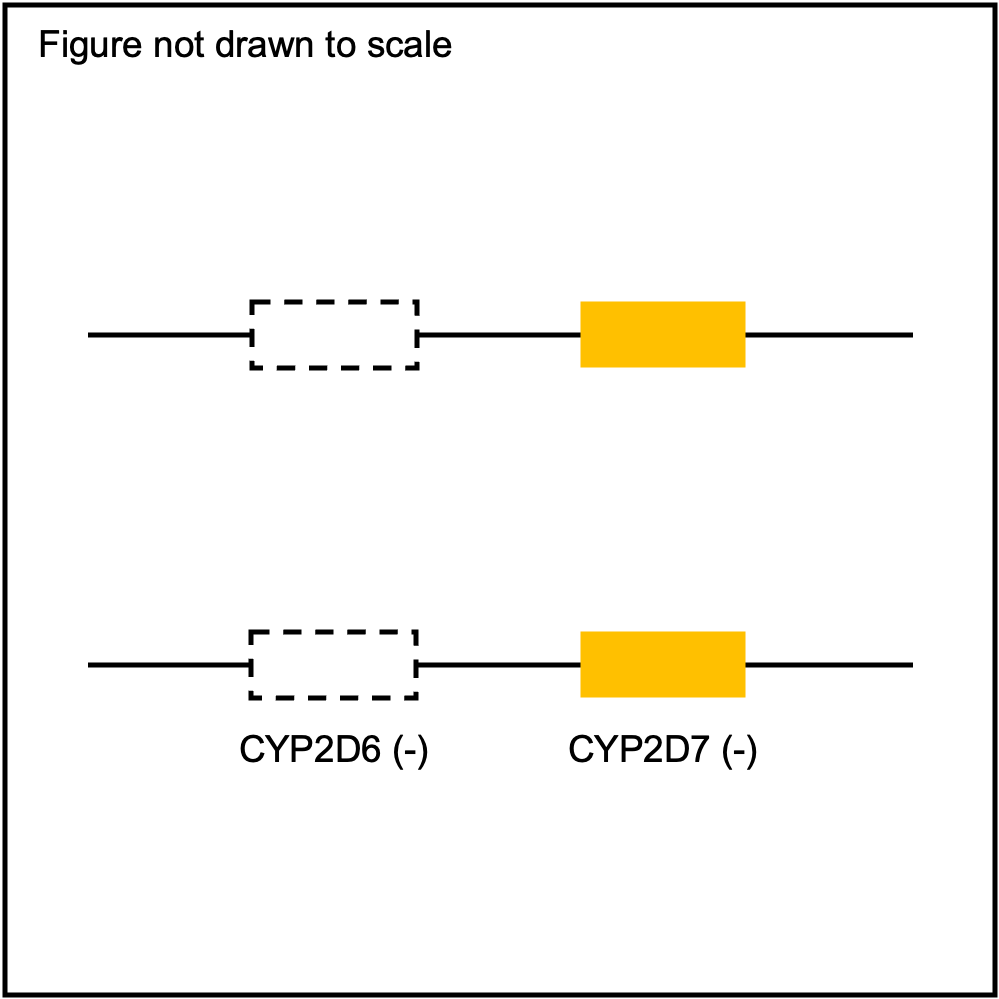
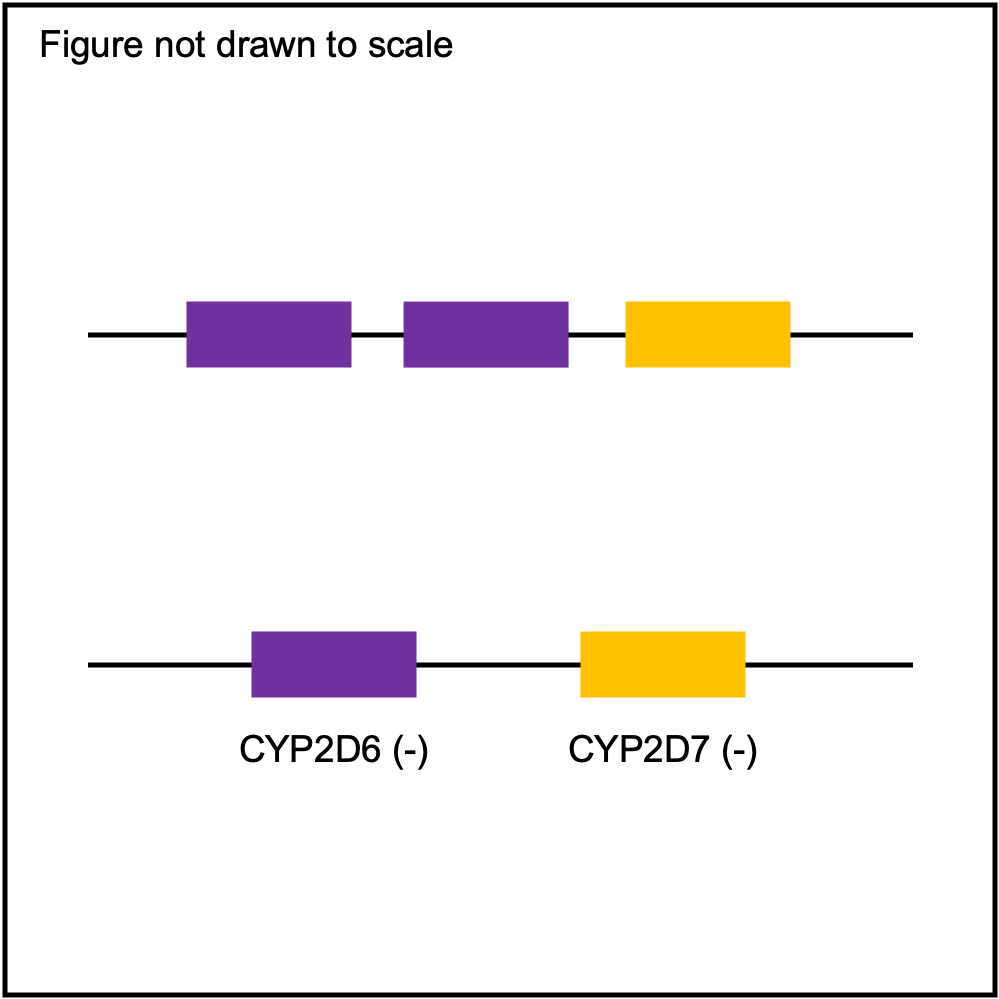
CYP2D6 has pseudogene (CYP2D7). |
|||
✅ |
✅ |
✅ |
Metabolism |
||||||
✅ |
✅ |
Metabolism |
|||||||
✅ |
✅ |
Metabolism |
|||||||
✅ |
✅ |
Metabolism |
|||||||
✅ |
✅ |
Metabolism |
|||||||
✅ |
✅ |
Metabolism |
|||||||
✅ |
✅ |
Metabolism |
|||||||
✅ |
✅ |
✅ |
✅ |
Metabolism |
|||||
✅ |
✅ |
Metabolism |
|||||||
✅ |
✅ |
Metabolism |
|||||||
✅ |
✅ |
Metabolism |
|||||||
✅ |
✅ |
Metabolism |
|||||||
✅ |
✅ |
Metabolism |
|||||||
✅ |
✅ |
✅ |
Metabolism |
||||||
✅ |
✅ |
Metabolism |
|||||||
✅ |
✅ |
Metabolism |
|||||||
✅ |
✅ |
Metabolism |
|||||||
DBH |
✅ |
Efficacy |
NM_000787.4 was used as the main transcript. |
||||||
✅ |
✅ |
✅ |
✅ |
Excretion |
|||||
DRD2 |
✅ |
Toxicity |
NM_000795.4 was used as the main transcript. |
||||||
F2 |
✅ |
Other |
NM_000506.5 was used as the main transcript. |
||||||
✅ |
✅ |
Other |
|||||||
✅ |
✅ |
✅ |
Disease |
G6PD is located on X chromosome. |
|||||
GRIK1 |
✅ |
Metabolism |
NM_001330994.2 was used as the main transcript. |
||||||
GRIK4 |
✅ |
Efficacy |
NM_014619.5 was used as the main transcript. |
||||||
GRIN2B |
✅ |
Other |
NM_000834.5 was used as the main transcript. |
||||||
✅ |
✅ |
Metabolism |
|||||||
GSTP1 |
✅ |
Metabolism |
|||||||
✅ |
Metabolism |
GSTT1 is located on different contigs between GRCh37 and GRCh38. |
|||||||
HTR1A |
✅ |
Efficacy |
NM_000524.4 was used as the main transcript. |
||||||
HTR2A |
✅ |
Efficacy |
NM_000524.4 was used as the main transcript. |
||||||
✅ |
✅ |
Other |
|||||||
IFNL4 |
✅ |
Other |
NR_074079.1 was used as the main transcript. |
||||||
ITGB3 |
✅ |
Efficacy |
NM_000212.3 was used as the main transcript. |
||||||
ITPA |
✅ |
Other |
NM_033453.4 was used as the main transcript. |
||||||
✅ |
✅ |
Disease |
|||||||
MTHFR |
✅ |
Metabolism |
|||||||
NAT1 |
✅ |
Metabolism |
|||||||
NAT2 |
✅ |
Metabolism |
|||||||
✅ |
✅ |
✅ |
✅ |
Metabolism |
|||||
OPRK1 |
✅ |
Other |
NM_000912.5 was used as the main transcript. |
||||||
OPRM1 |
✅ |
Other |
NM_000914.5 was used as the main transcript. |
||||||
✅ |
✅ |
Disease |
|||||||
✅ |
✅ |
Other |
|||||||
RARG |
✅ |
Toxicity |
NM_000966.6 was used as the main transcript. |
||||||
✅ |
✅ |
✅ |
Disease |
||||||
SLC6A4 |
✅ |
Other |
NM_001045.6 was used as the main transcript. |
||||||
SLC15A2 |
✅ |
Excretion |
|||||||
✅ |
✅ |
Excretion |
|||||||
SLC28A3 |
✅ |
✅ |
Excretion |
NM_001199633.2 was used as the main transcript. |
|||||
SLC47A2 |
✅ |
Other |
NM_001099646.3 was used as the main transcript. |
||||||
✅ |
✅ |
✅ |
✅ |
Absorption |
|||||
SLCO1B3 |
✅ |
Absorption |
|||||||
SLCO2B1 |
✅ |
Absorption |
|||||||
✅ |
✅ |
Metabolism |
|||||||
✅ |
✅ |
Other |
|||||||
✅ |
✅ |
✅ |
Metabolism |
||||||
✅ |
✅ |
✅ |
Excretion |
||||||
✅ |
✅ |
Excretion |
|||||||
UGT1A6 |
✅ |
Excretion |
NM_001072.4 was used as the main transcript. |
||||||
UGT2B7 |
✅ |
Excretion |
|||||||
✅ |
✅ |
Excretion |
|||||||
✅ |
Excretion |
||||||||
VKORC1 |
✅ |
✅ |
Target |
||||||
XPC |
✅ |
Other |
ABCG2
Phenotype summary for ABCG2
Diplotype-phenotype mapping is used for phenotype prediction.
Phenotype |
Example |
Priority |
|---|---|---|
Normal Function |
Reference/Reference |
Normal/Routine/Low Risk |
Decreased Function |
Reference/rs2231142 |
Abnormal/Priority/High Risk |
Poor Function |
rs2231142/rs2231142 |
Abnormal/Priority/High Risk |
Recommendations for ABCG2
Rosuvastatin
“Prescribe ≤20mg as a starting dose and adjust doses of rosuvastatin based on disease-specific and specific population guidelines for patients who are SLCO1B1 or ABCG2 poor function phenotype. If dose >20mg needed for desired efficacy, consider combination therapy (i.e. rosuvastatin plus non-statin guideline directed medical therapy). Patients with both ABCG2 poor function and SLCO1B1 poor/decreased function should be prescribed ≤10mg as a starting dose.” (Source: PharmGKB)
Resources for ABCG2
CACNA1S
Phenotype summary for CACNA1S
Diplotype-phenotype mapping is used for phenotype prediction.
Phenotype
Example
Priority
Uncertain Susceptibility
Reference/Reference
Normal Risk
Malignant Hyperthermia Susceptibility
Reference/c.520C>T
Abnormal/Priority/High Risk
Recommendations for CACNA1S
Desflurane
“The CPIC Dosing Guideline recommends that halogenated volatile anesthetics uch as desflurane, enflurane, halothane, isoflurane, methoxyflurane, sevoflurane and the depolarizing muscle relaxants succinylcholine are relatively contraindicated in persons with malignant hyperthermia susceptibility (MHS). See full guideline for disclaimers, further details and supporting evidence.” (Source: PharmGKB)
Enflurane
“The CPIC Dosing Guideline recommends that halogenated volatile anesthetics such as desflurane, enflurane, halothane, isoflurane, methoxyflurane, sevoflurane and the depolarizing muscle relaxants succinylcholine are relatively contraindicated in persons with malignant hyperthermia susceptibility (MHS). See full guideline for disclaimers, further details and supporting evidence.” (Source: PharmGKB)
Halothane
“The CPIC Dosing Guideline recommends that halogenated volatile anesthetics such as desflurane, enflurane, halothane, isoflurane, methoxyflurane, sevoflurane and the depolarizing muscle relaxants succinylcholine are relatively contraindicated in persons with malignant hyperthermia susceptibility (MHS). See full guideline for disclaimers, further details and supporting evidence.” (Source: PharmGKB)
Isoflurane
“The CPIC Dosing Guideline recommends that halogenated volatile anesthetics such as desflurane, enflurane, halothane, isoflurane, methoxyflurane, sevoflurane and the depolarizing muscle relaxants succinylcholine are relatively contraindicated in persons with malignant hyperthermia susceptibility (MHS). See full guideline for disclaimers, further details and supporting evidence.” (Source: PharmGKB)
Methoxyflurane
“The CPIC Dosing Guideline recommends that halogenated volatile anesthetics such as desflurane, enflurane, halothane, isoflurane, methoxyflurane, sevoflurane and the depolarizing muscle relaxants succinylcholine are relatively contraindicated in persons with malignant hyperthermia susceptibility (MHS). See full guideline for disclaimers, further details and supporting evidence.” (Source: PharmGKB)
Sevoflurane
“The CPIC Dosing Guideline recommends that halogenated volatile anesthetics such as desflurane, enflurane, halothane, isoflurane, methoxyflurane, sevoflurane and the depolarizing muscle relaxants succinylcholine are relatively contraindicated in persons with malignant hyperthermia susceptibility (MHS). See full guideline for disclaimers, further details and supporting evidence.” (Source: PharmGKB)
Succinylcholine
“The CPIC Dosing Guideline recommends that halogenated volatile anesthetics such as desflurane, enflurane, halothane, isoflurane, methoxyflurane, sevoflurane and the depolarizing muscle relaxants succinylcholine are relatively contraindicated in persons with malignant hyperthermia susceptibility (MHS). See full guideline for disclaimers, further details and supporting evidence.” (Source: PharmGKB)
Resources for CACNA1S
CFTR
Phenotype summary for CFTR
Diplotype-phenotype mapping is used for phenotype prediction.
Phenotype
Example
Priority
Favorable Response
Reference/G551D
None
Unfavorable Response
F508del/F508del
None
Indeterminate
Reference/F508del
None
Recommendations for CFTR
Ivacaftor
“Ivacaftor treatment is recommended only in cystic fibrosis (CF) patients that are either homozygous or heterozygous for certain CFTR variants. See full guideline for disclaimers, further details and supporting evidence.” (Source: PharmGKB)
Resources for CFTR
CYP1A1
Resources for CYP1A1
CYP1A2
Resources for CYP1A2
CYP1B1
Resources for CYP1B1
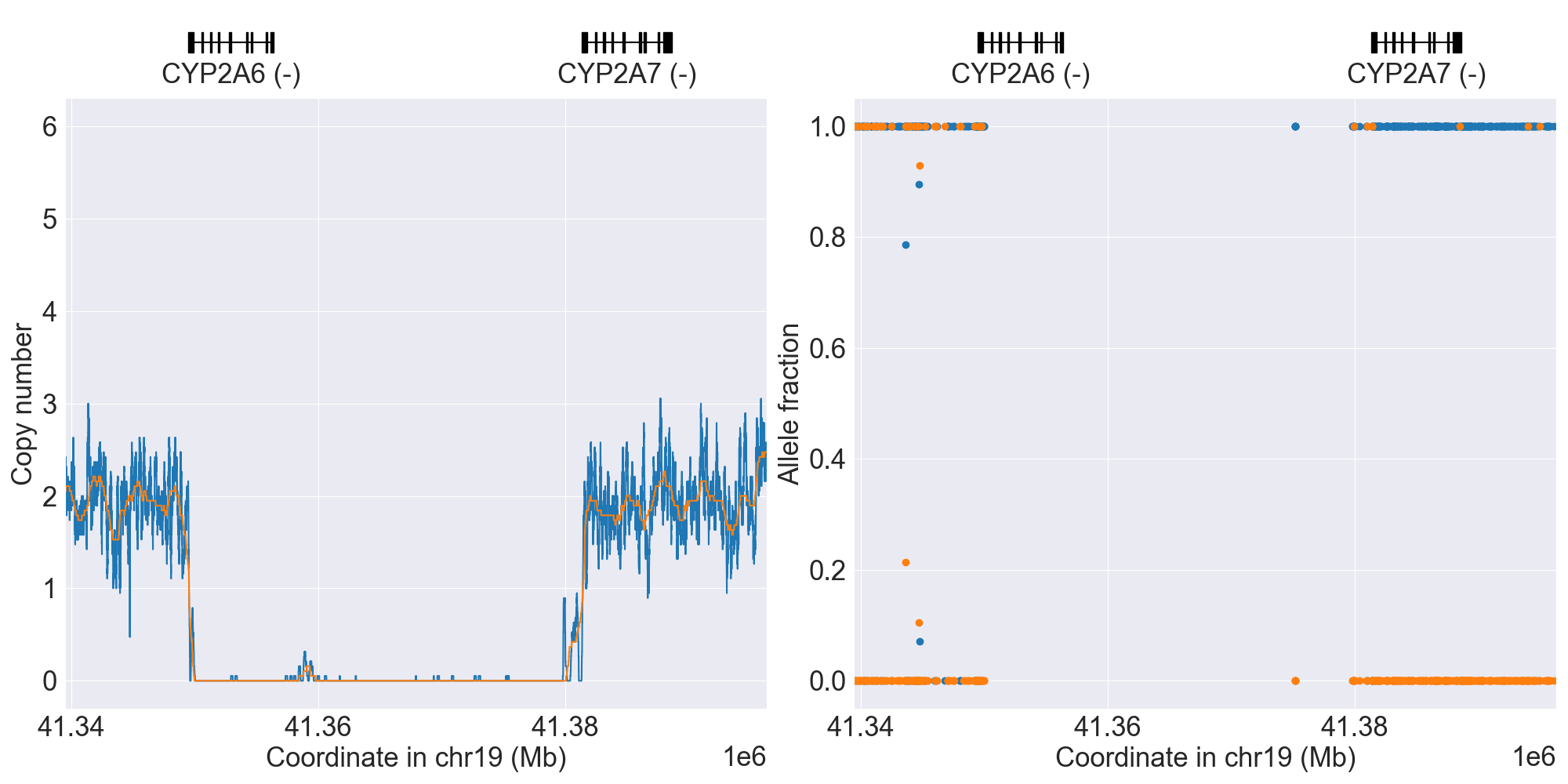
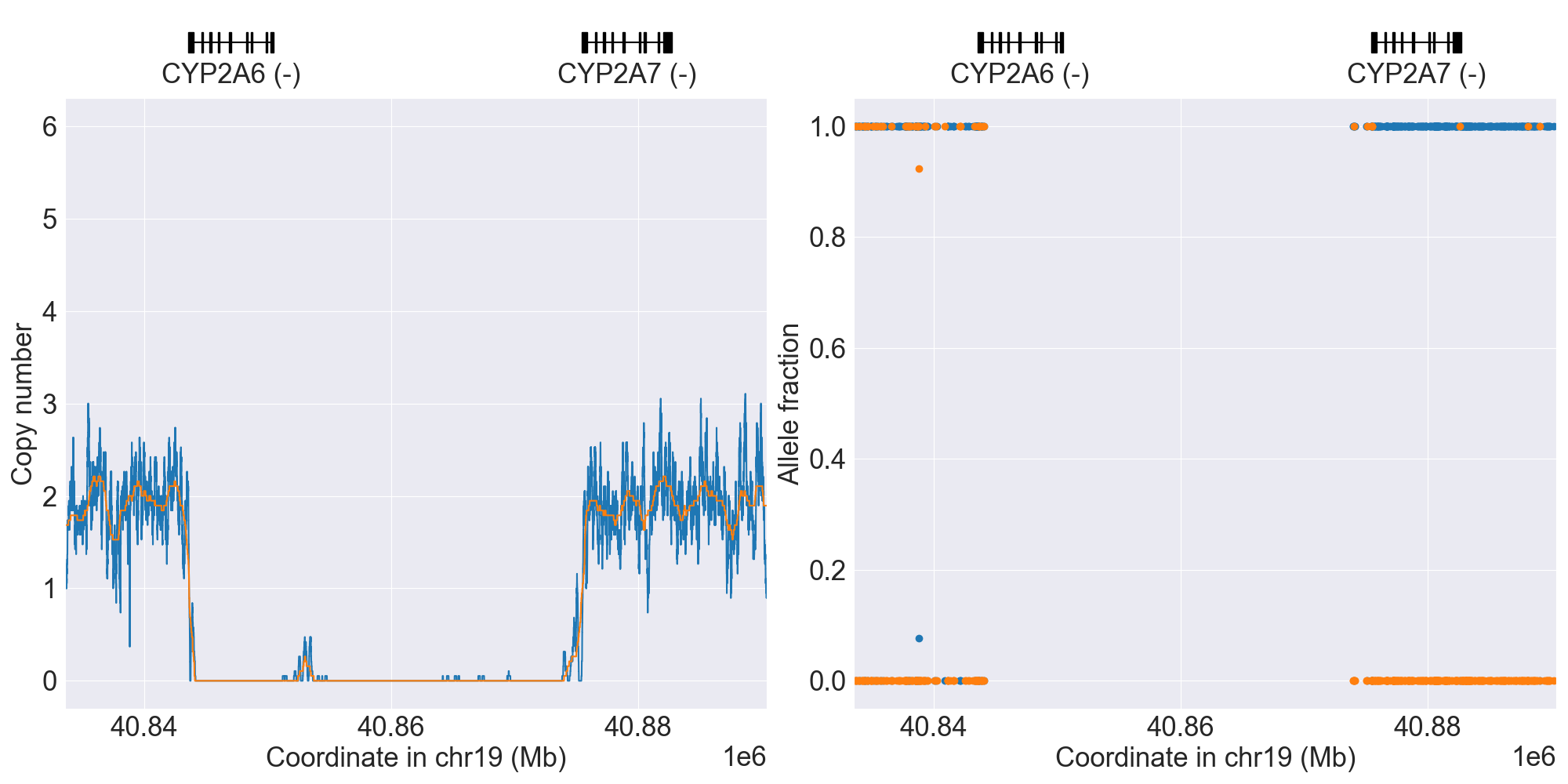
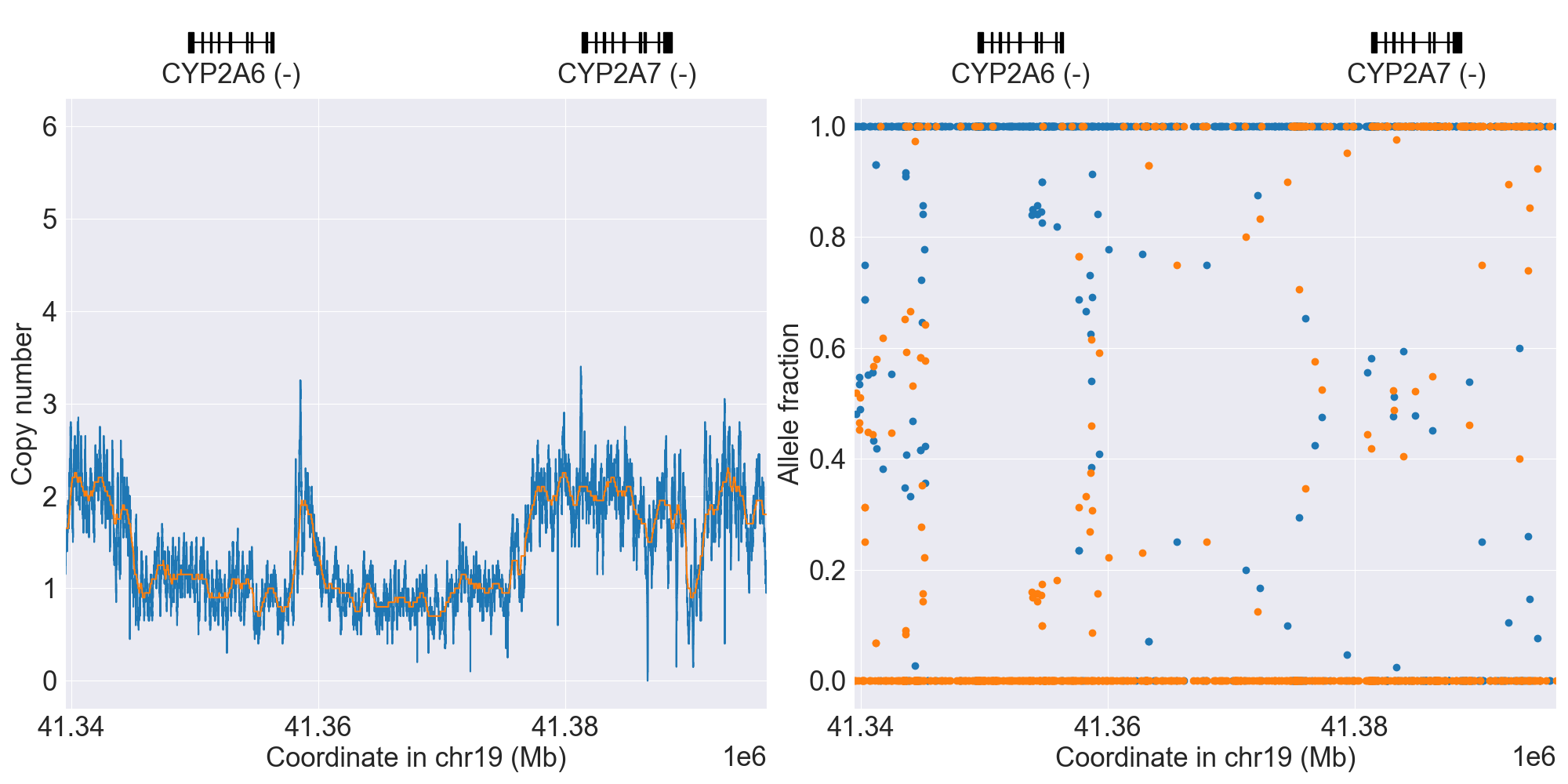
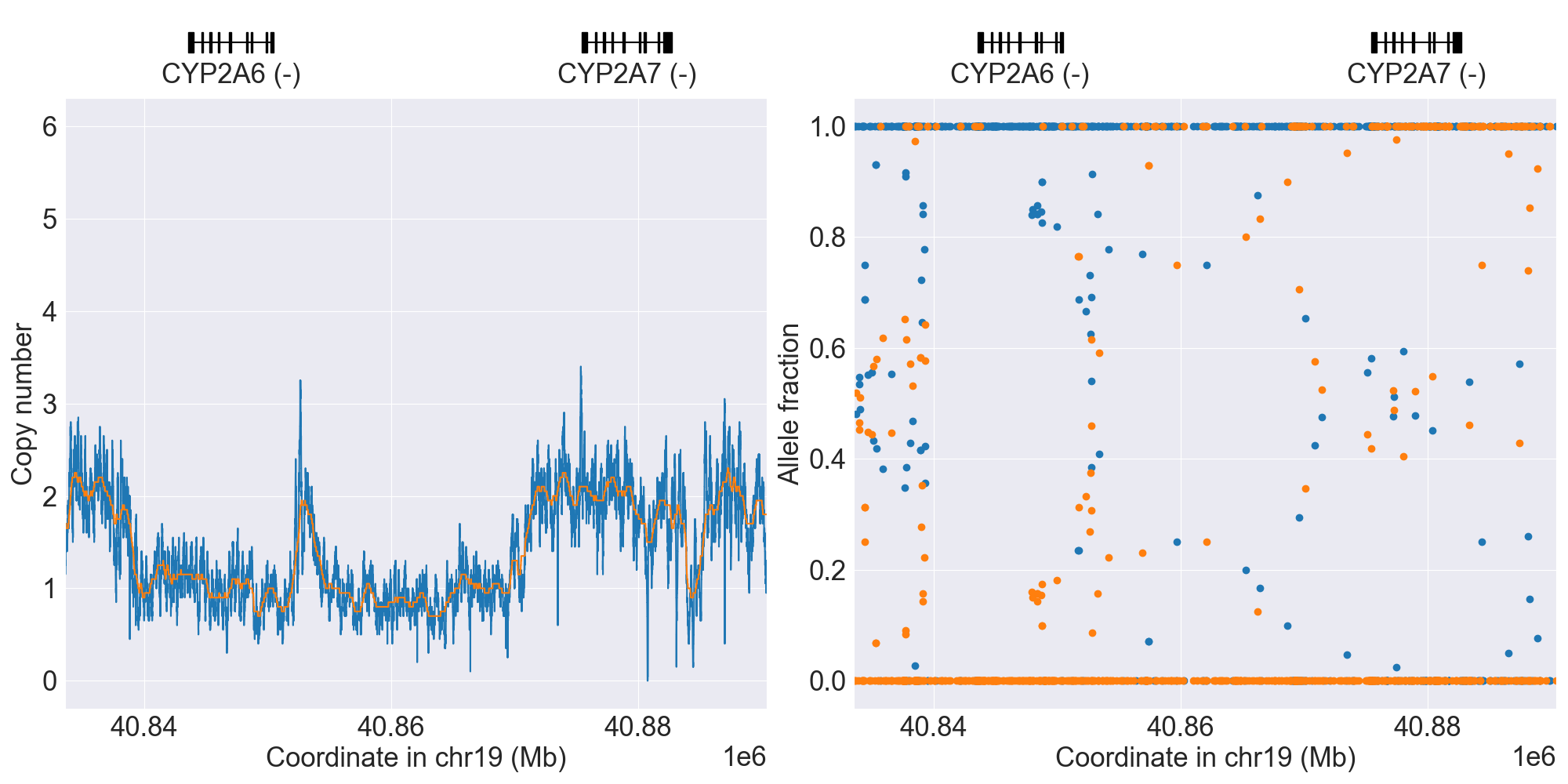
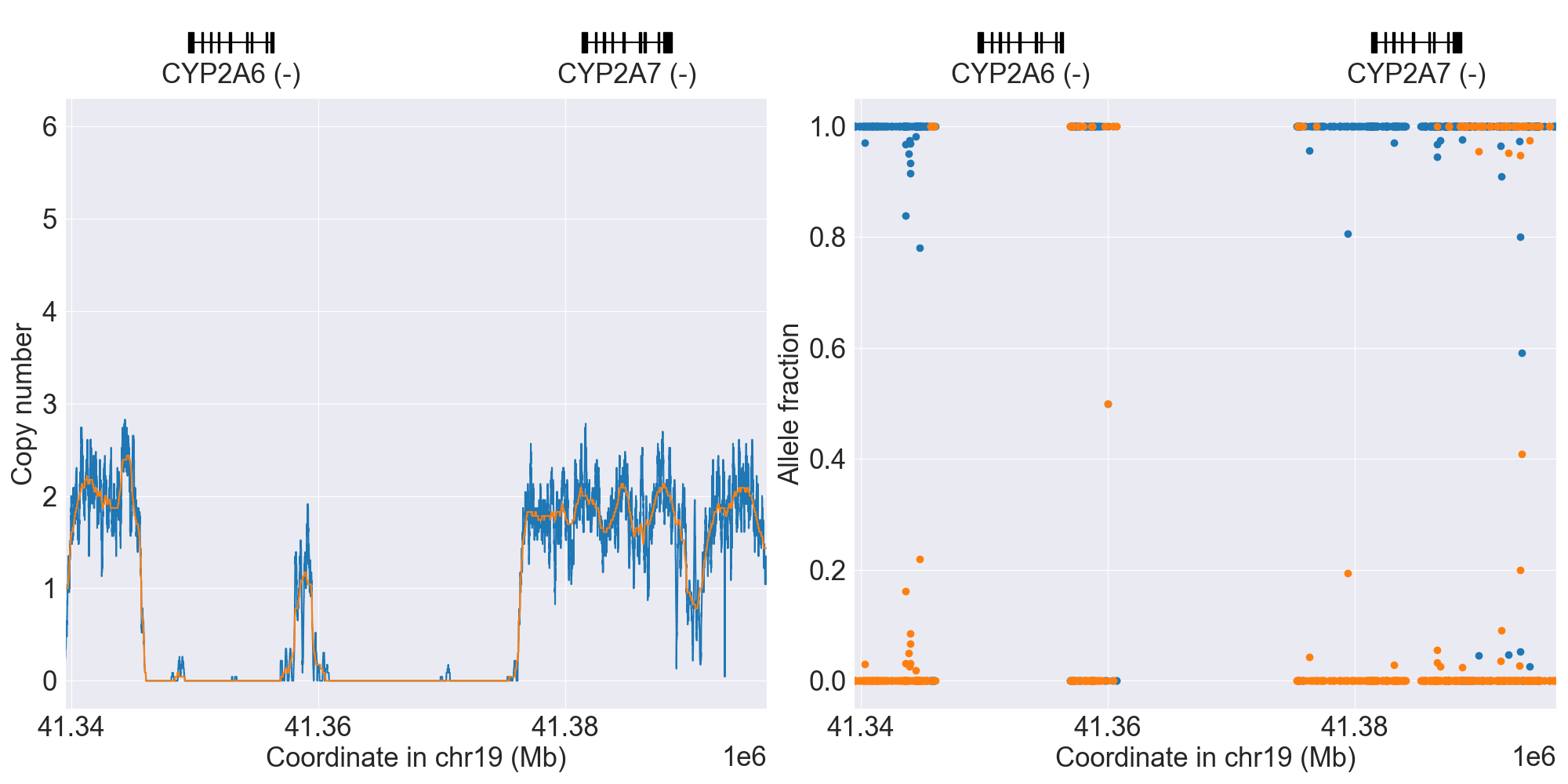
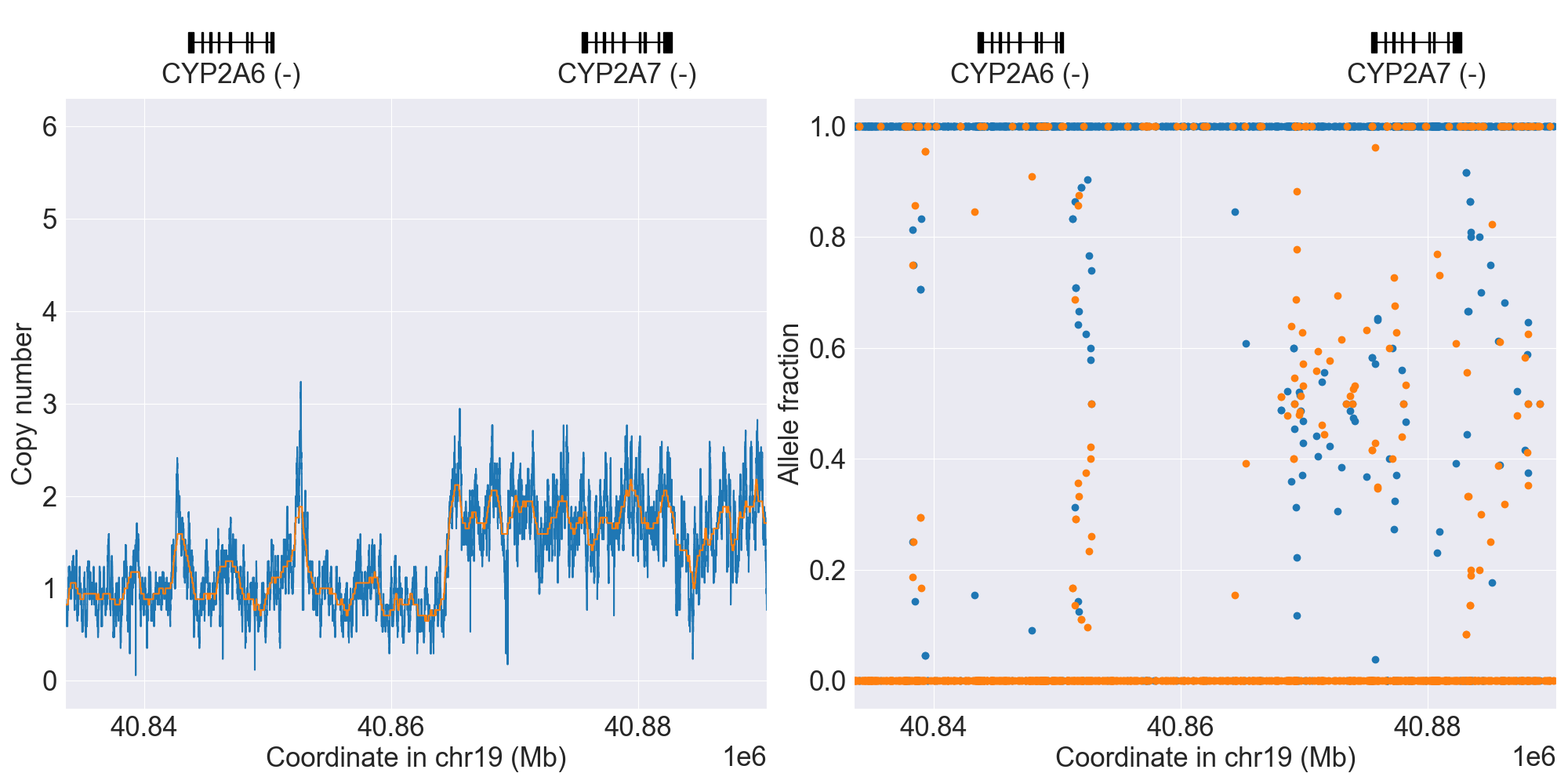
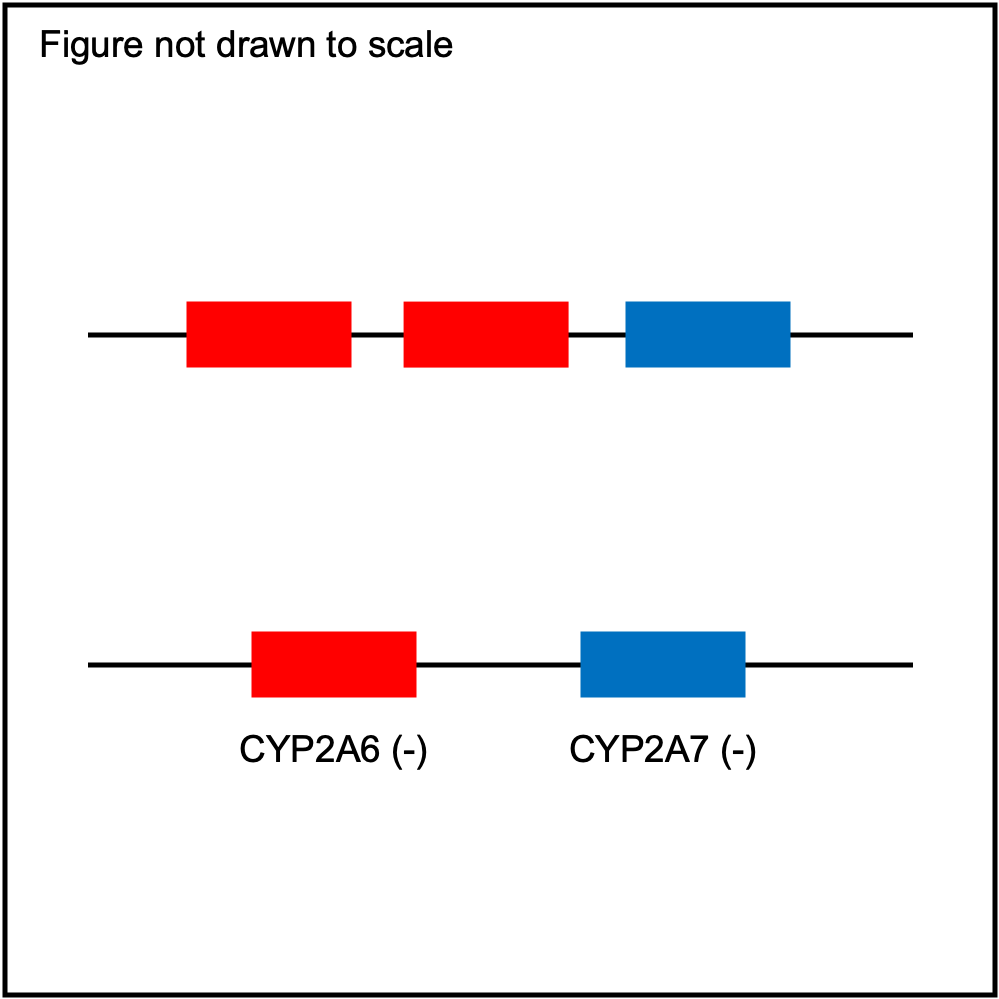
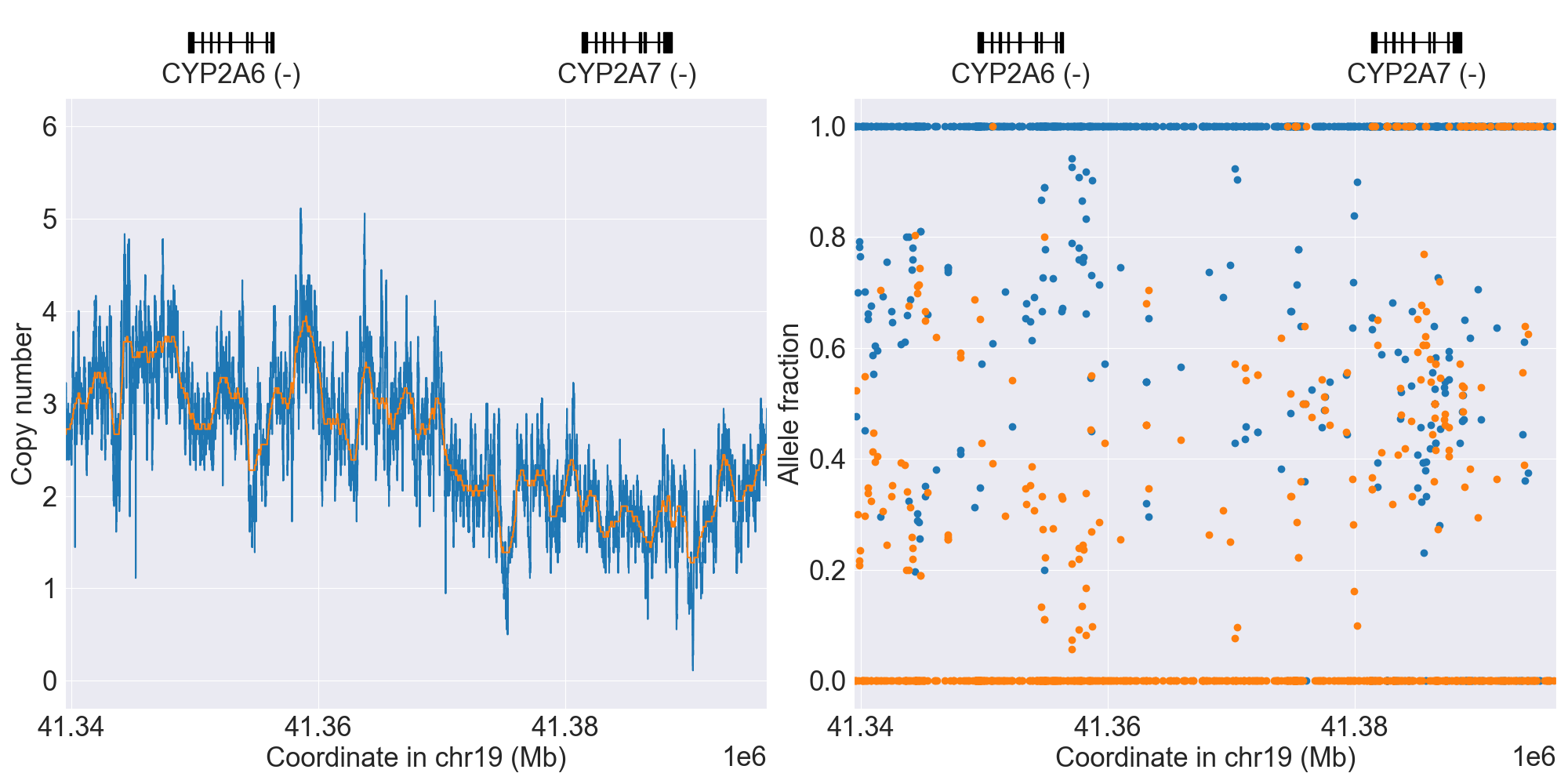
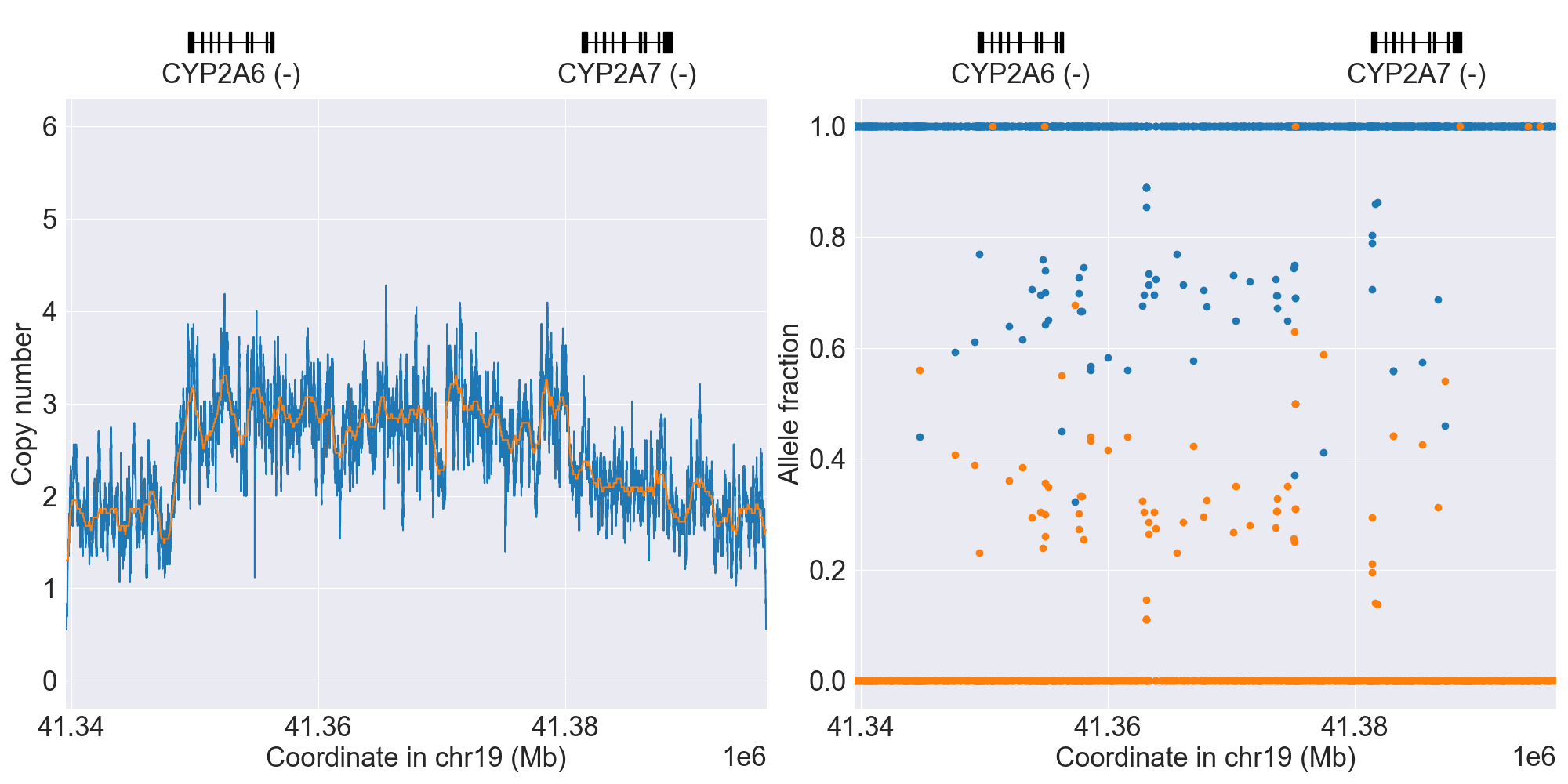
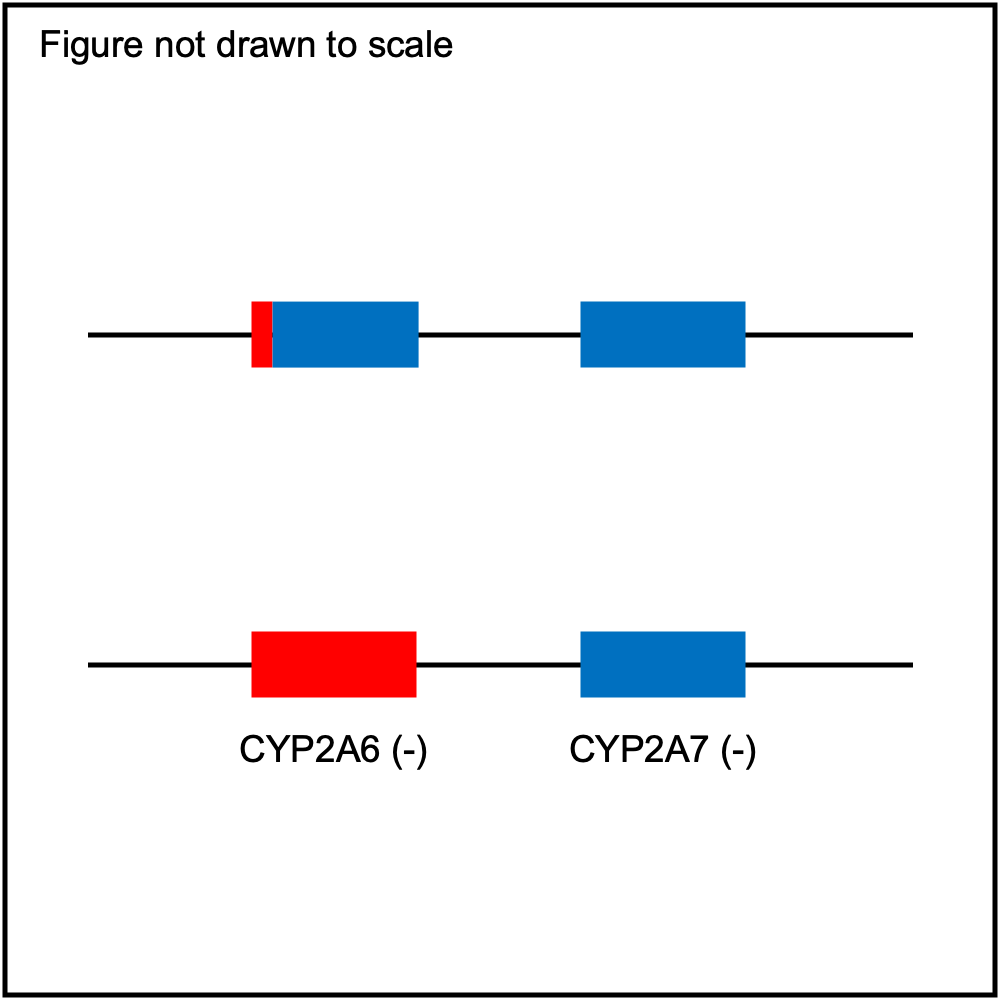
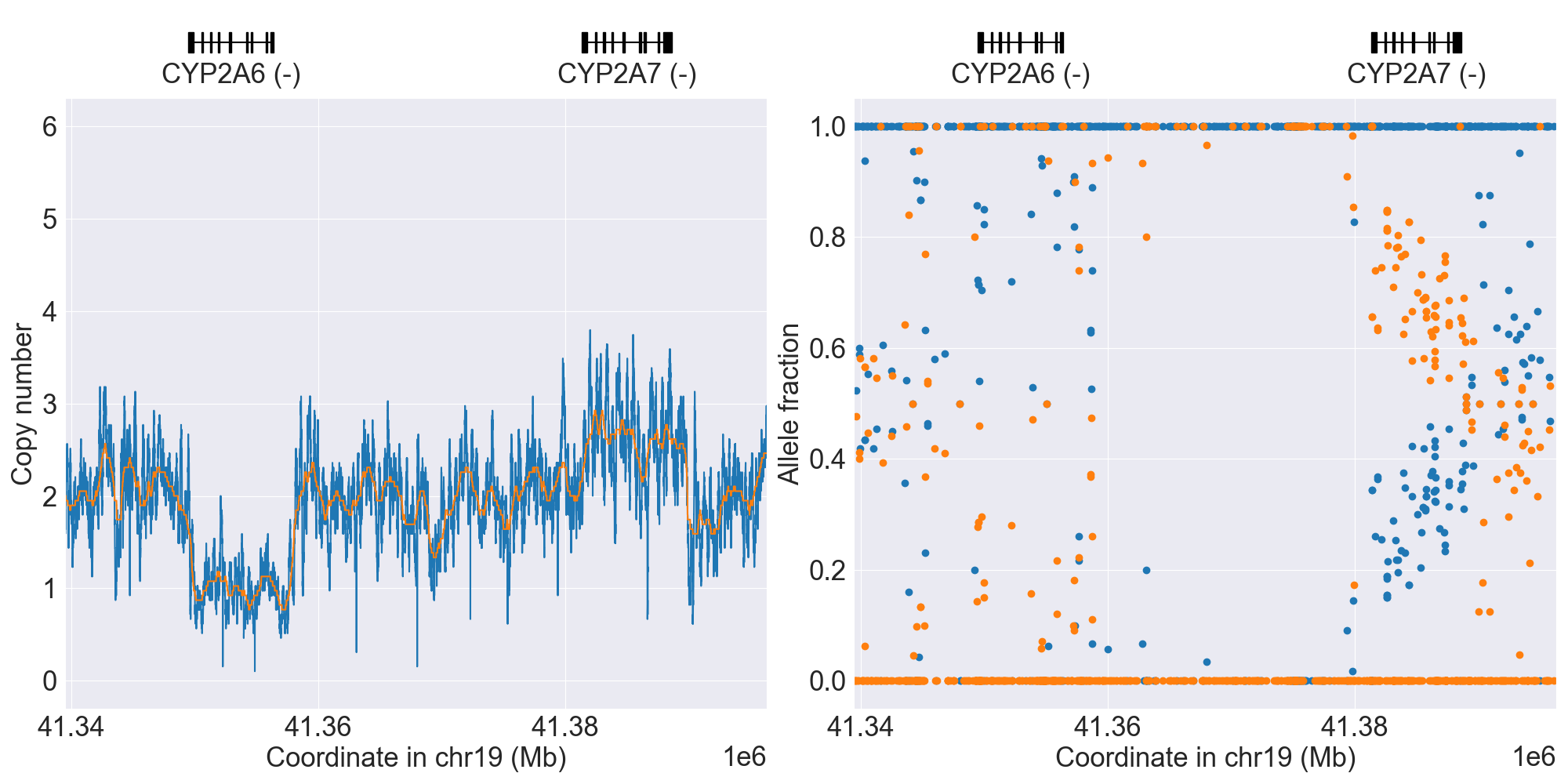
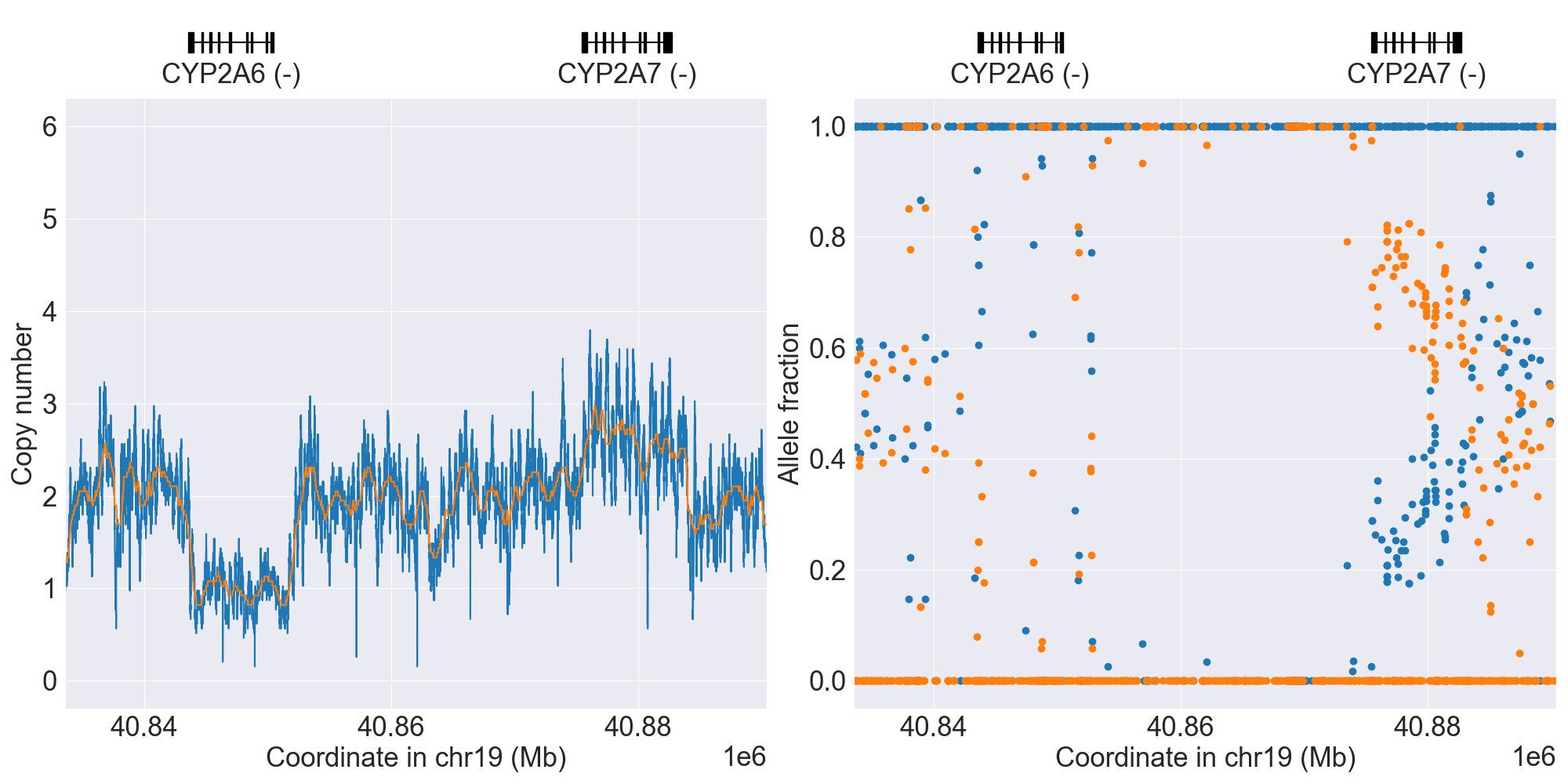
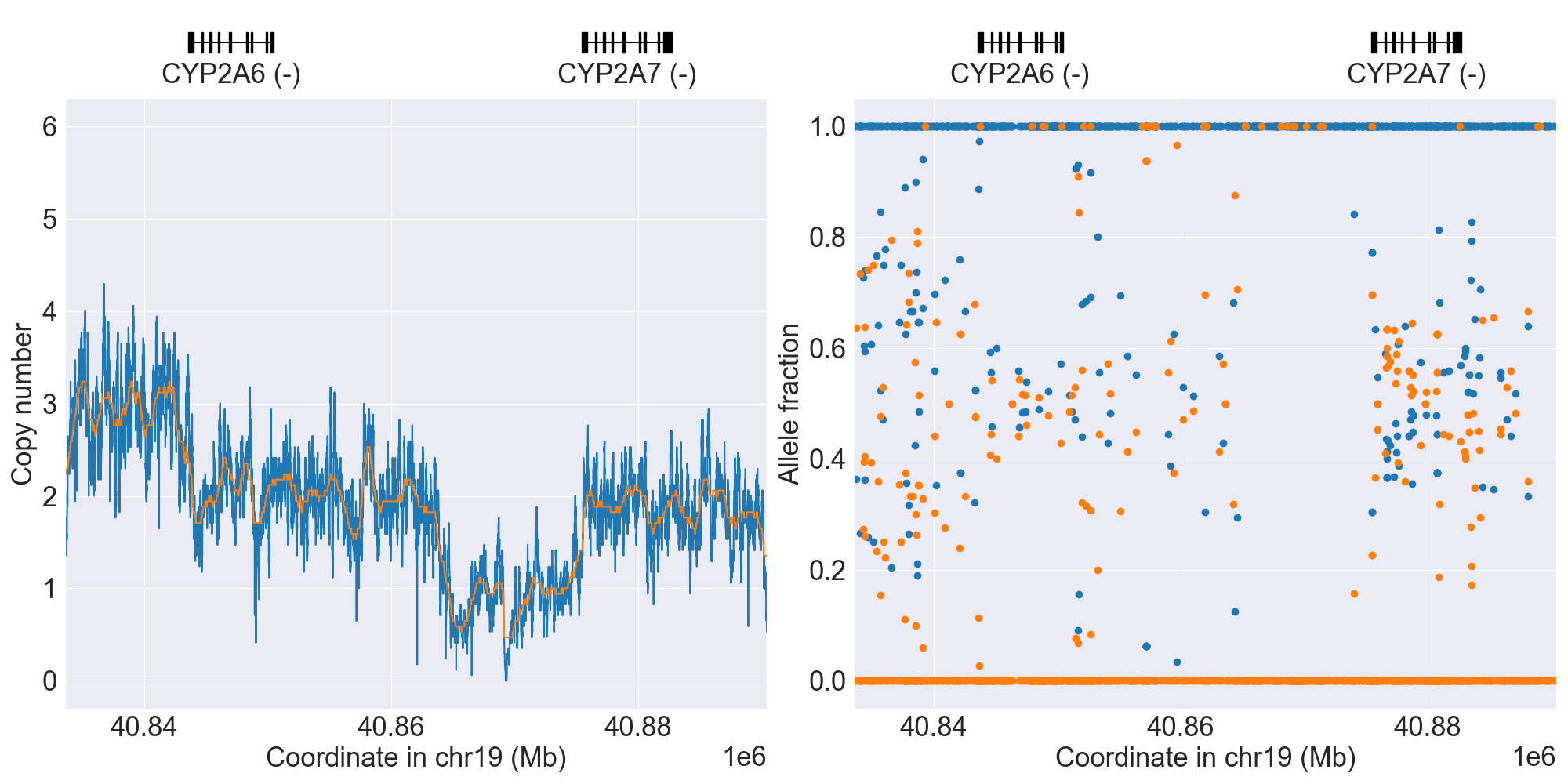
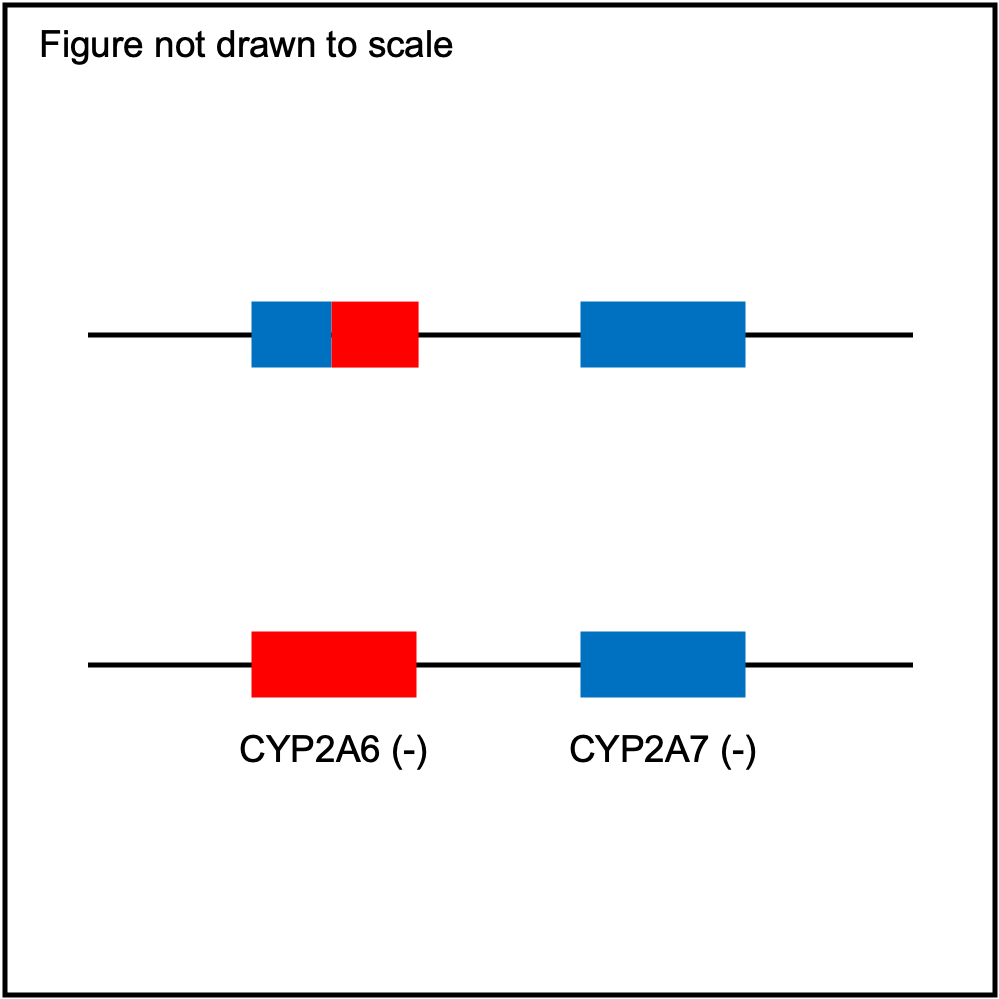
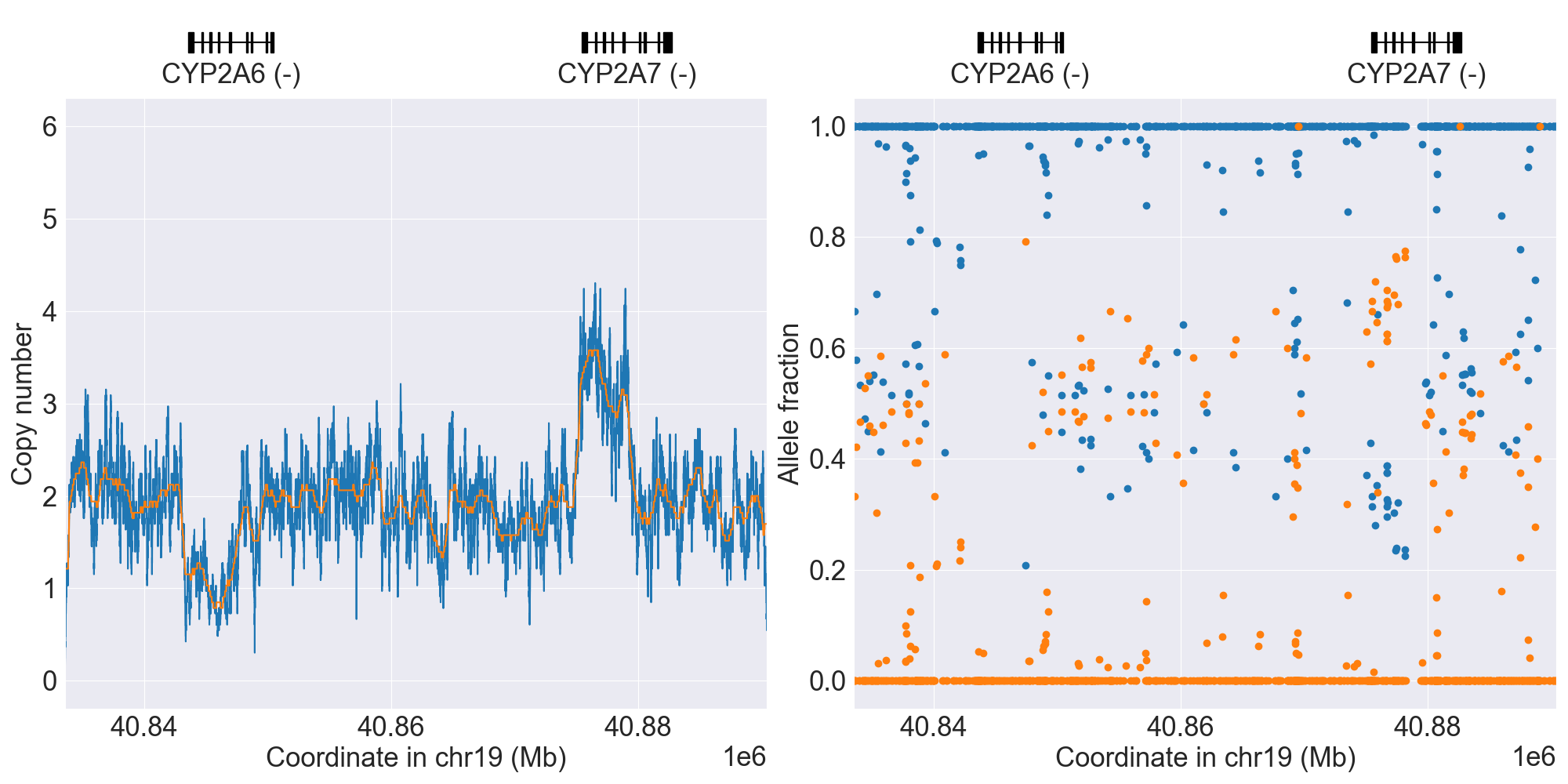
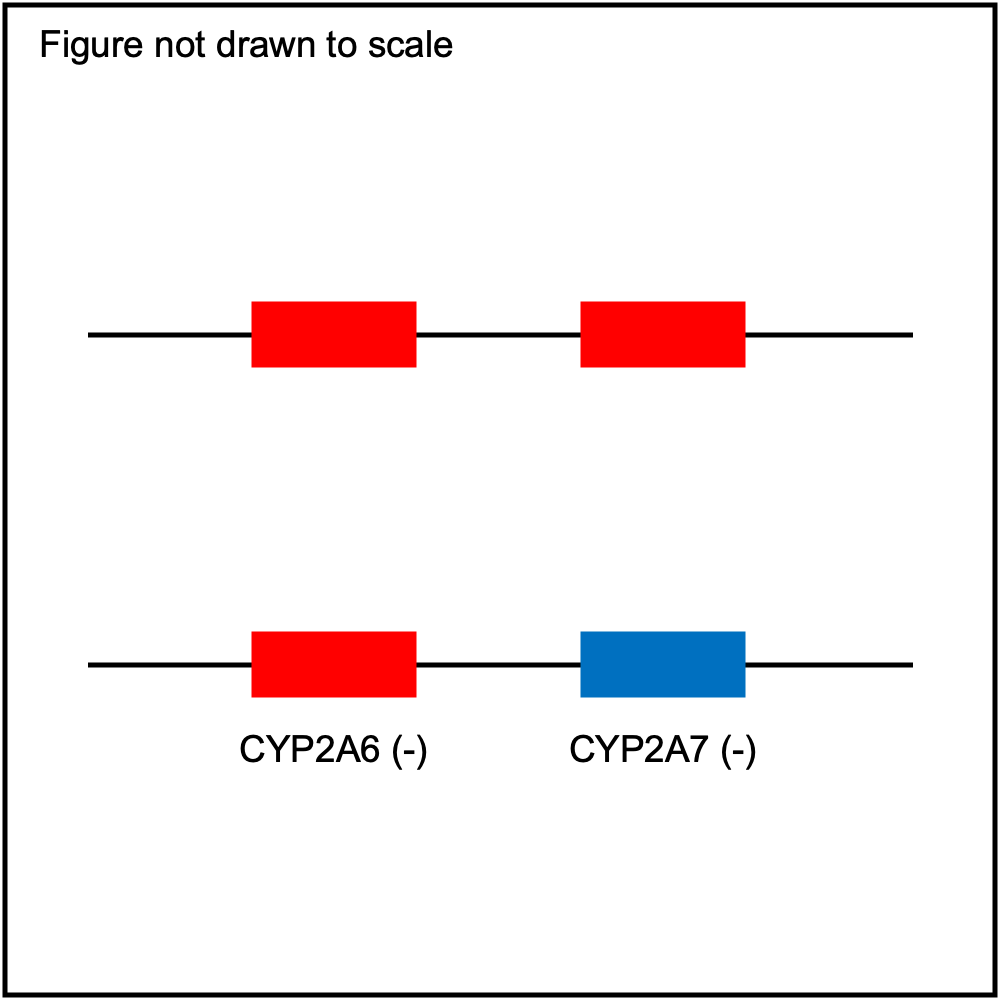
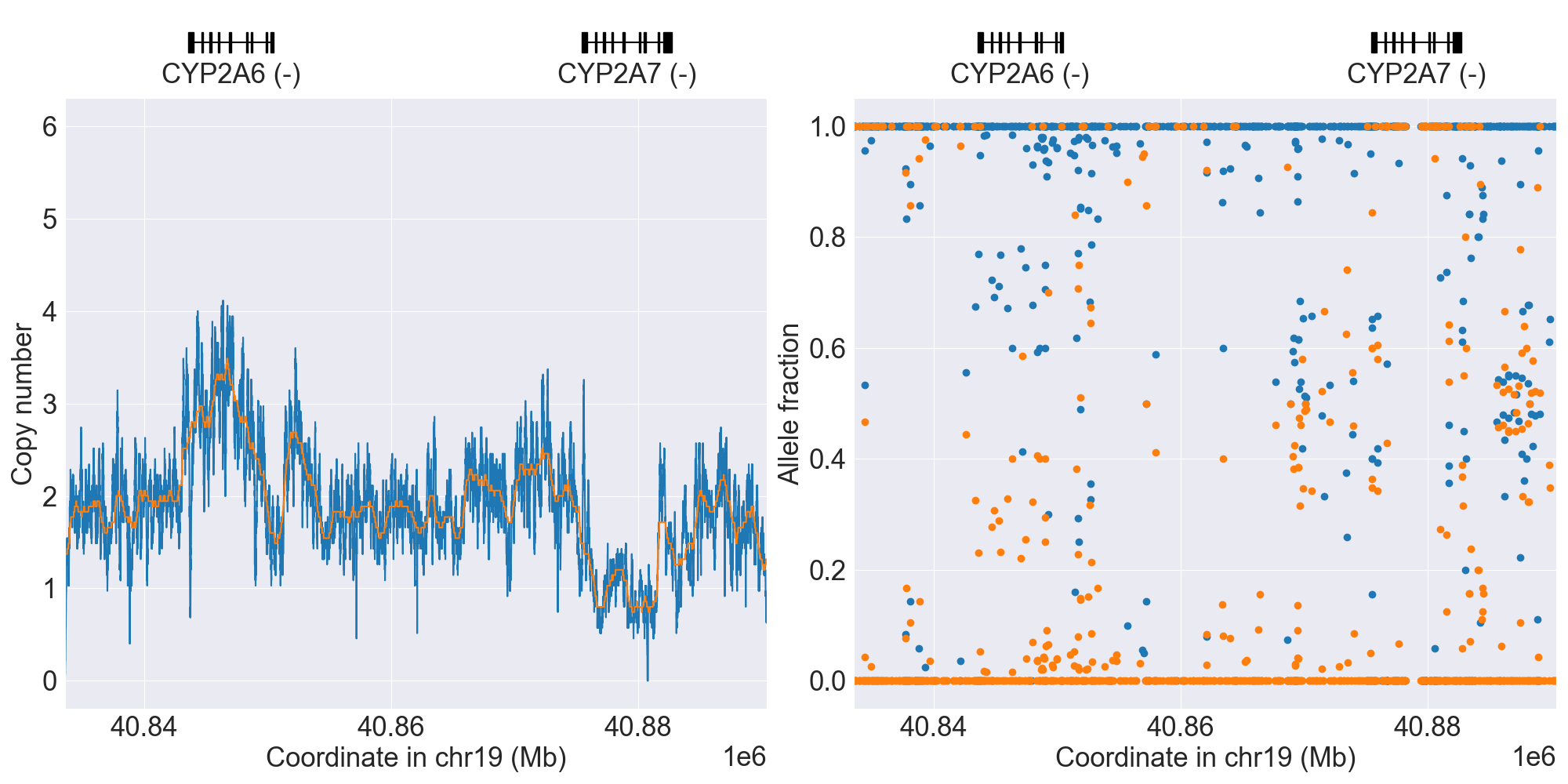
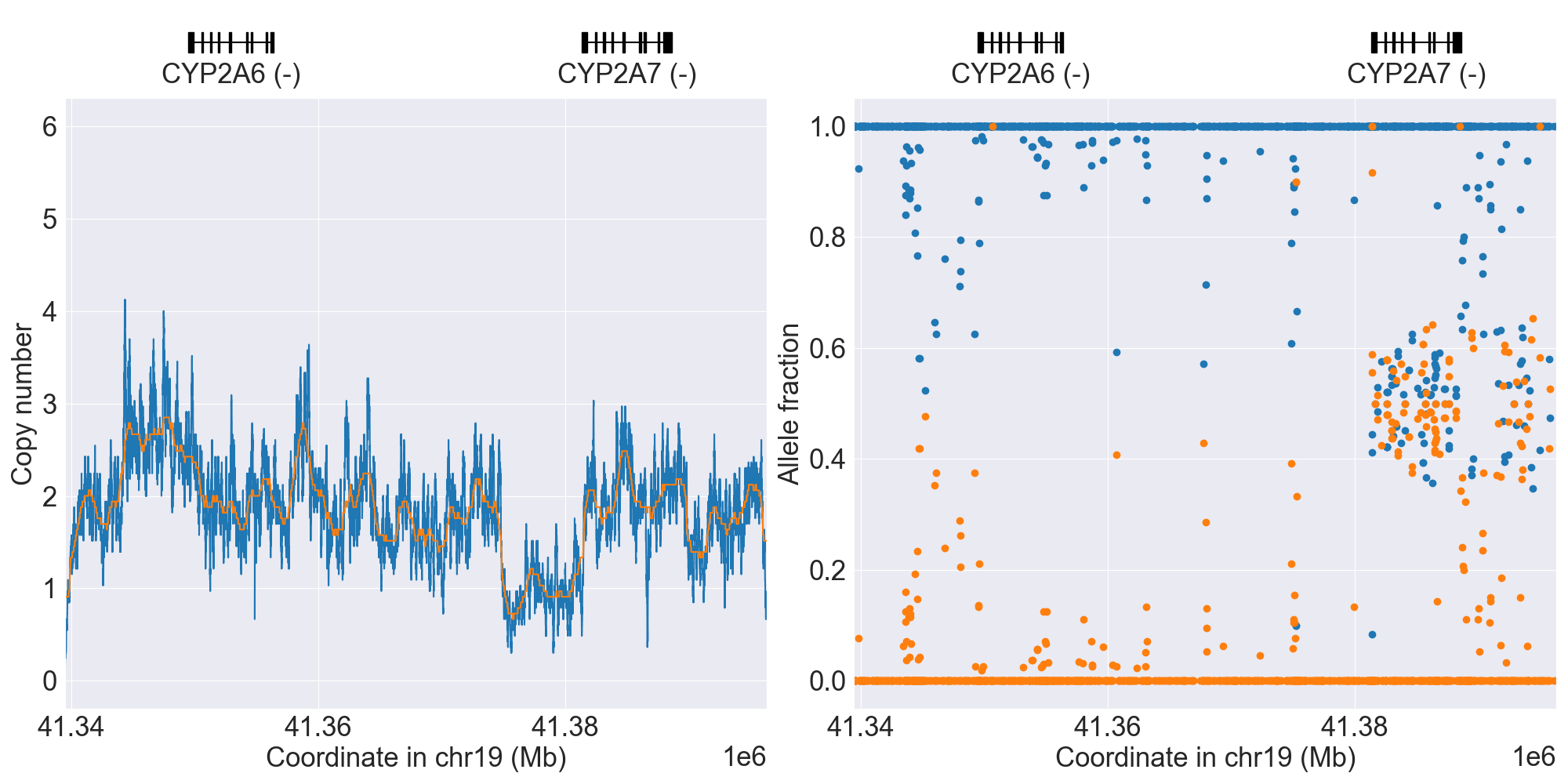
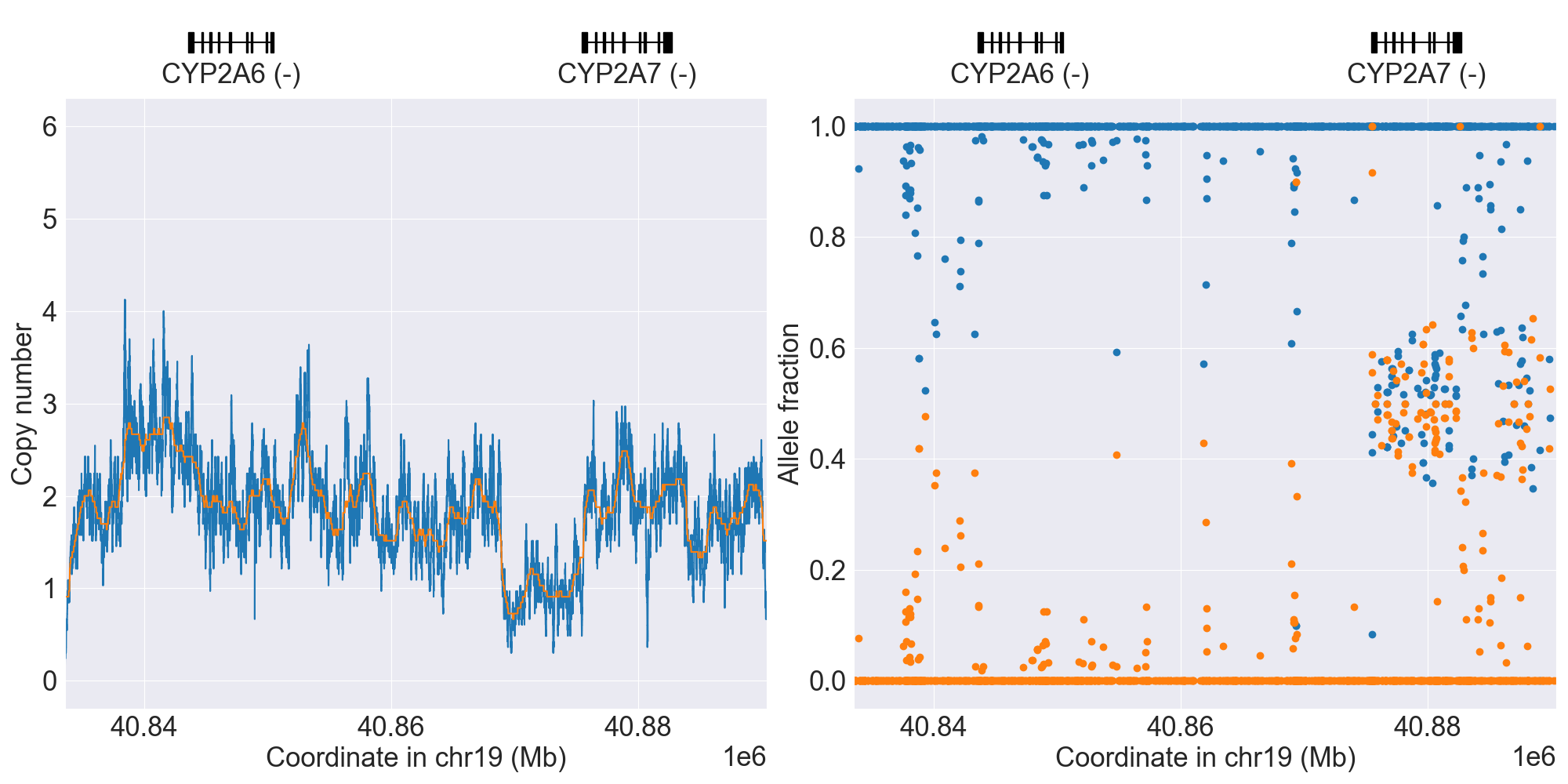
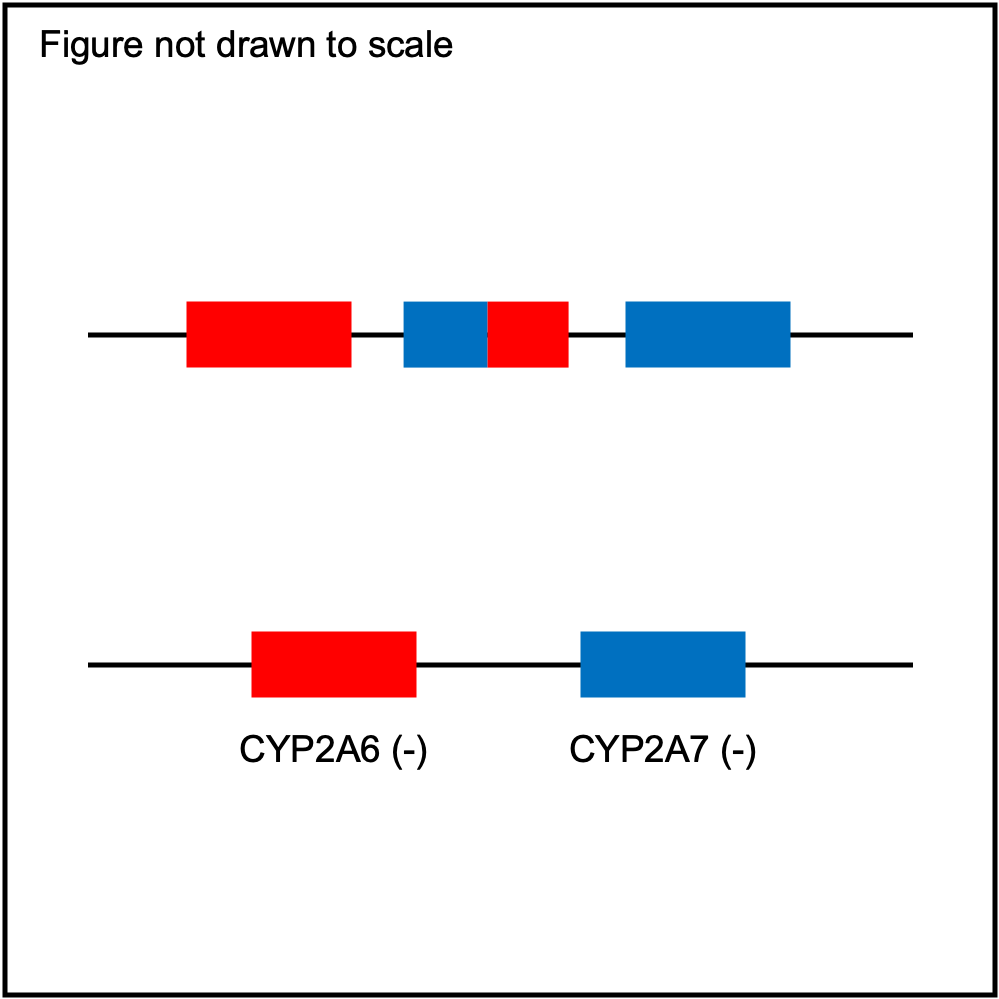
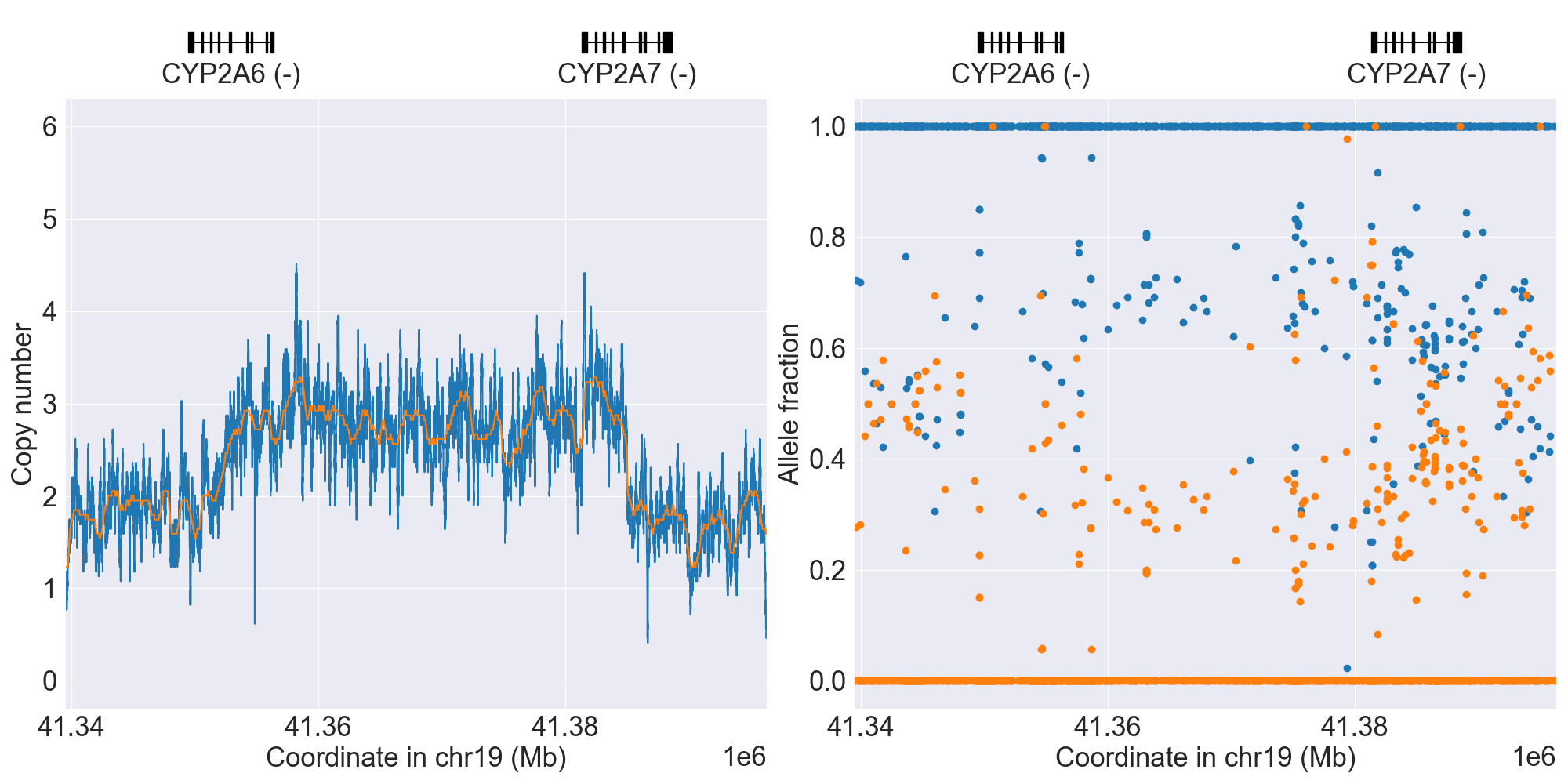
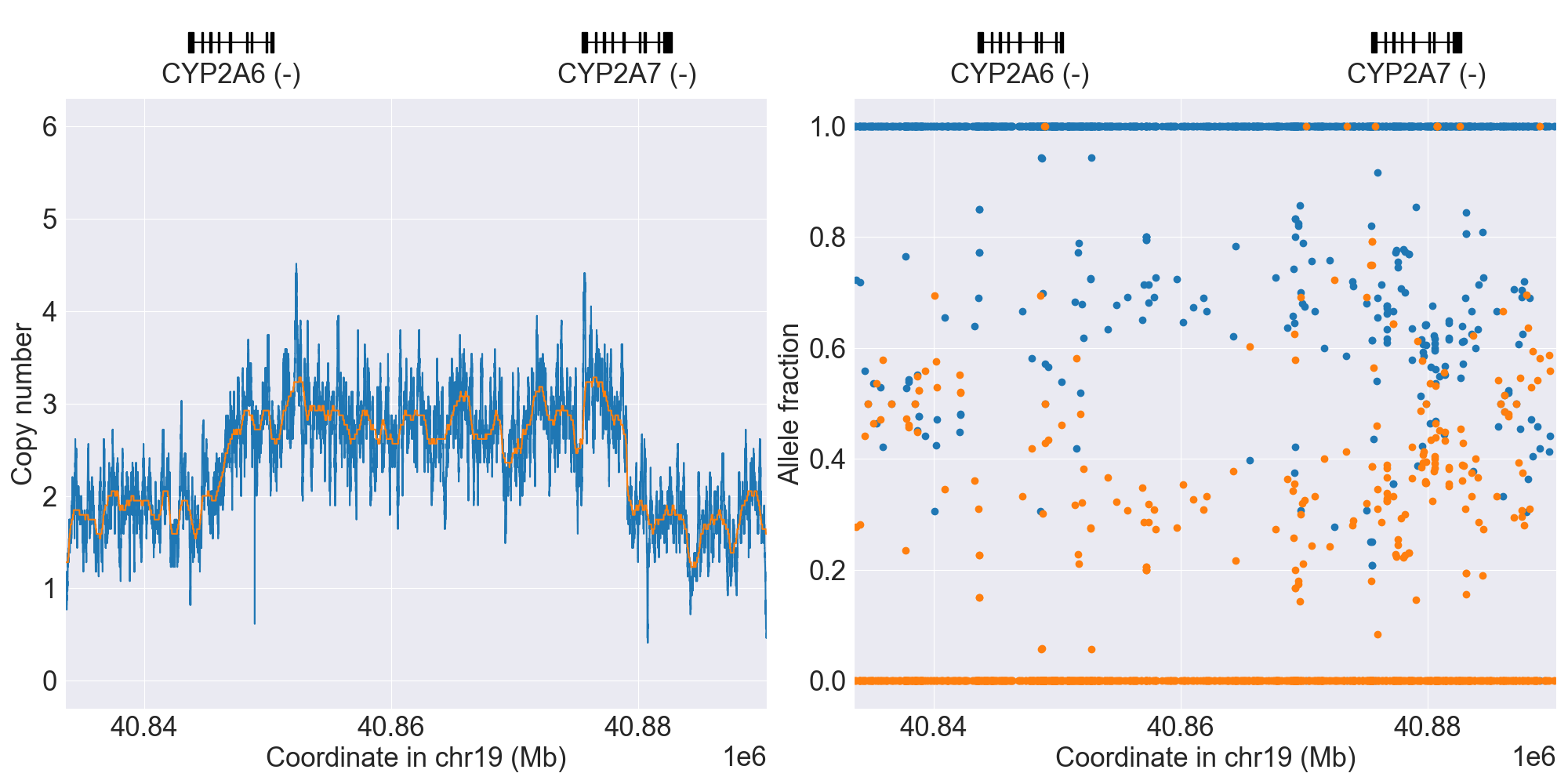
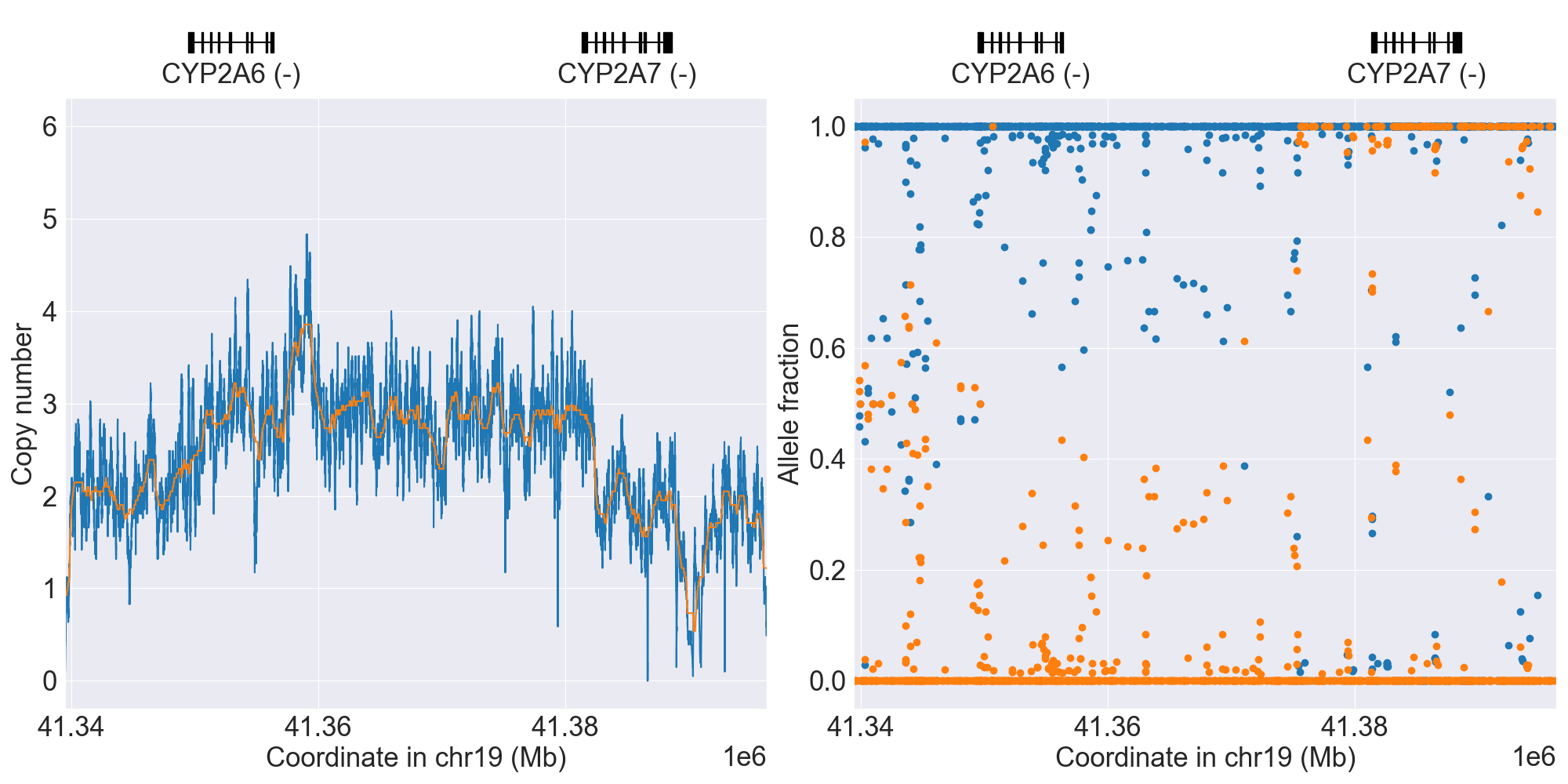
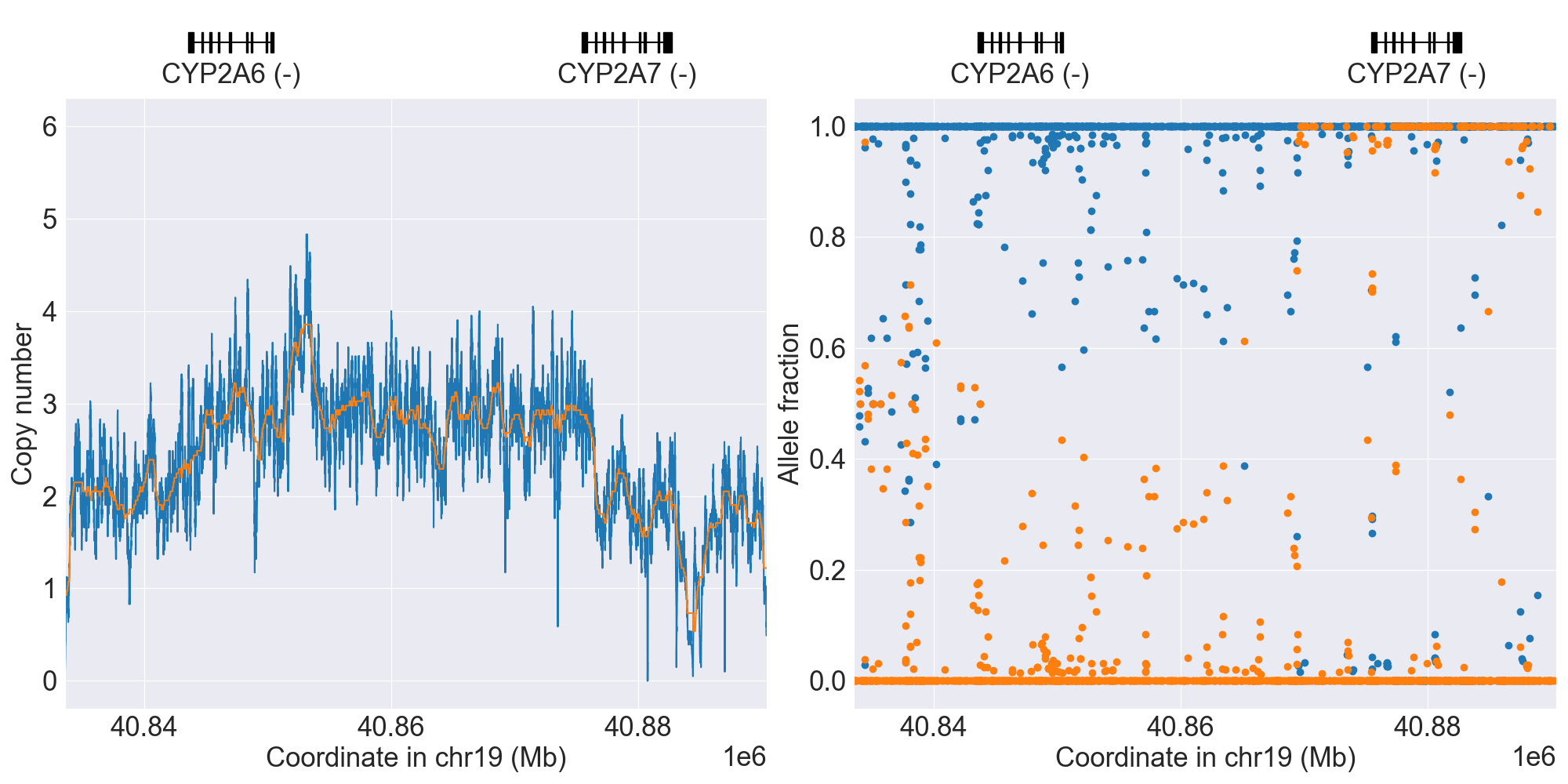
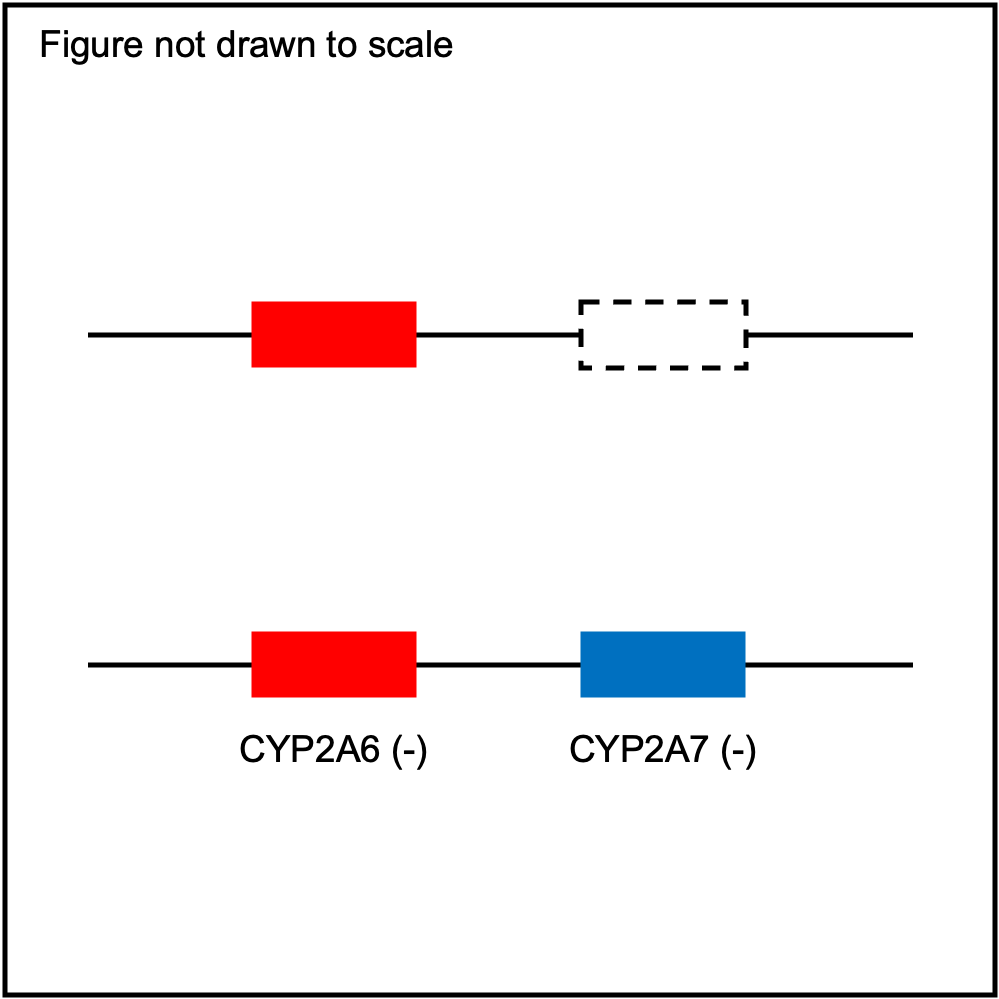
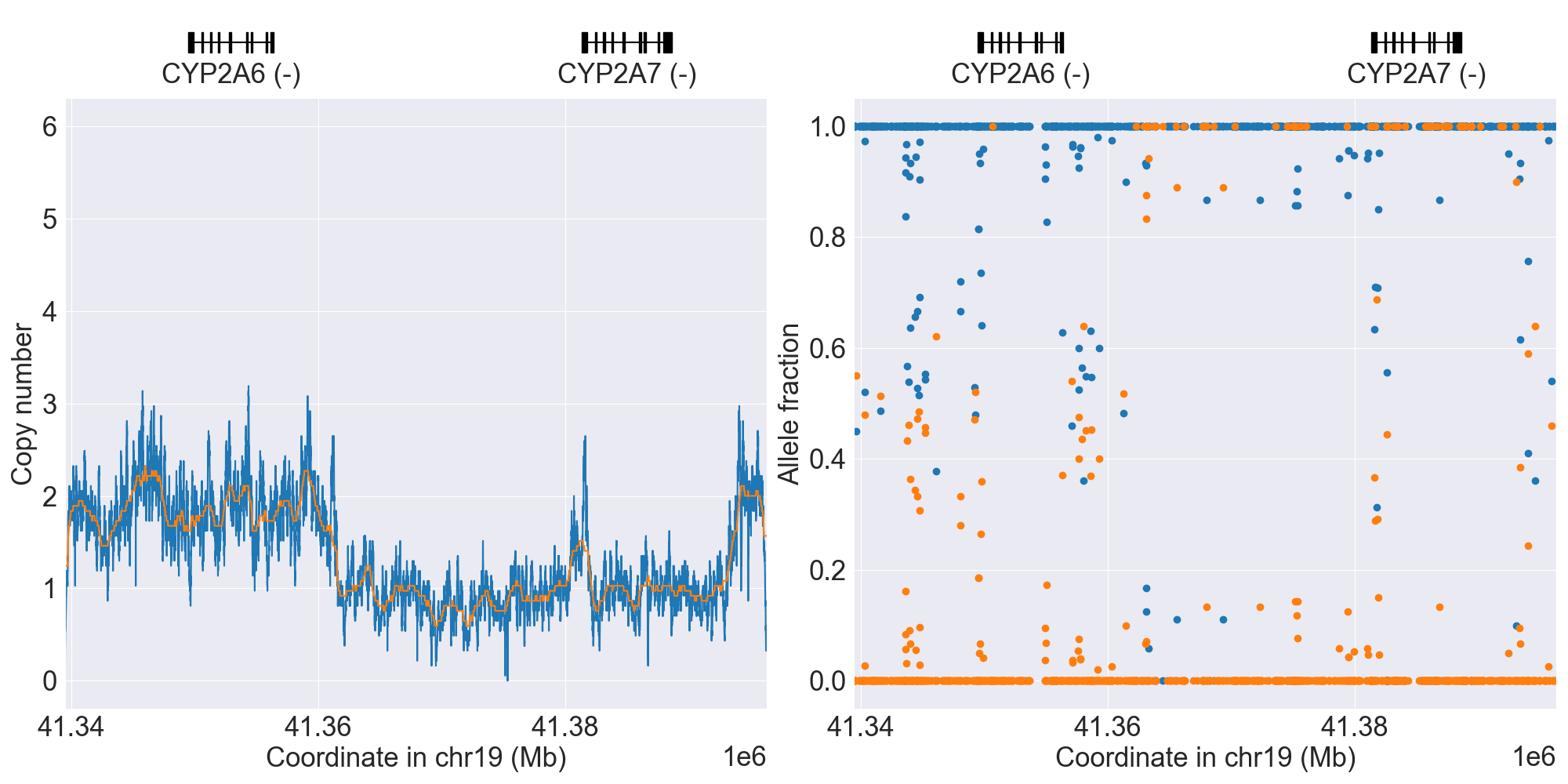
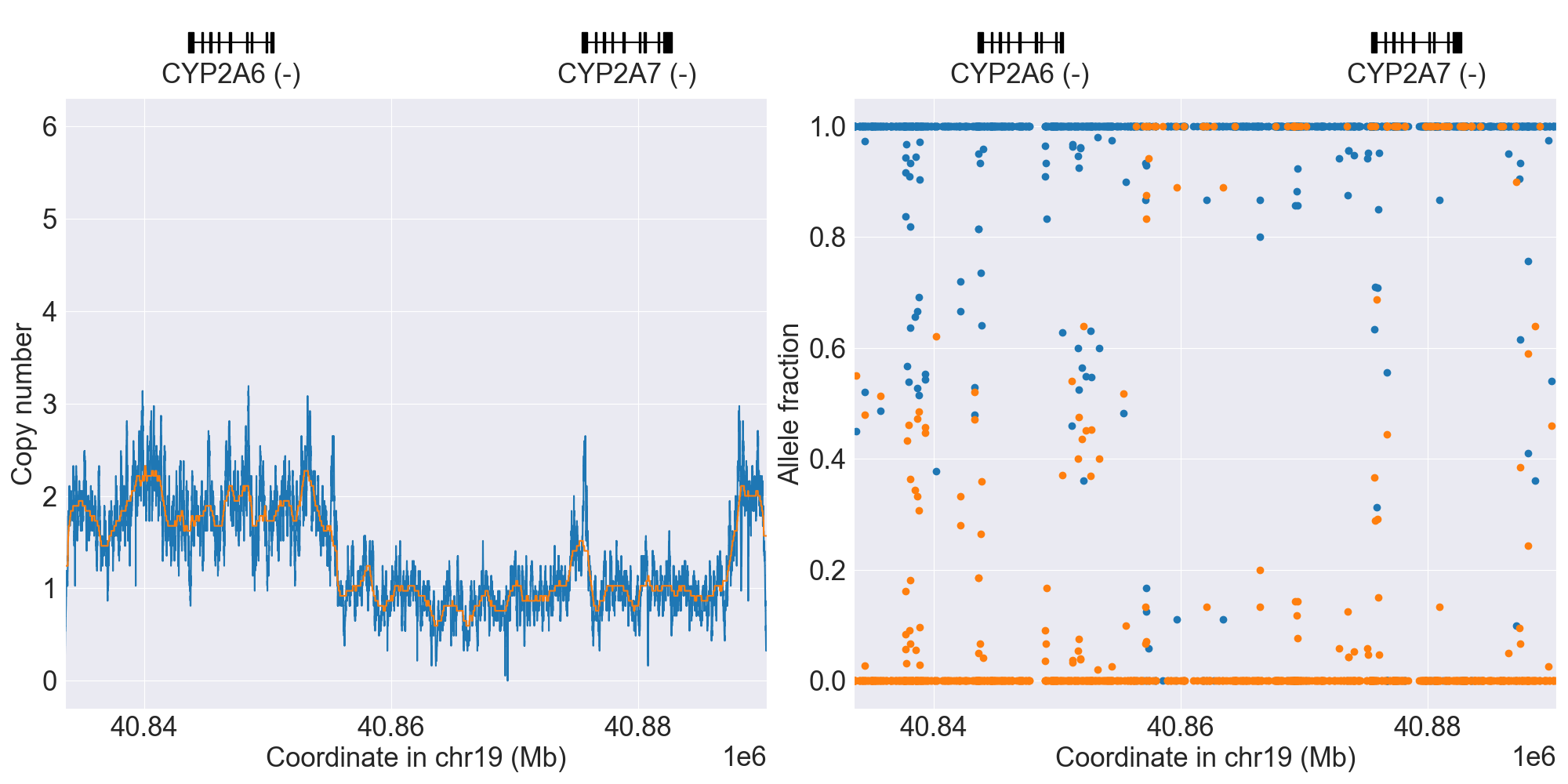
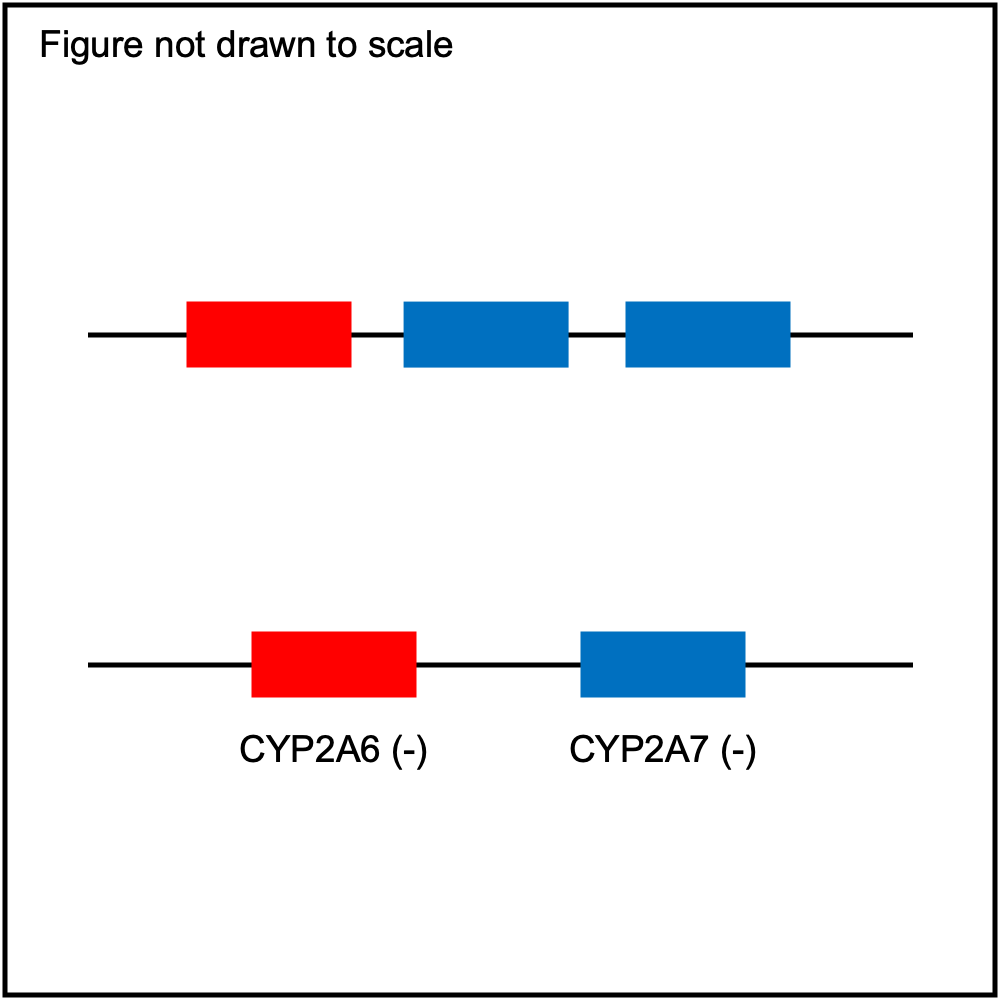
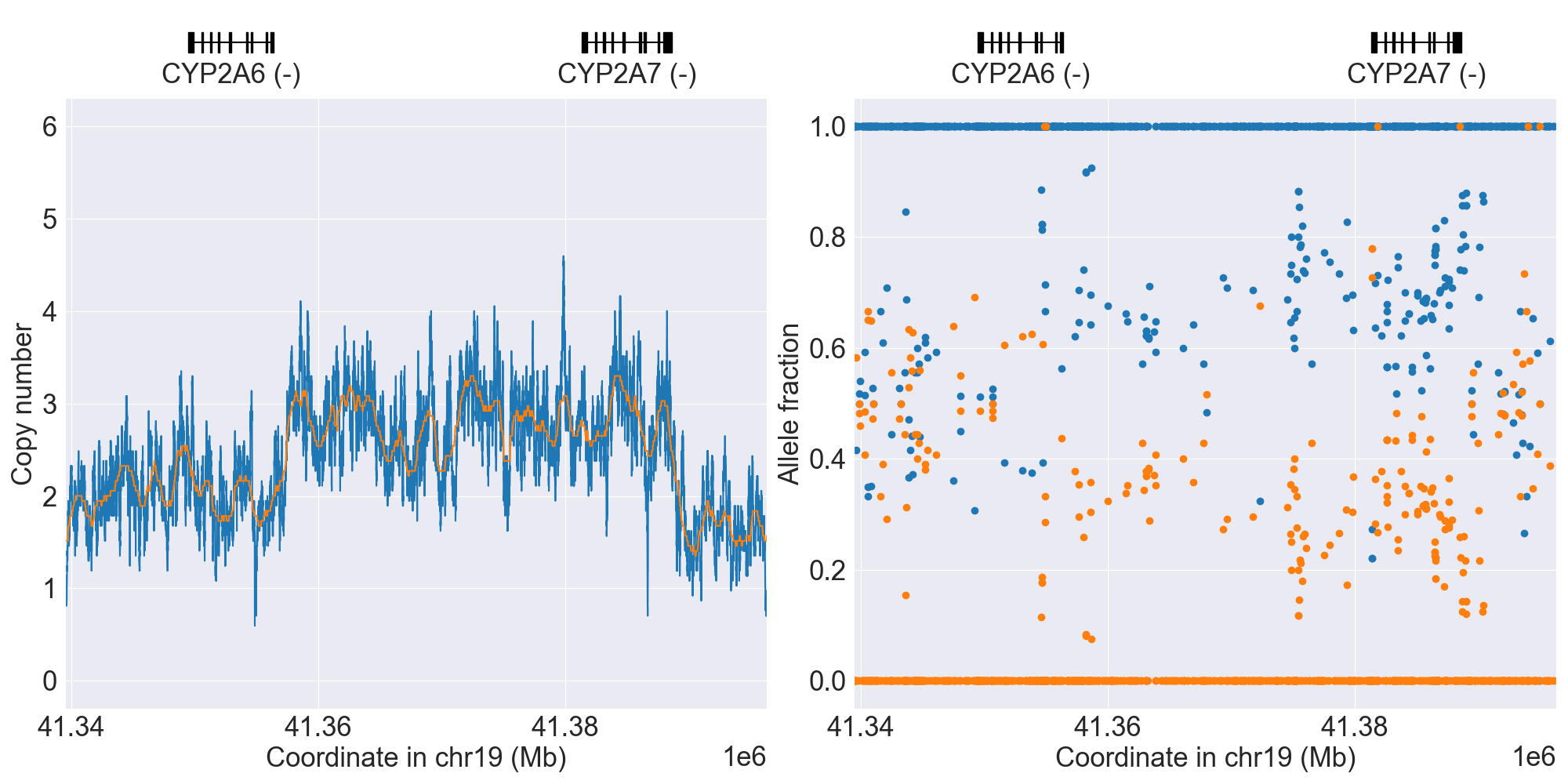
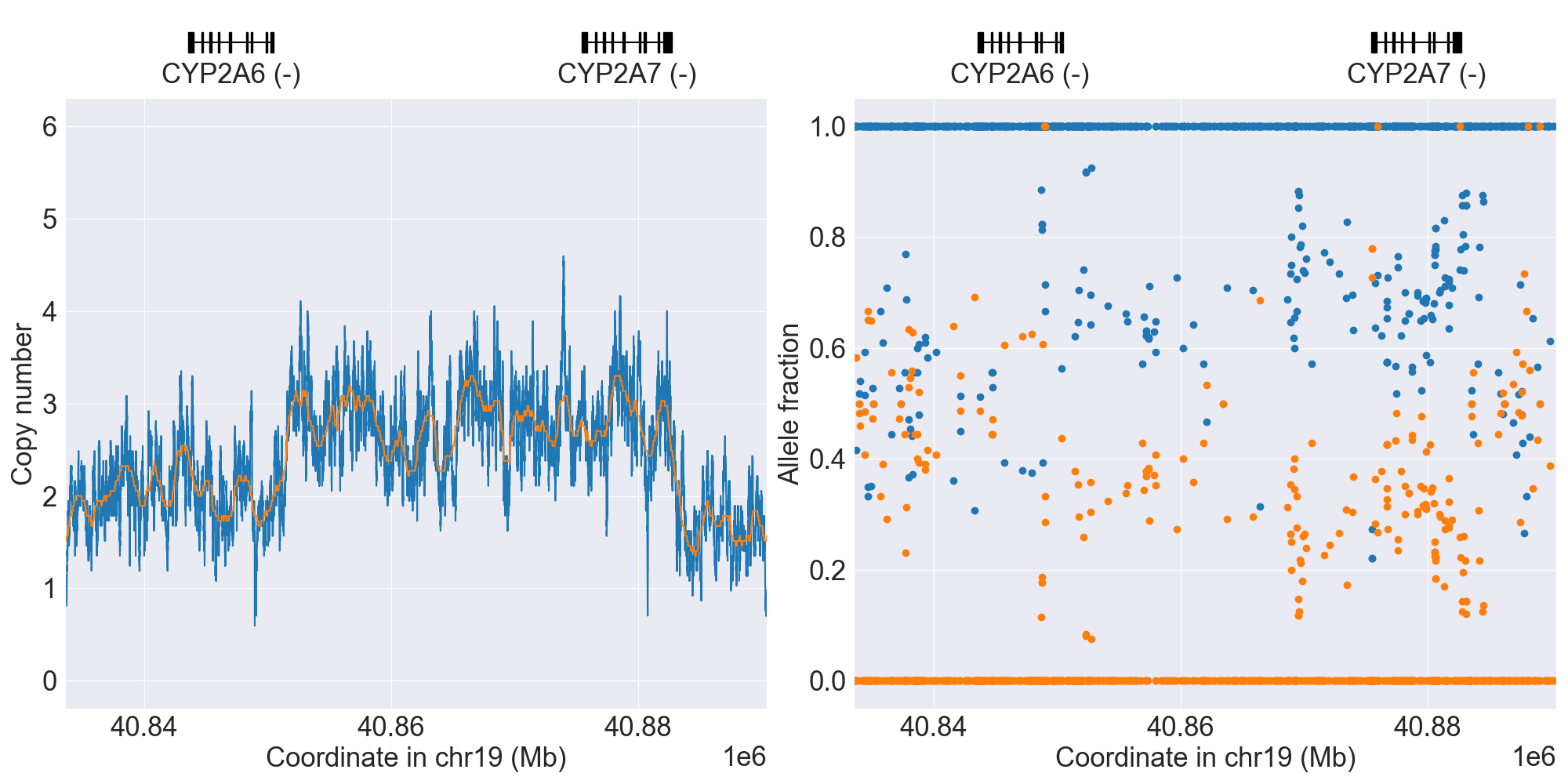
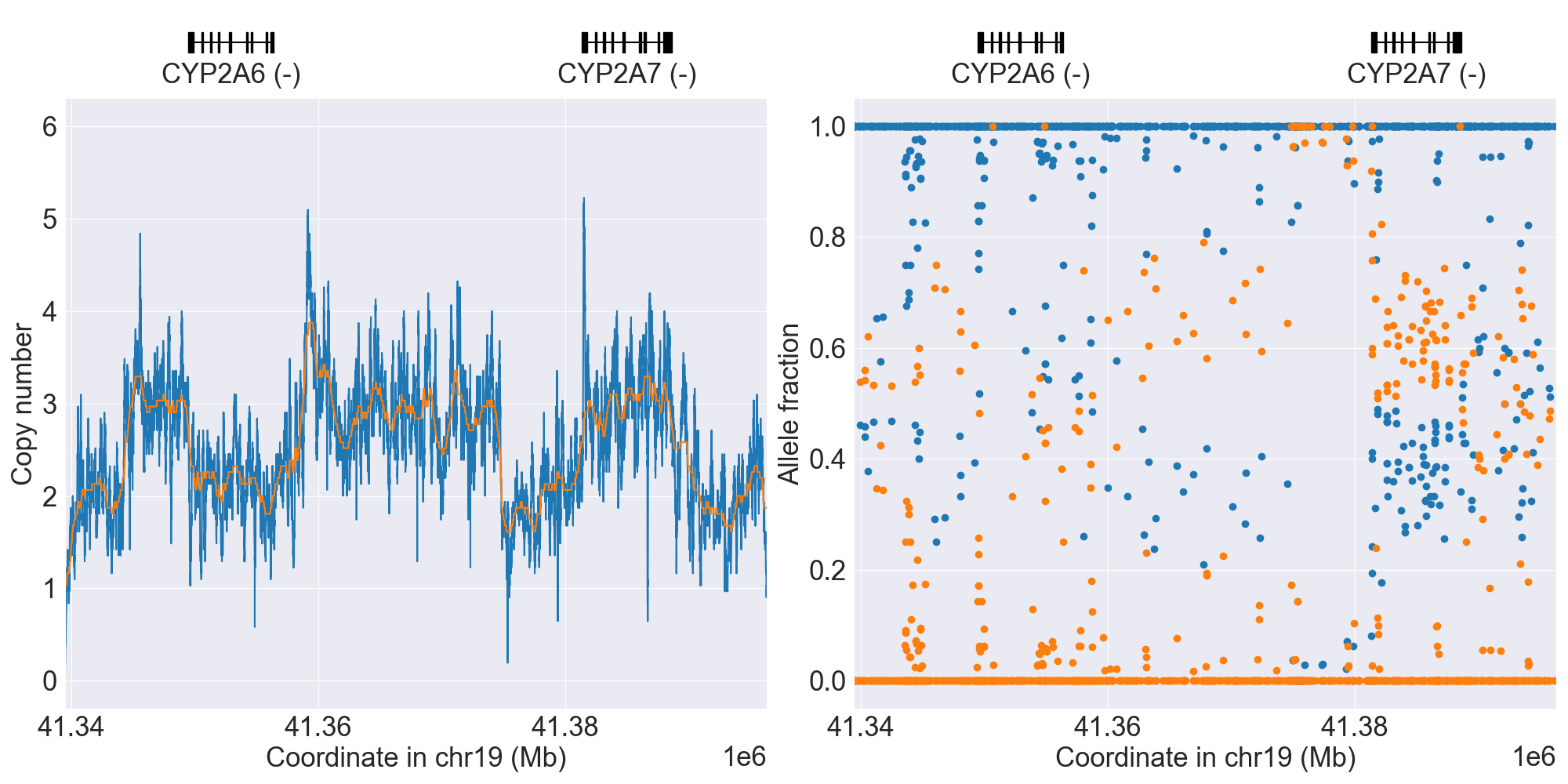
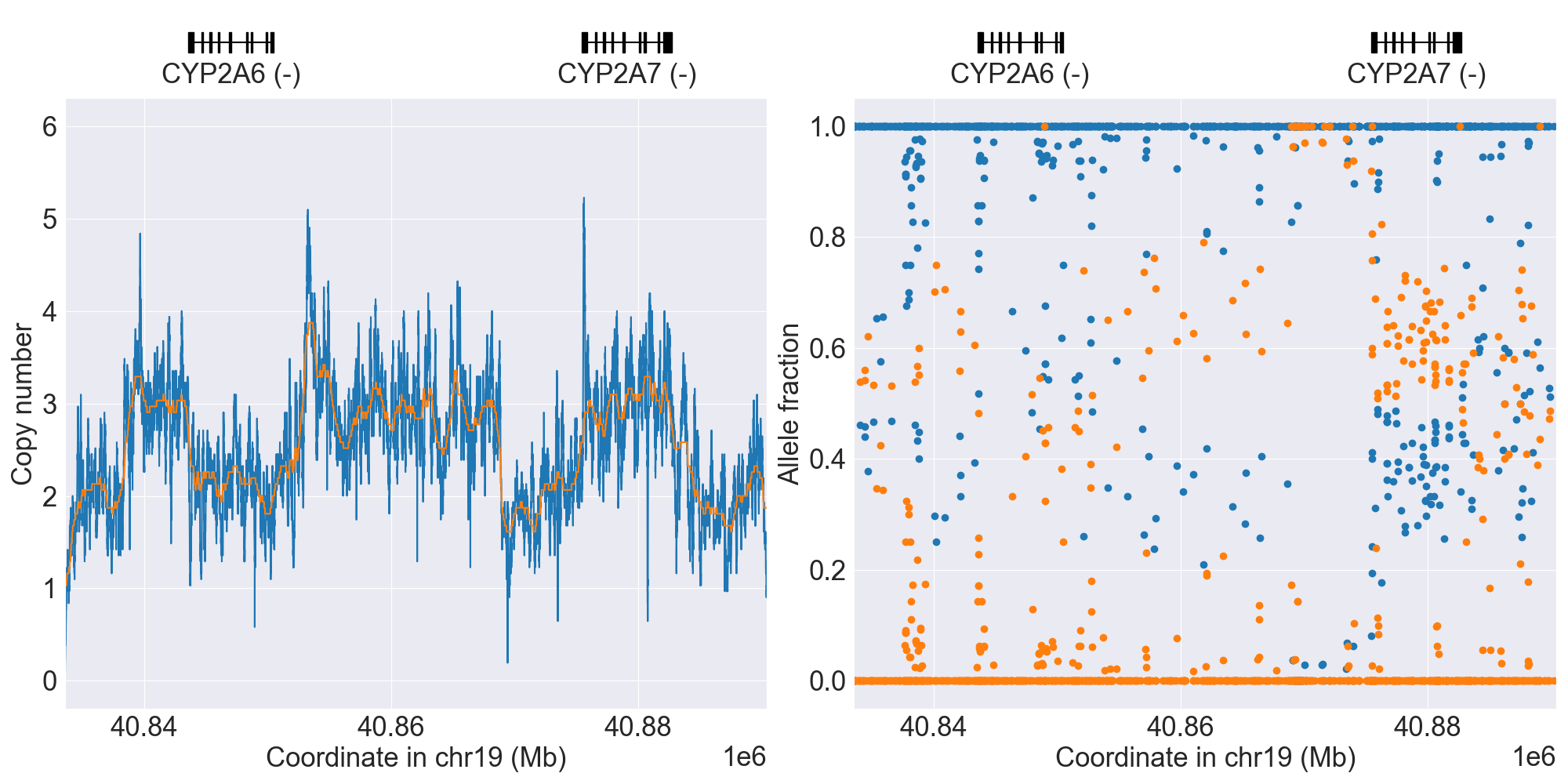
CYP2A6
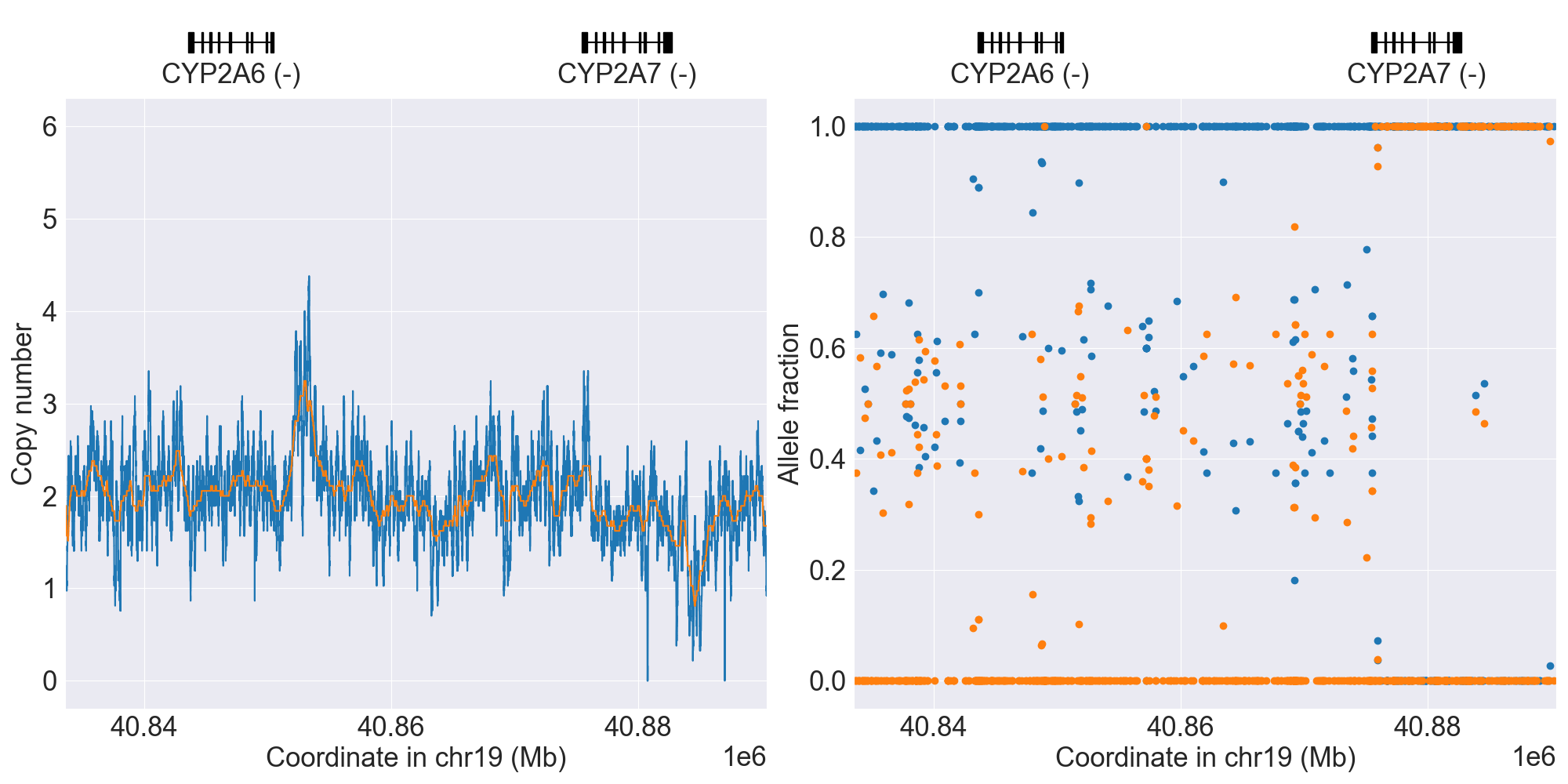
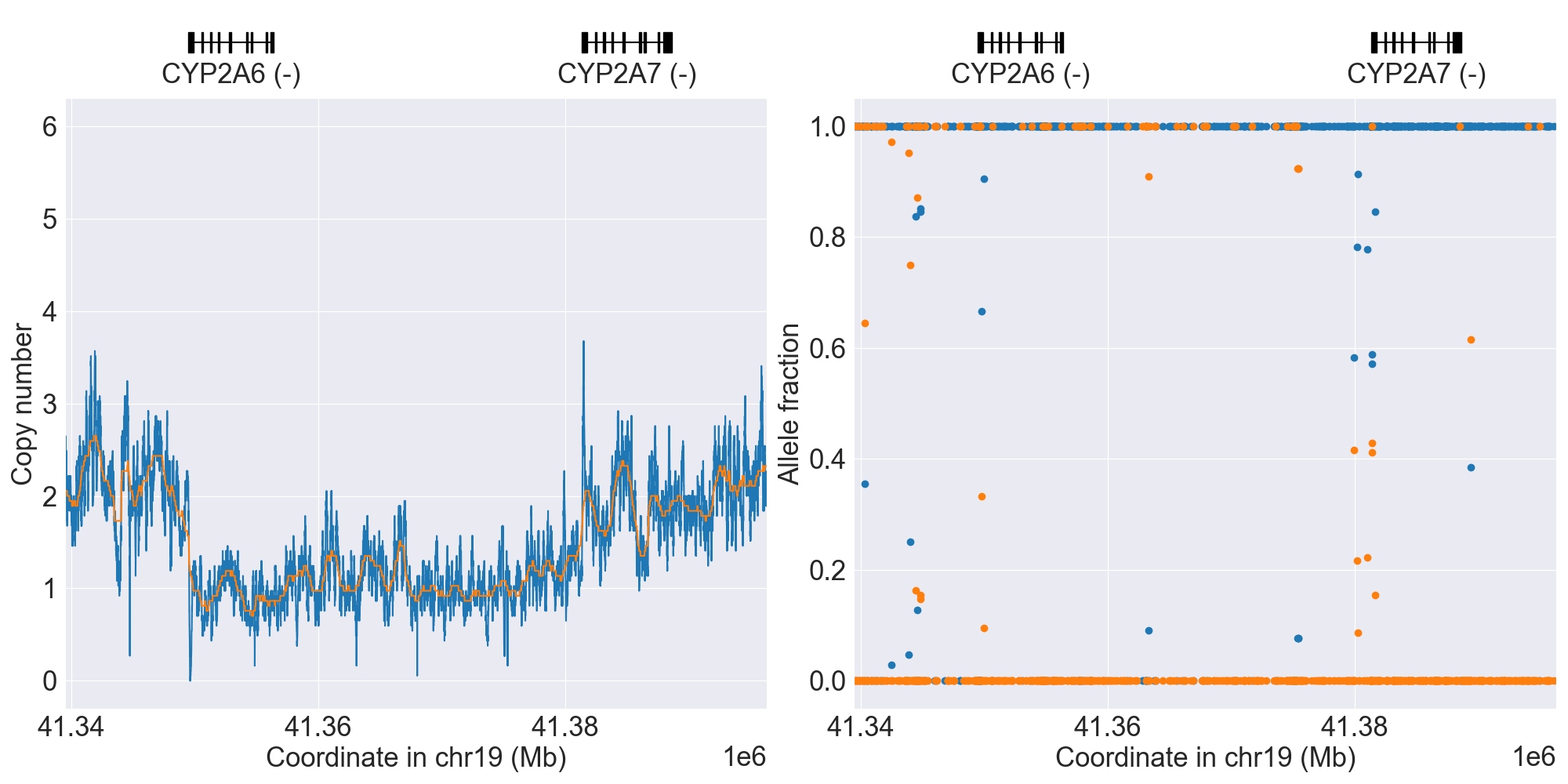
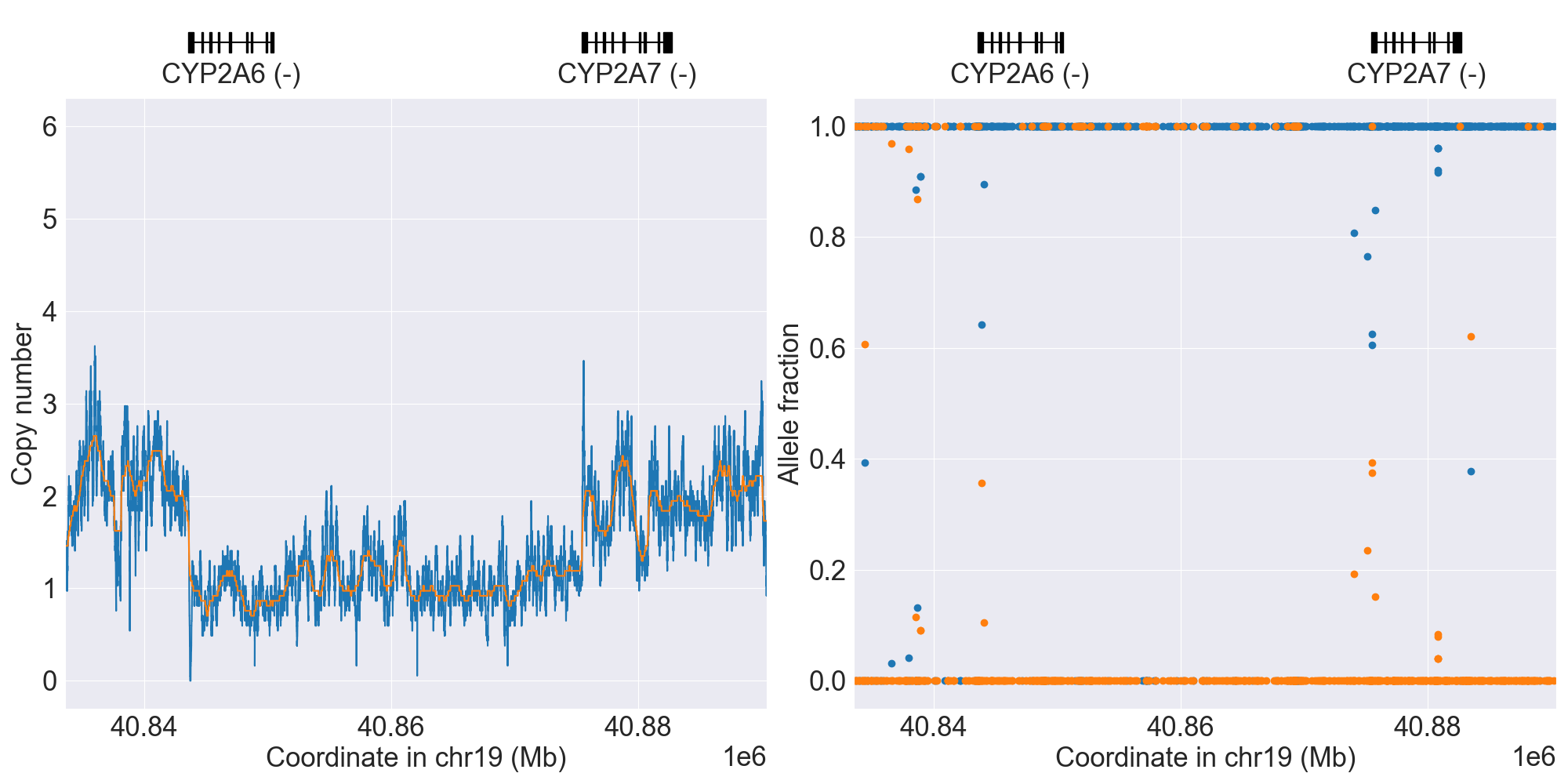
SV summary for CYP2A6
Below is comprehensive summary of SV described from real NGS studies:
SV Alleles |
SV Name |
Genotype |
Reference |
Gene Model |
GRCh37 |
GRCh38 |
Data Type |
Source |
Coriell ID |
Version |
Description |
|---|---|---|---|---|---|---|---|---|---|---|---|
Normal |
*1/*2 |
WGS |
NA10831 |
0.4.1 |
|||||||
*4 |
WholeDel1 |
*1/*4 |
WGS |
NA18617 |
0.4.1 |
||||||
*4 |
WholeDel1Hom |
*4/*4 |
WGS |
NA18952 |
0.4.1 |
||||||
*4 |
WholeDel2 |
*1/*4 |
WGS |
0.12.0 |
|||||||
*4 |
WholeDel2Hom |
*4/*4 |
WGS |
NA21093 |
0.15.0 |
||||||
*4 |
WholeDel3 |
*4/*9 |
WGS |
NA18488 |
0.12.0 |
||||||
*1x2 |
WholeDup1 |
*1x2/*25 |
WGS |
NA18861 |
0.4.1 |
||||||
*1x2 |
WholeDup2 |
*1x2/*2 |
WGS |
NA12342 |
0.12.0 |
||||||
*1x2 |
WholeDup3 |
*1x2/*17 |
WGS |
NA19129 |
0.12.0 |
||||||
Hybrid1 |
Indeterminate |
WGS |
HG00436 |
0.4.1 |
|||||||
*12 |
Hybrid2 |
*1/*12 |
WGS |
NA11829 |
0.12.0 |
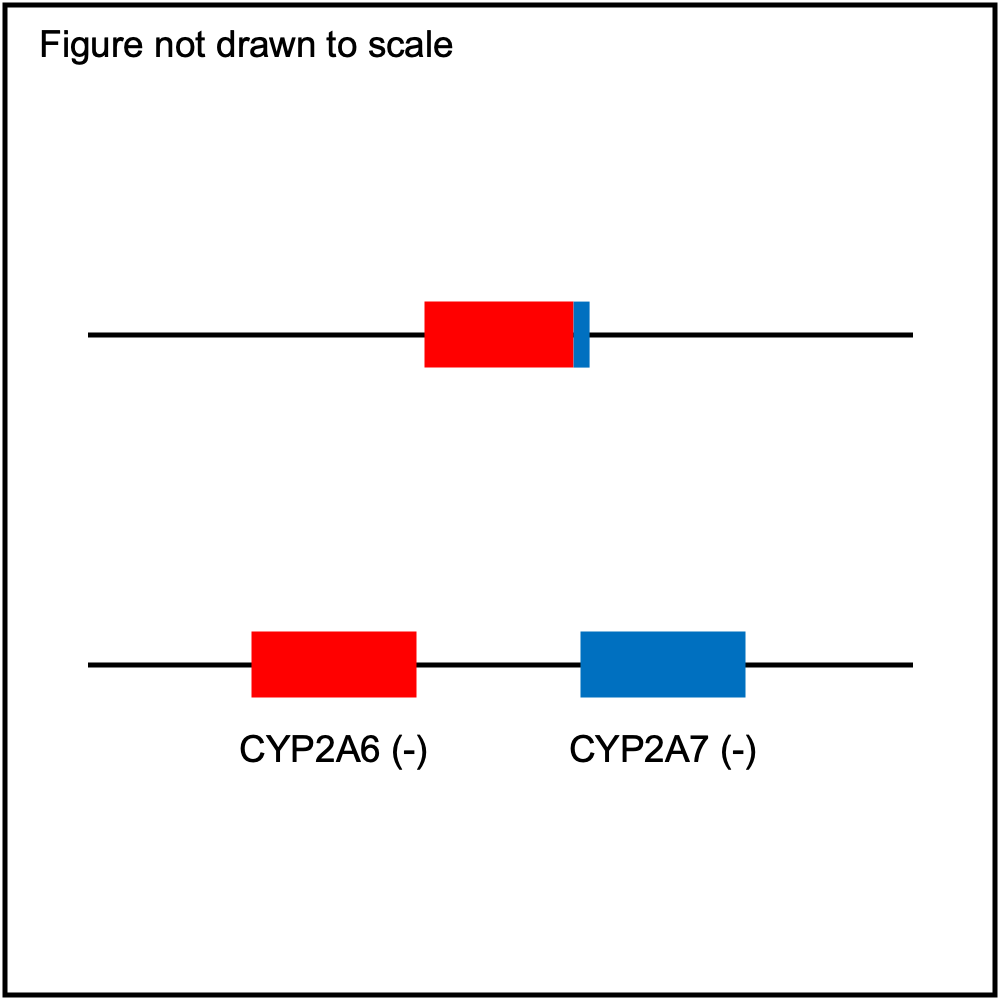
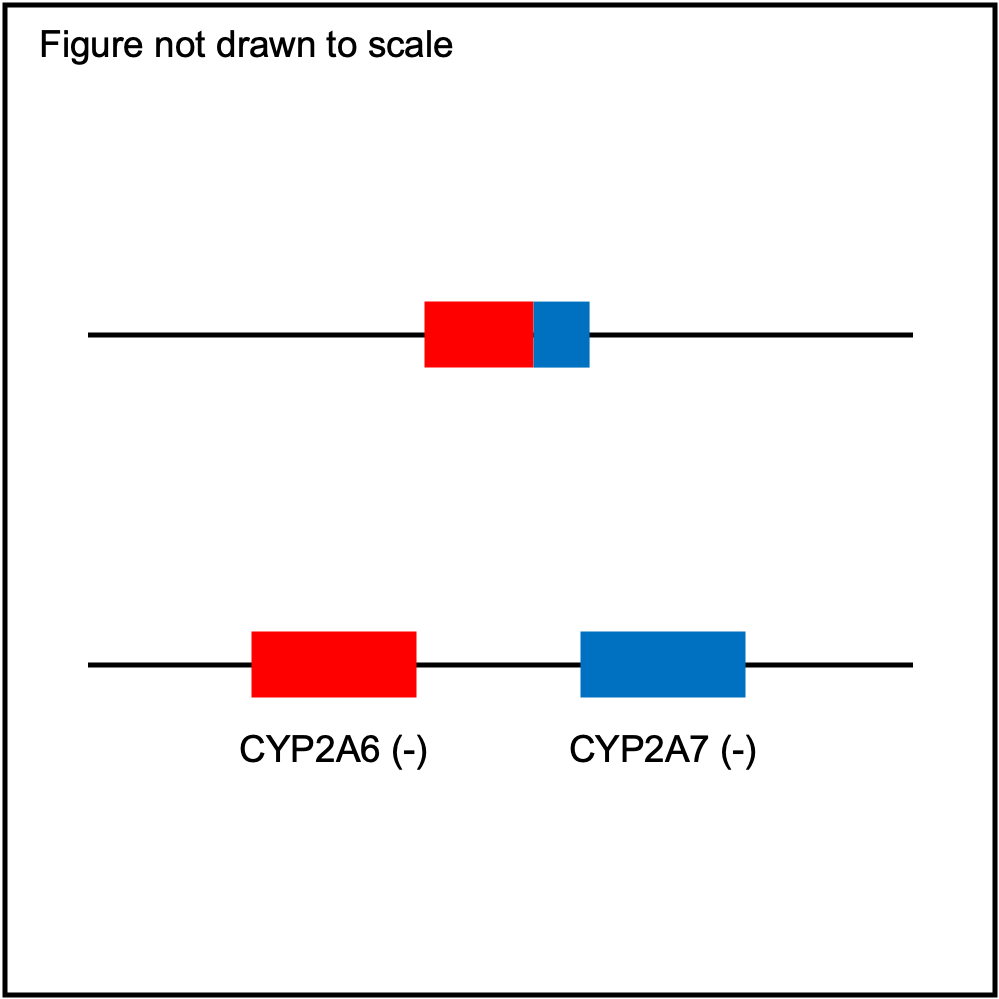
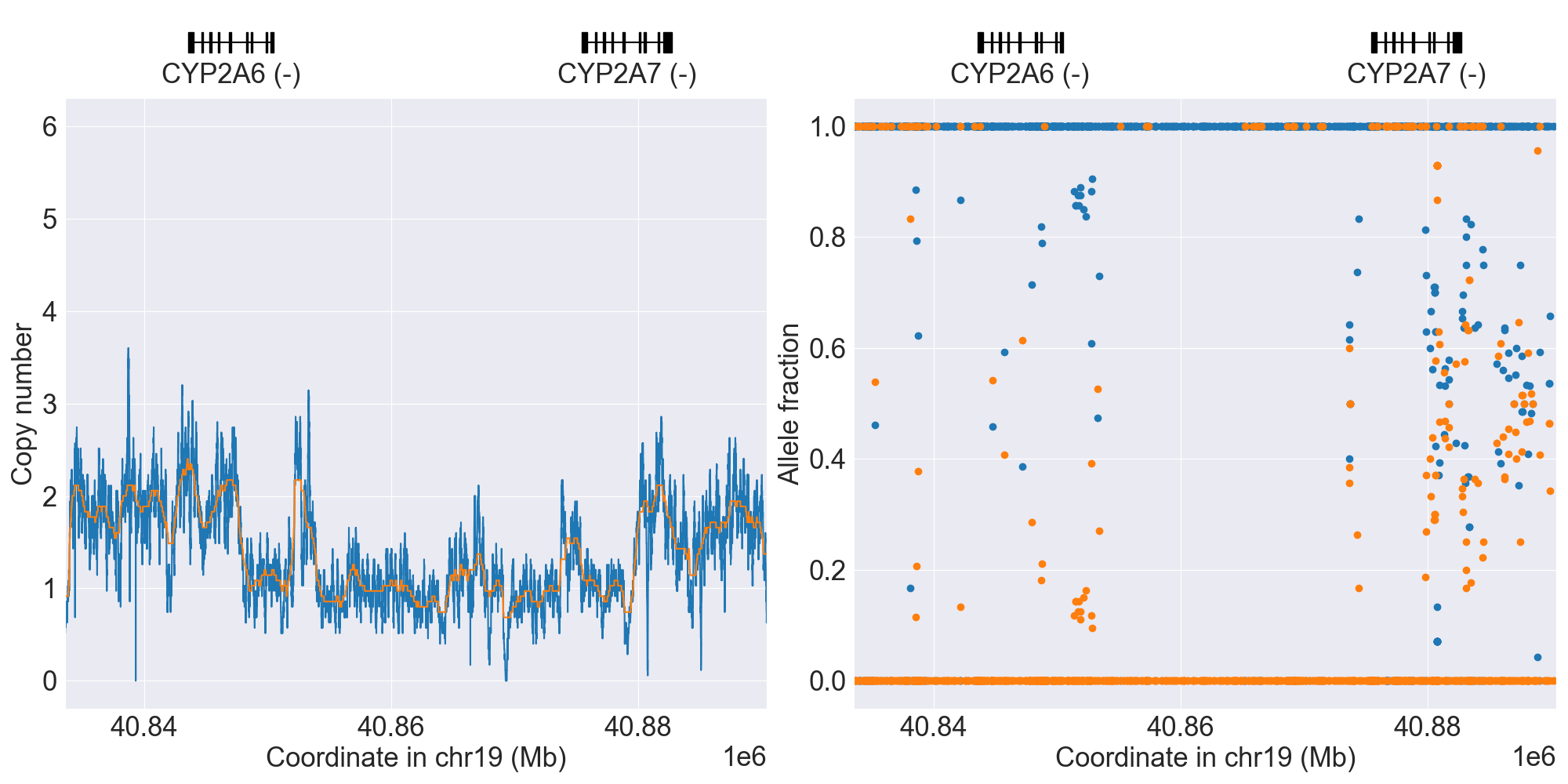
*12 has exons 1-2 of CYP2A7 origin and exons 3-9 of CYP2A6 origin (breakpoint in intron 2). |
|||||
*12 |
Hybrid2Hom |
*12/*12 |
WGS |
NA19780 |
0.14.0 |
||||||
*34 |
Hybrid3 |
*1/*34 |
WGS |
NA18516 |
0.12.0 |
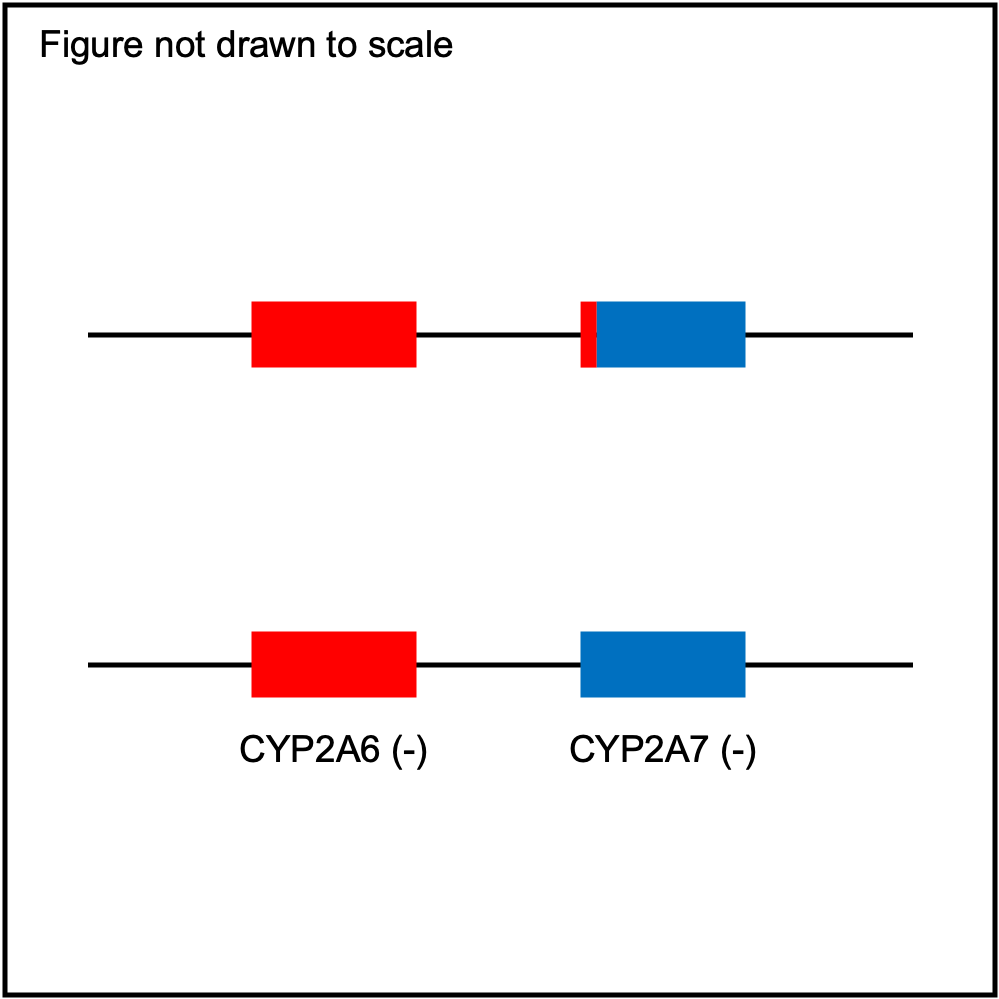
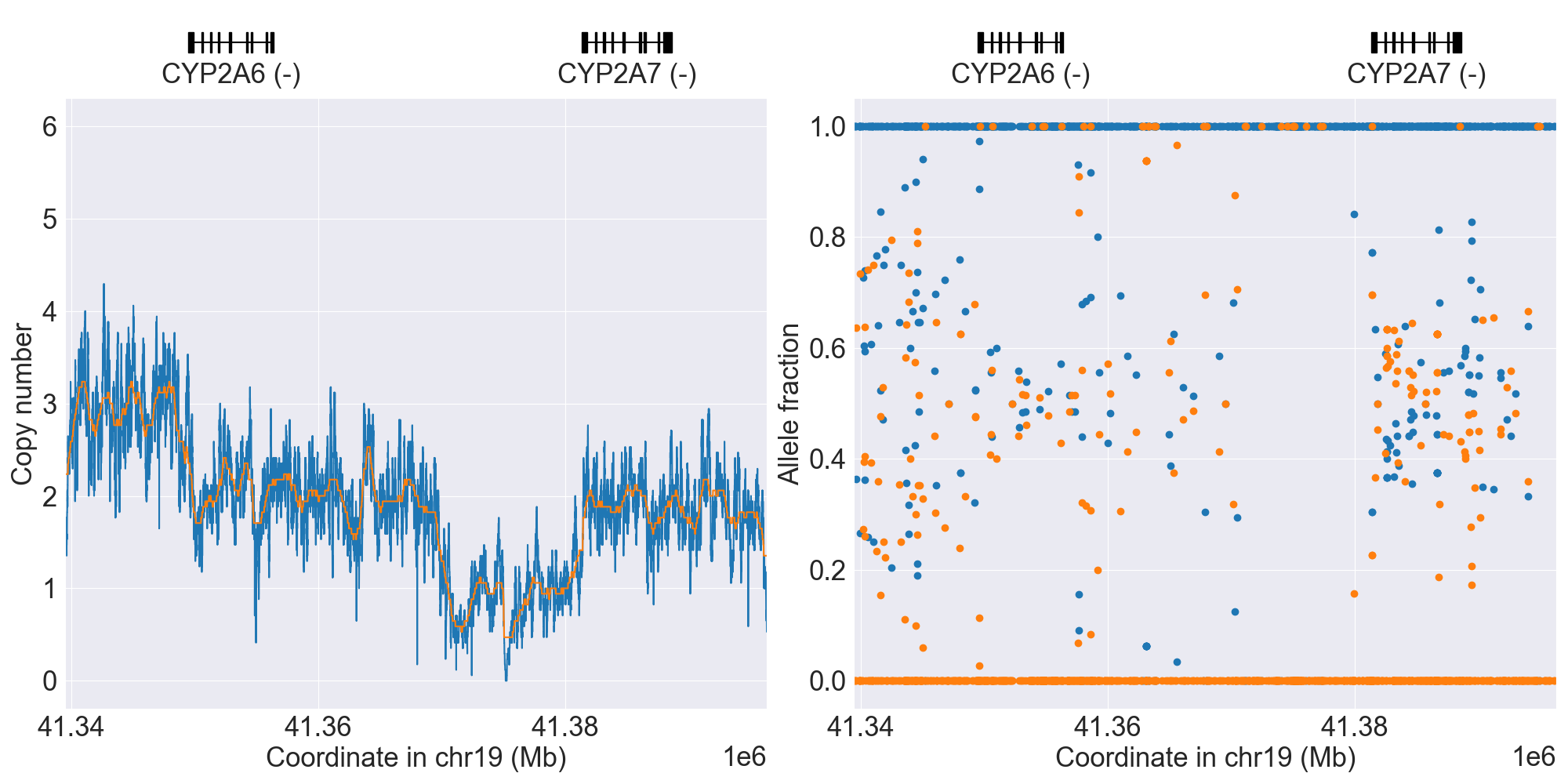
*34 has exons 1-4 of CYP2A7 origin and exons 5-9 of CYP2A6 origin (breakpoint in intron 4). |
|||||
Hybrid4 |
Indeterminate |
WGS |
NA20515 |
0.14.0 |
|||||||
Hybrid5 |
Indeterminate |
WGS |
HG00155 |
0.15.0 |
|||||||
Hybrid6 |
Indeterminate |
WGS |
HG00141 |
0.15.0 |
|||||||
Hybrid7 |
Indeterminate |
WGS |
HG02382 |
0.16.0 |
|||||||
Tandem1 |
Indeterminate |
WGS |
NA20828 |
0.14.0 |
|||||||
Tandem2 |
Indeterminate |
WGS |
HG04214 |
0.16.0 |
|||||||
ParalogWholeDel1 |
Indeterminate |
WGS |
HG00625 |
0.15.0 |
|||||||
ParalogWholeDup1 |
Indeterminate |
WGS |
NA06985 |
0.12.0 |
|||||||
Unknown1 |
Indeterminate |
WGS |
HG02081 |
0.16.0 |
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
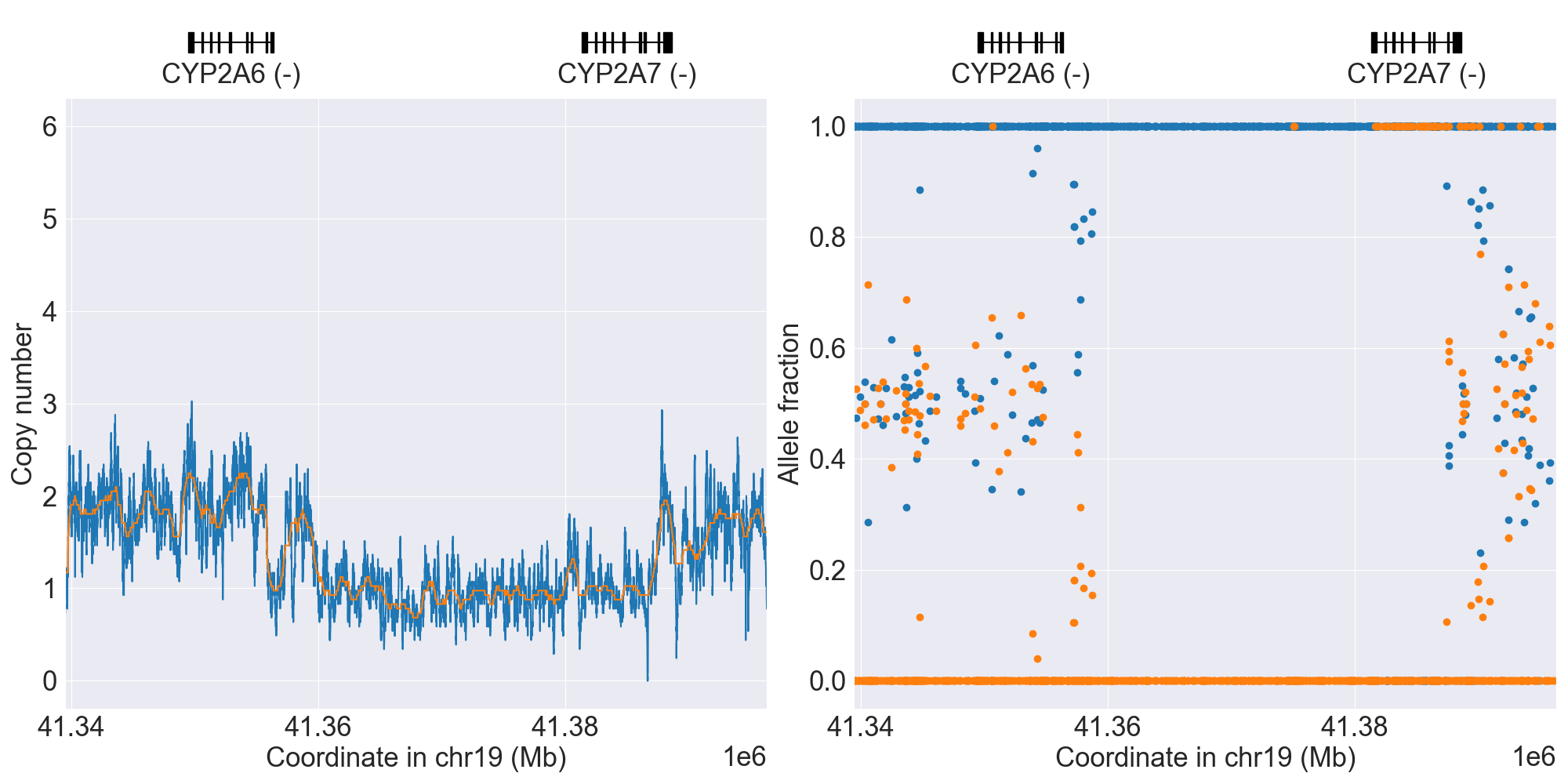
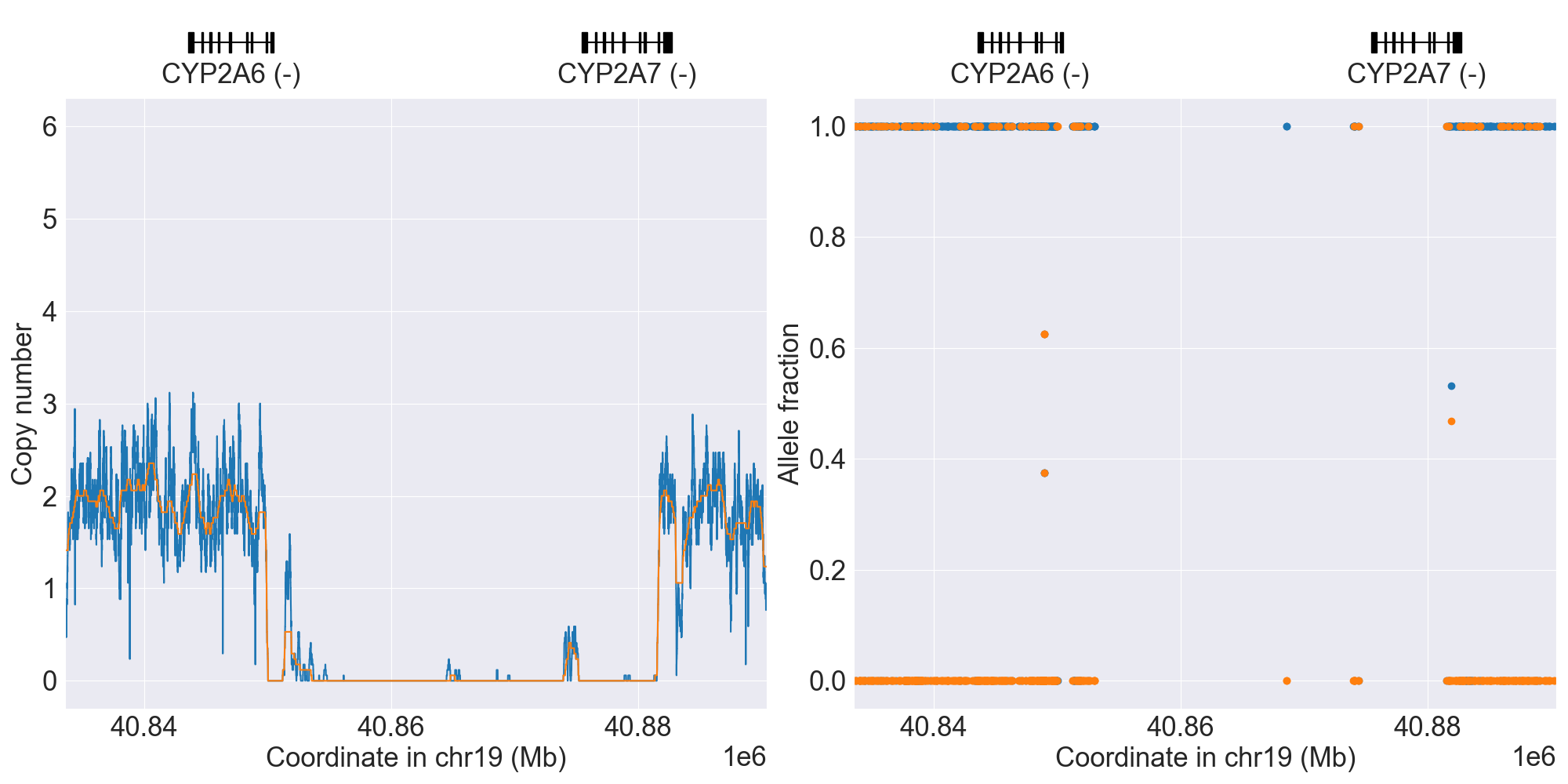
PyPGx was recently applied to the entire high-coverage WGS dataset from 1KGP (N=2,504). Click here to see individual SV calls for CYP2A6, and corresponding copy number profiles and allele fraction profiles.
Filtered alleles for CYP2A6
Some alleles in PharmVar will not be called by PyPGx because one or more of their variants have a high false positive rate, likely due to read misalignment to the CYP2A7 pseudogene. Those alleles are listed in below table. If problematic variants are present in gnomAD, their links are provided so that you can look at filtering status, allele imbalance for heterozygotes, etc.
Problematic Variant |
Star Alleles |
GRCh37 |
GRCh38 |
|---|---|---|---|
rs143731390 (N438Y) |
*35 |
Resources for CYP2A6
CYP2A13
Resources for CYP2A13
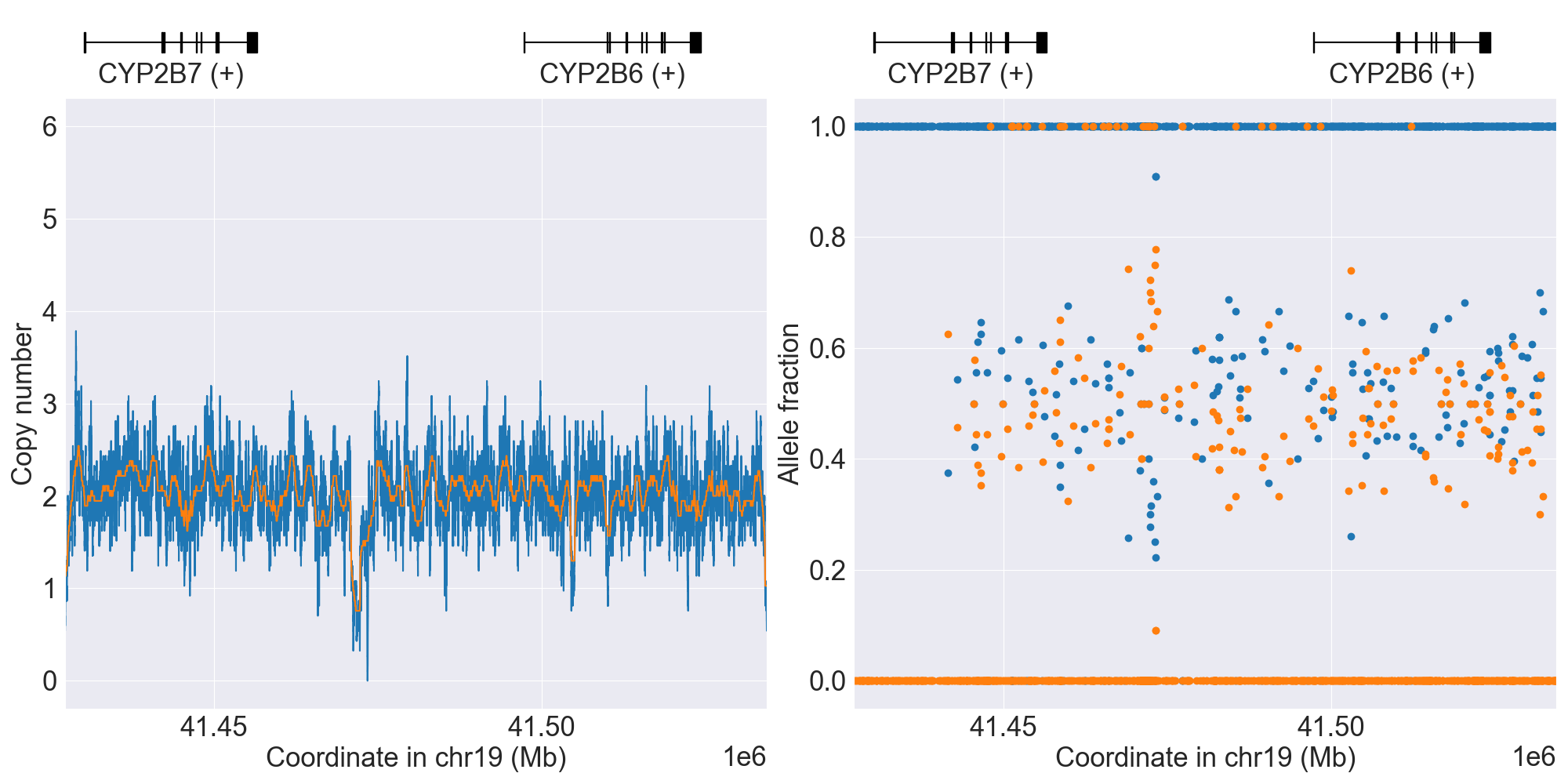
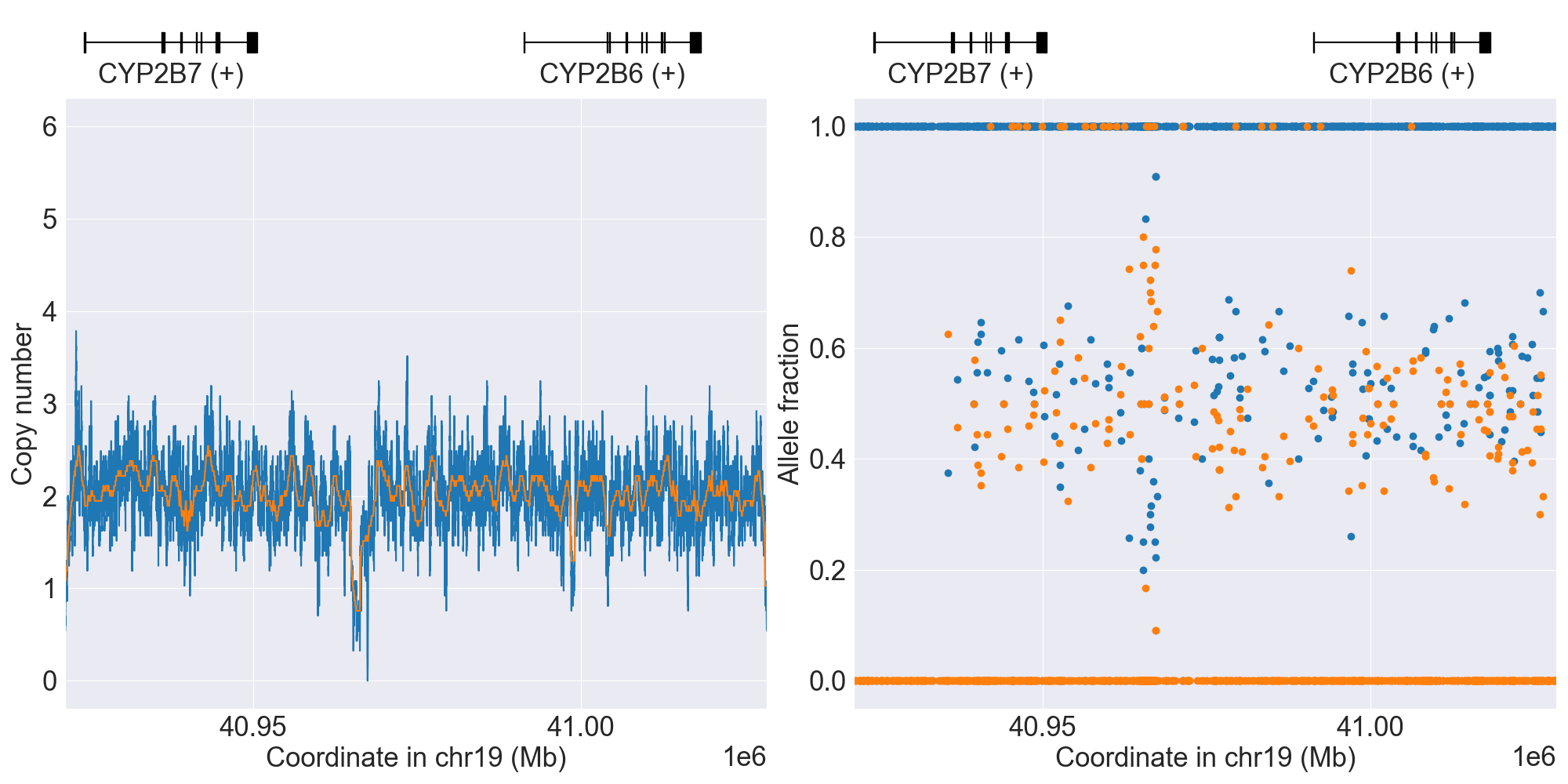
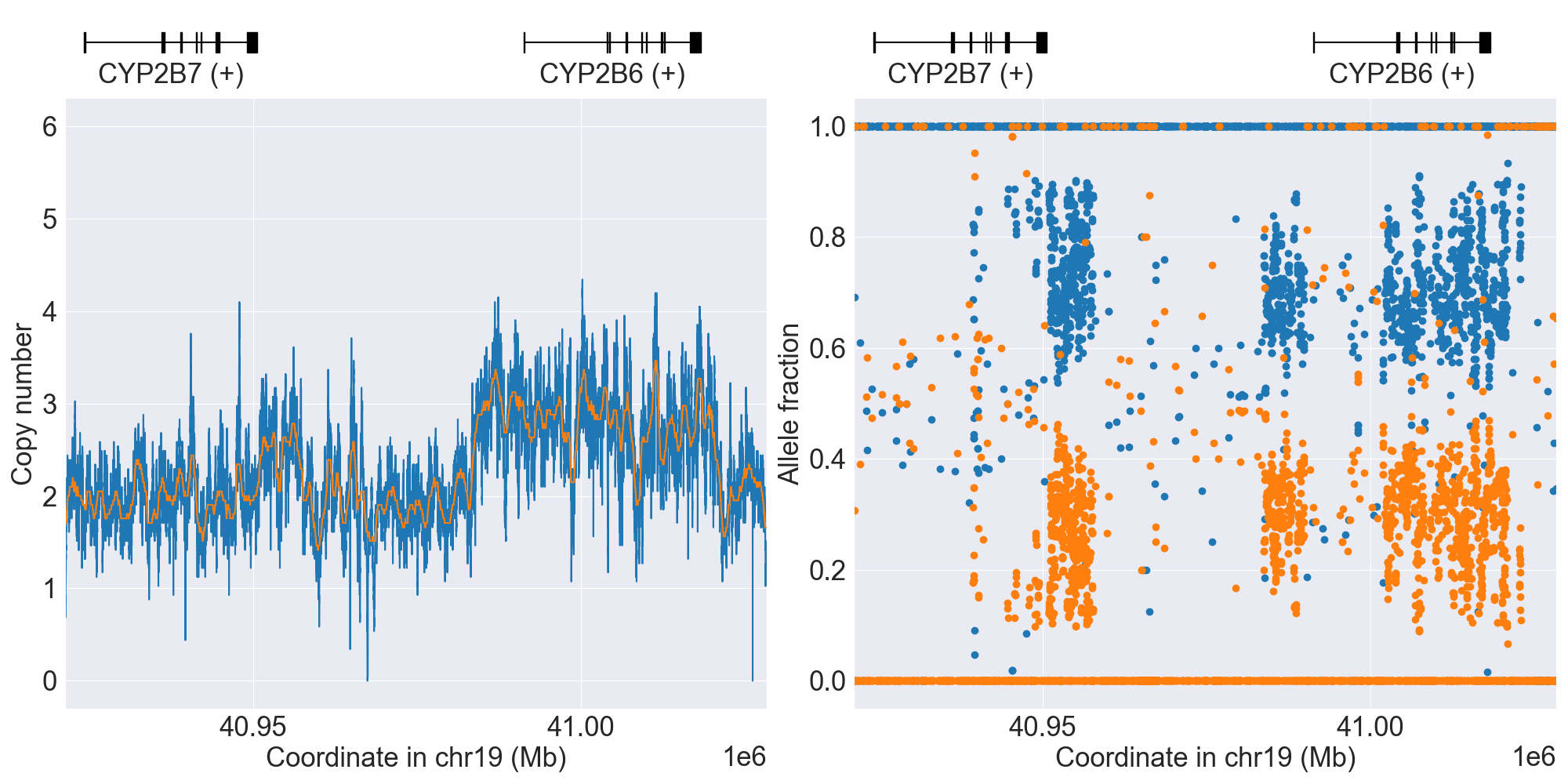
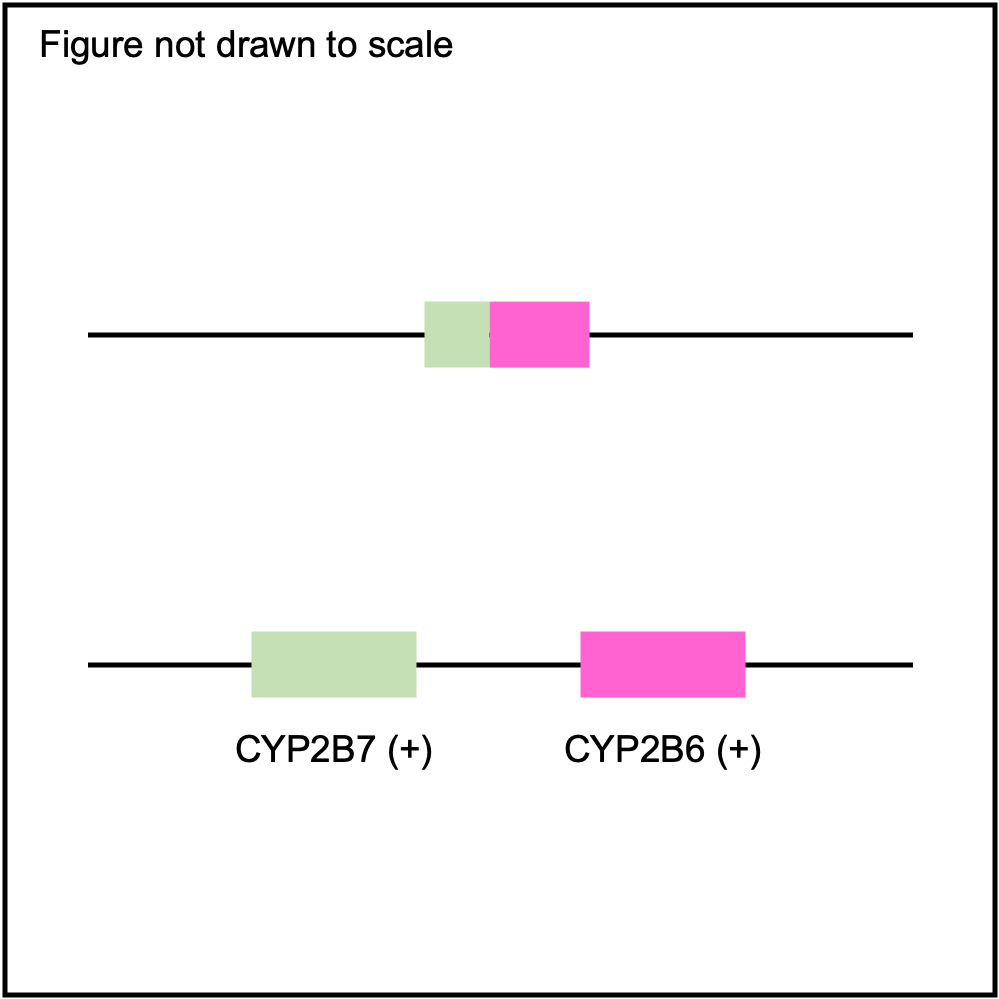
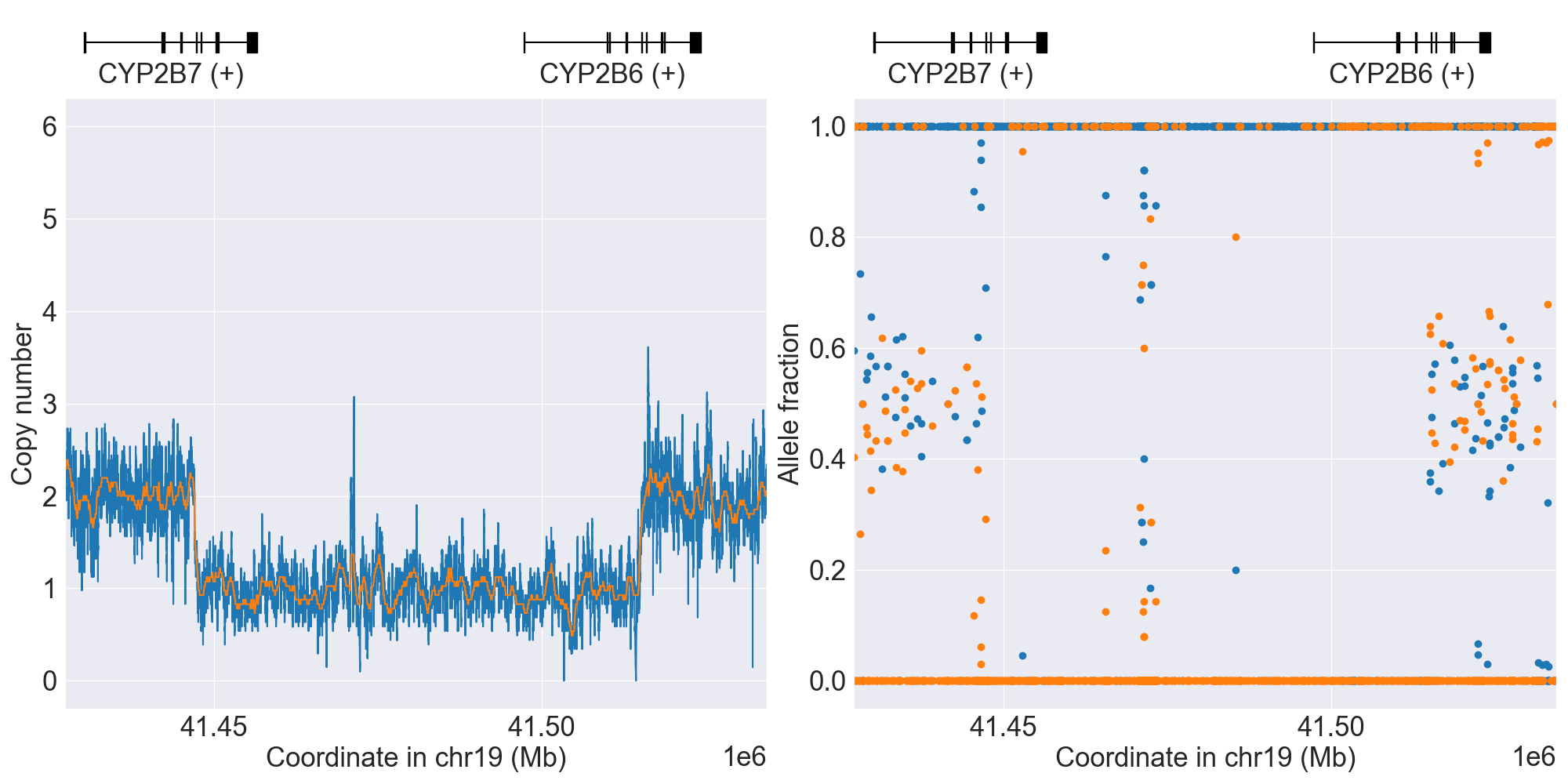
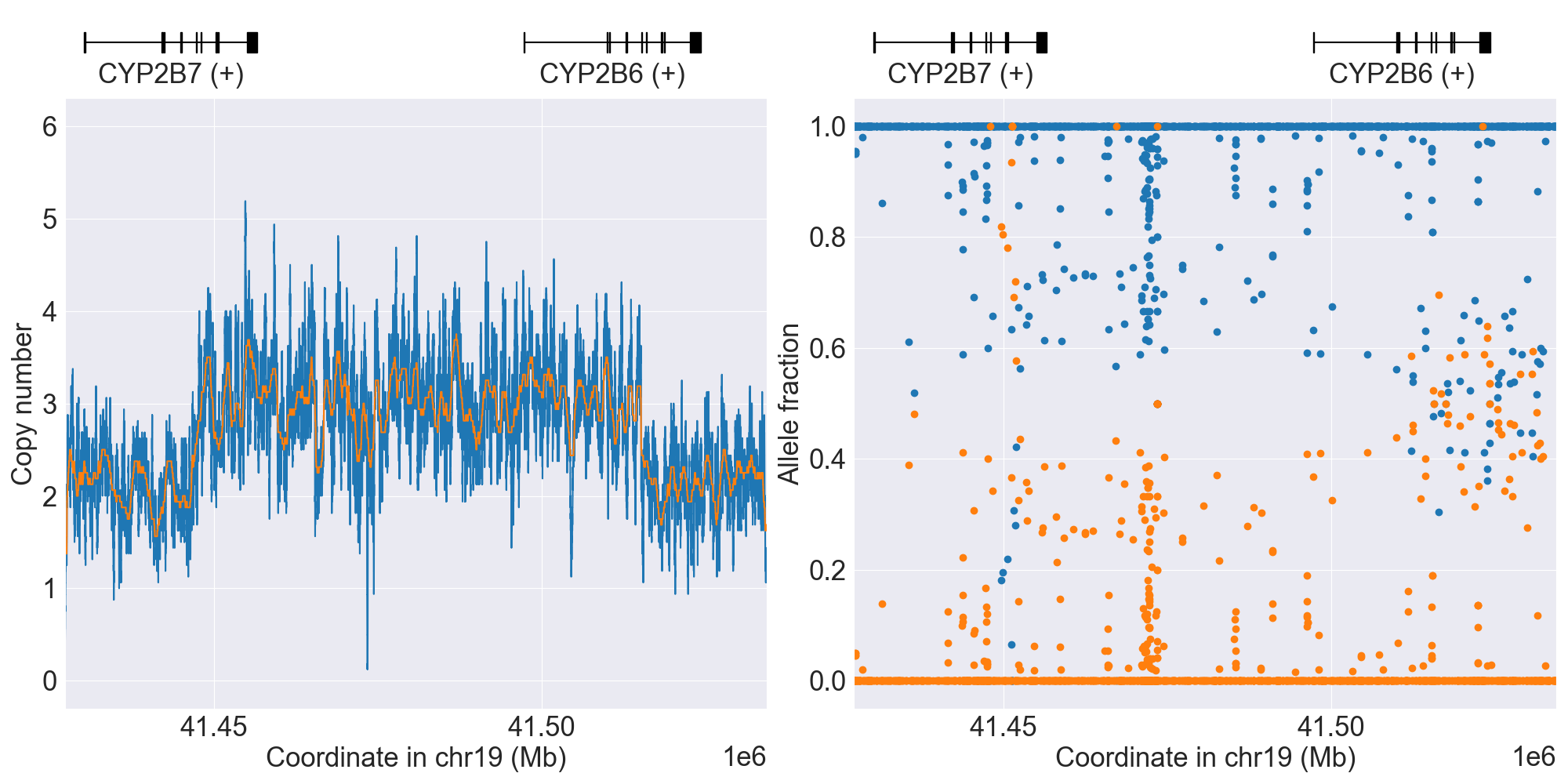
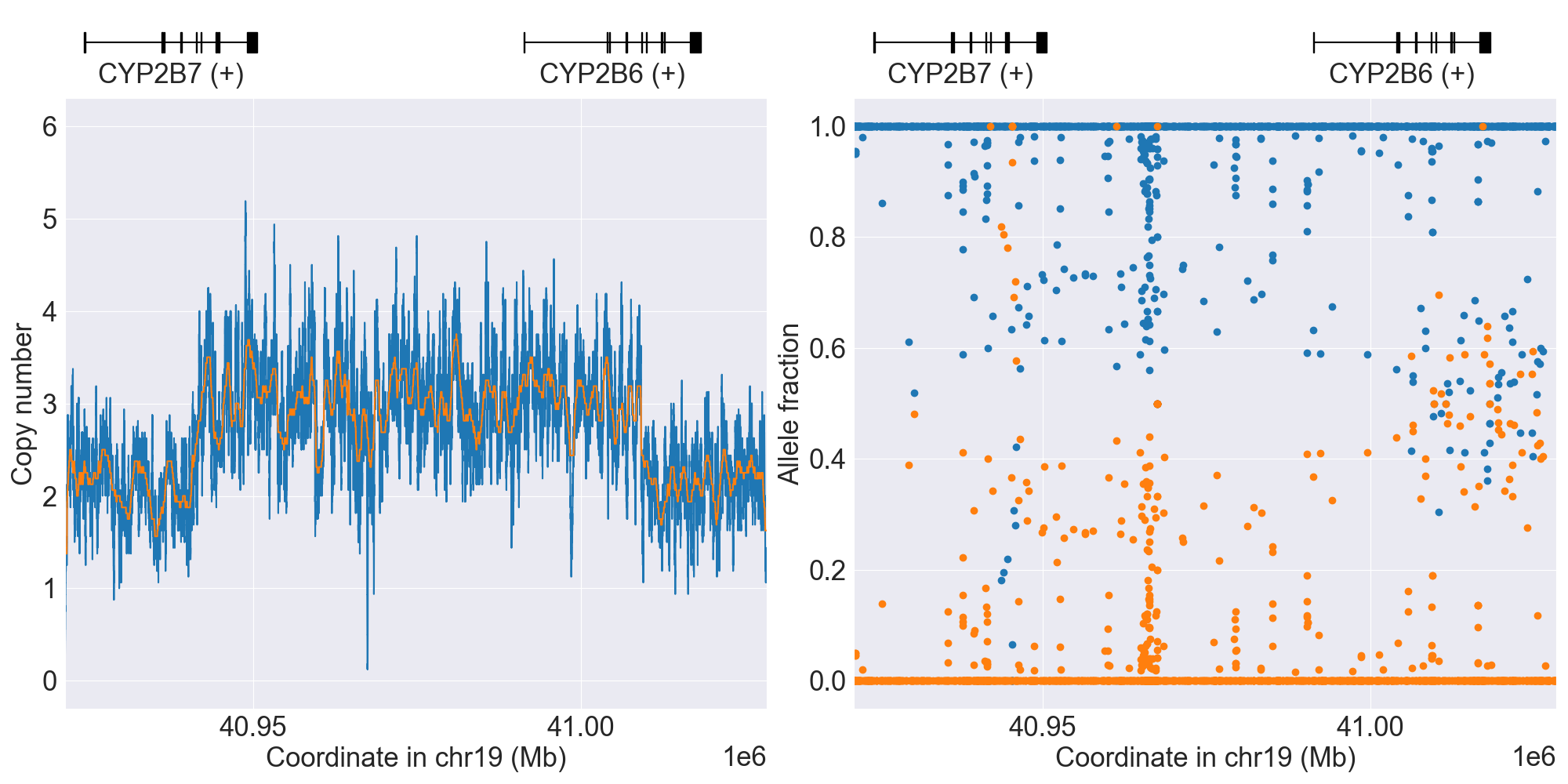
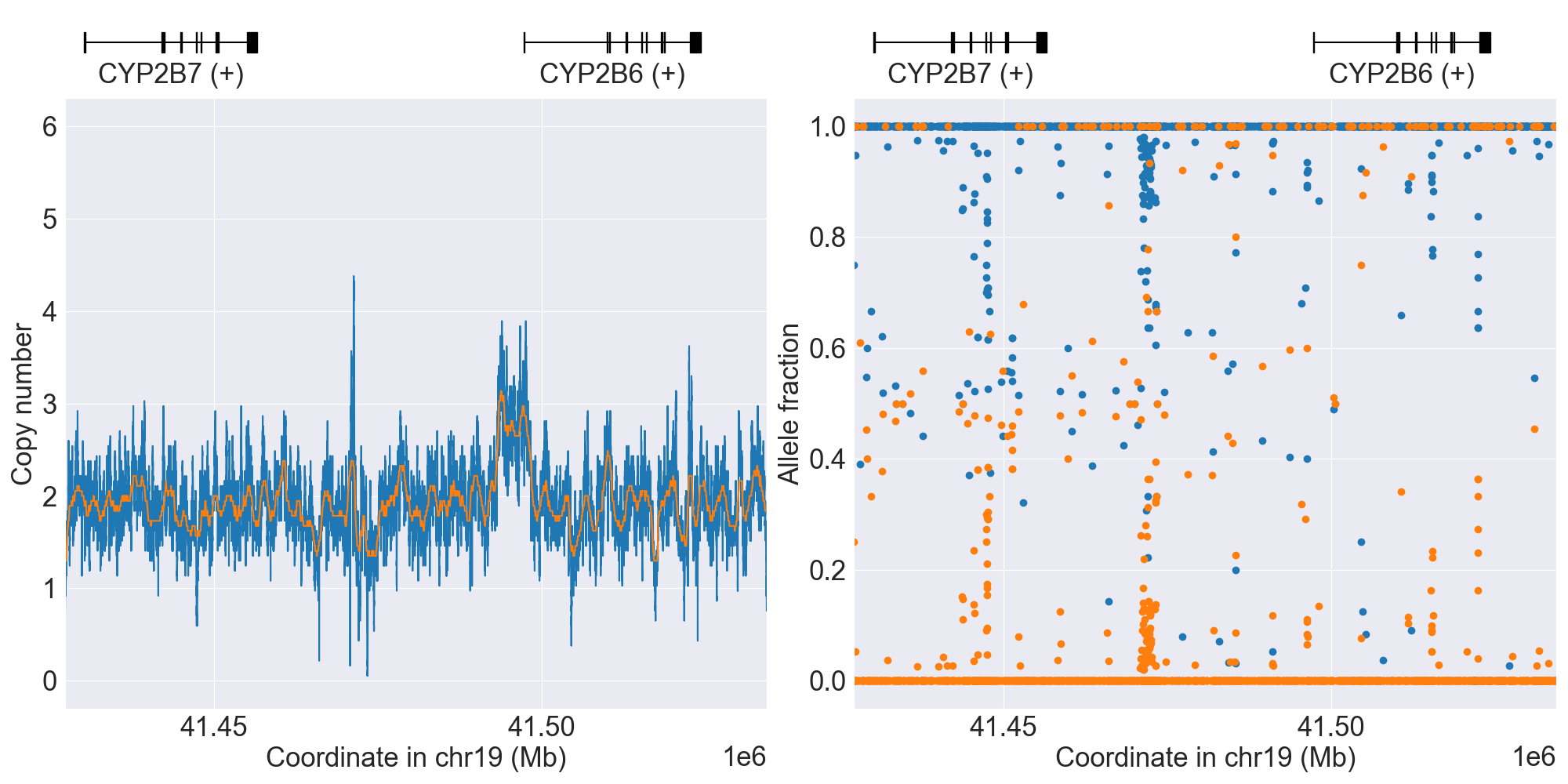
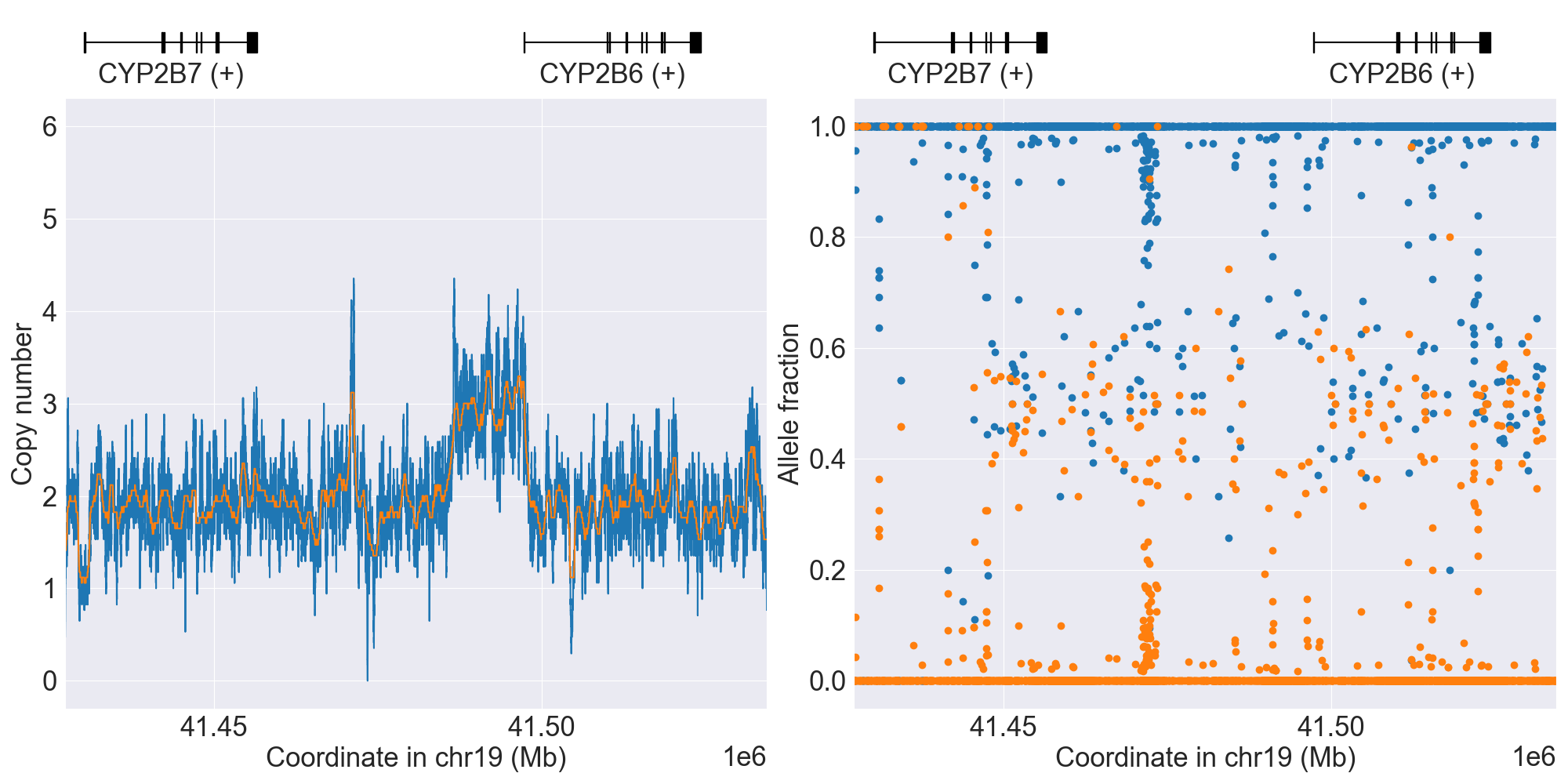
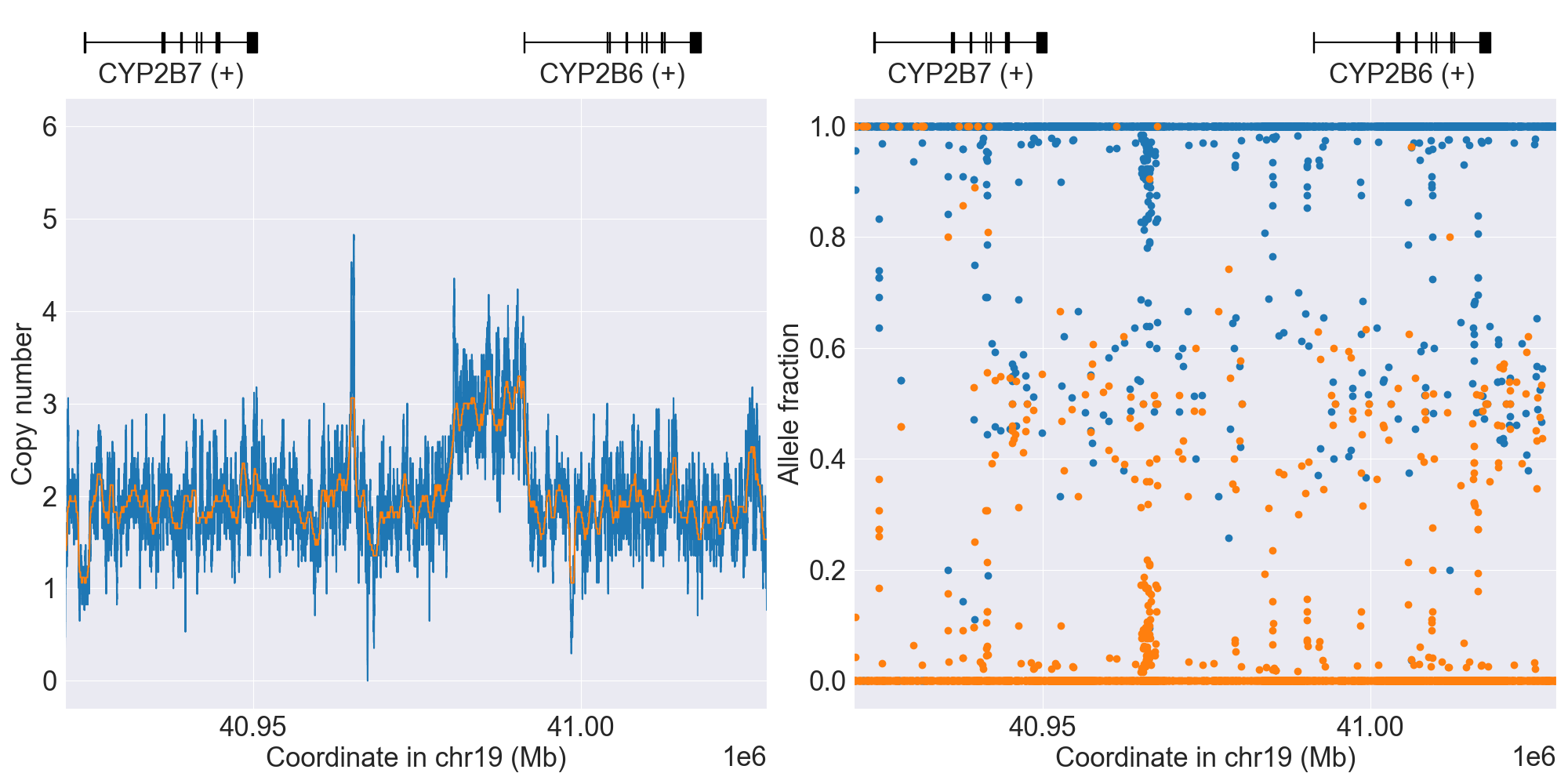
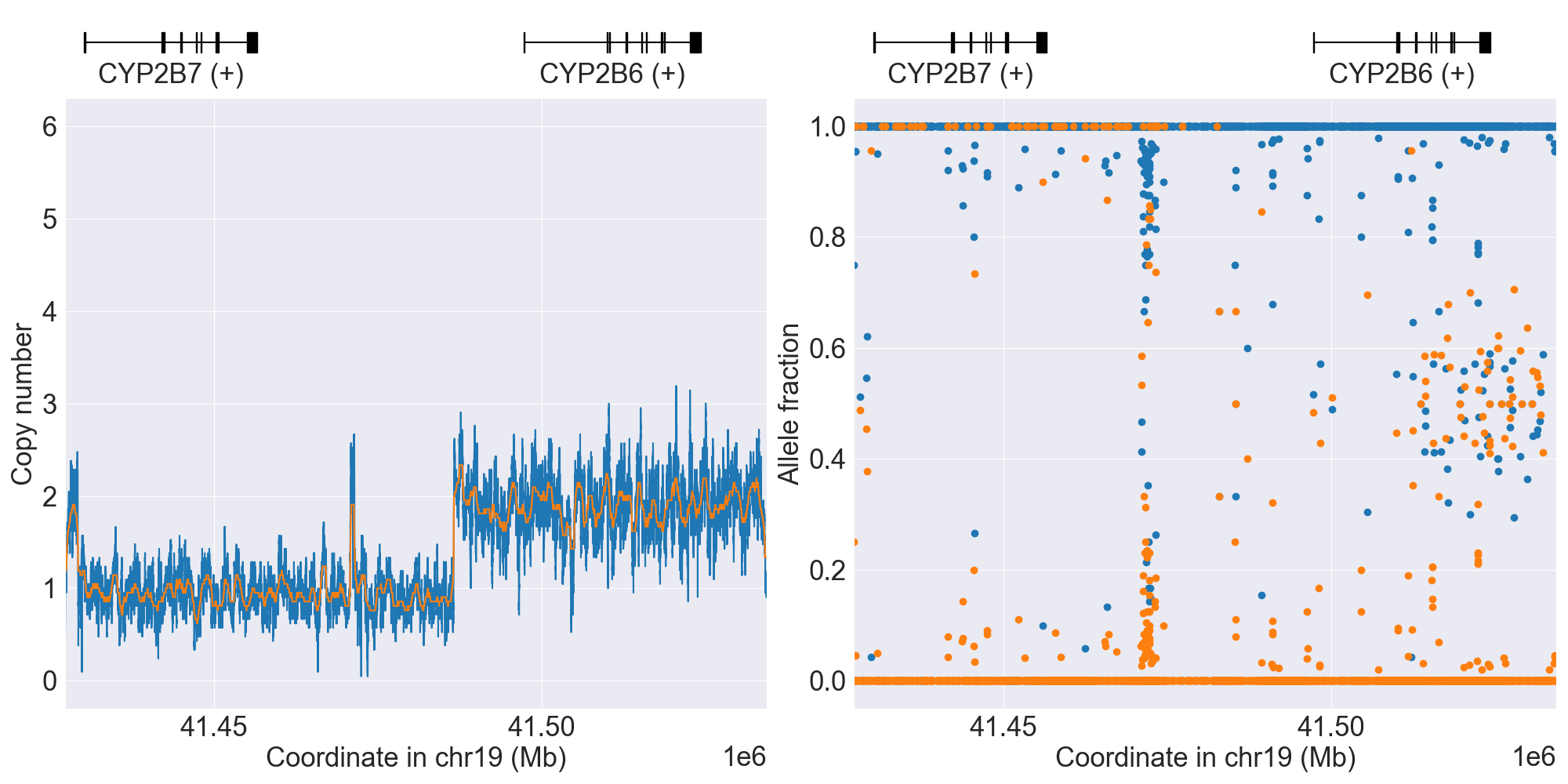
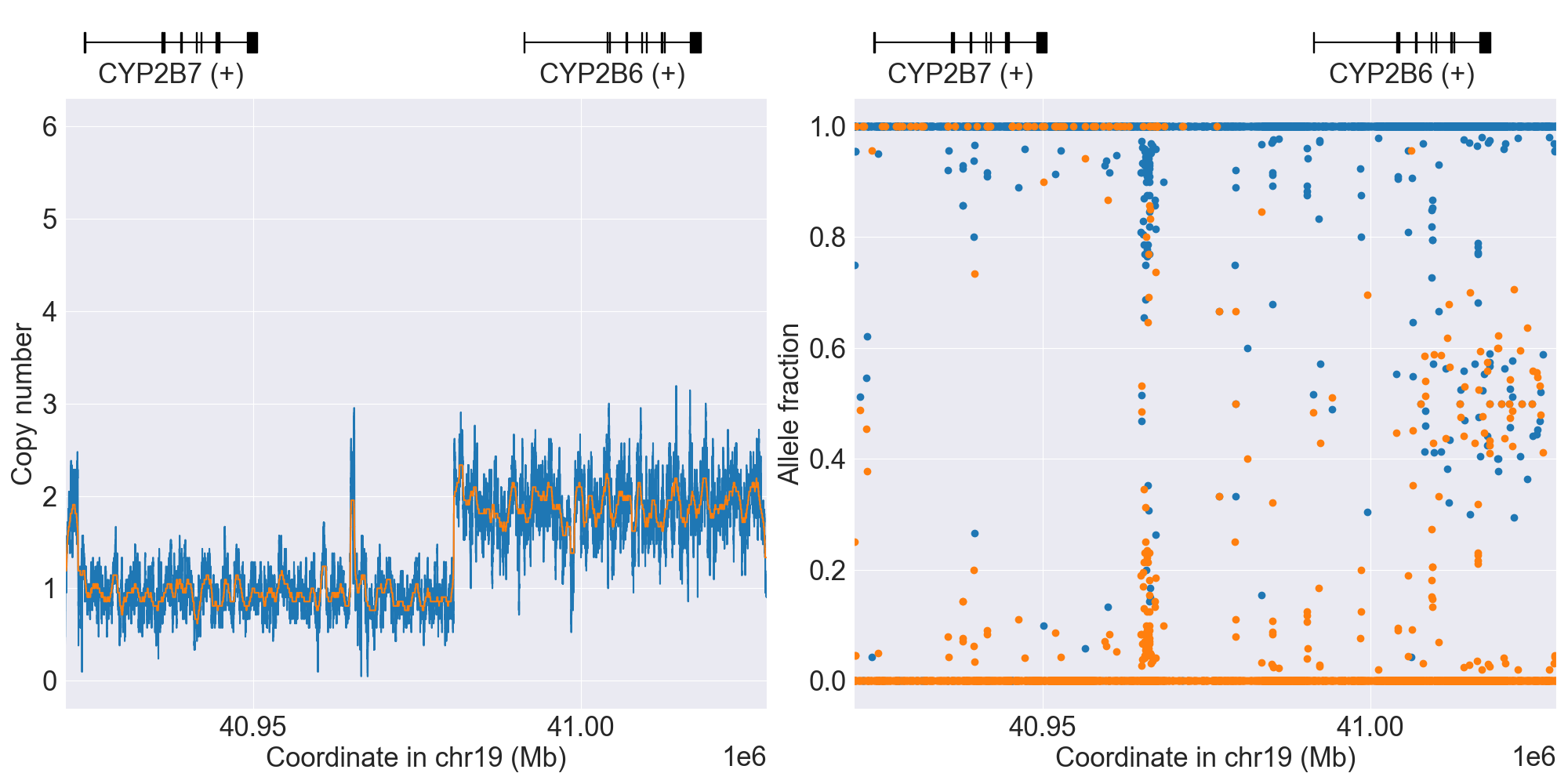
CYP2B6
SV summary for CYP2B6
Below is comprehensive summary of SV described from real NGS studies:
SV Alleles |
SV Name |
Genotype |
Reference |
Gene Model |
GRCh37 |
GRCh38 |
Data Type |
Source |
Coriell ID |
Version |
Description |
|---|---|---|---|---|---|---|---|---|---|---|---|
Normal |
*1/*2 |
WGS |
NA12813 |
0.4.1 |
|||||||
*22x2 |
WholeDup1 |
*6/*22x2 |
WGS |
NA19190 |
0.12.0 |
||||||
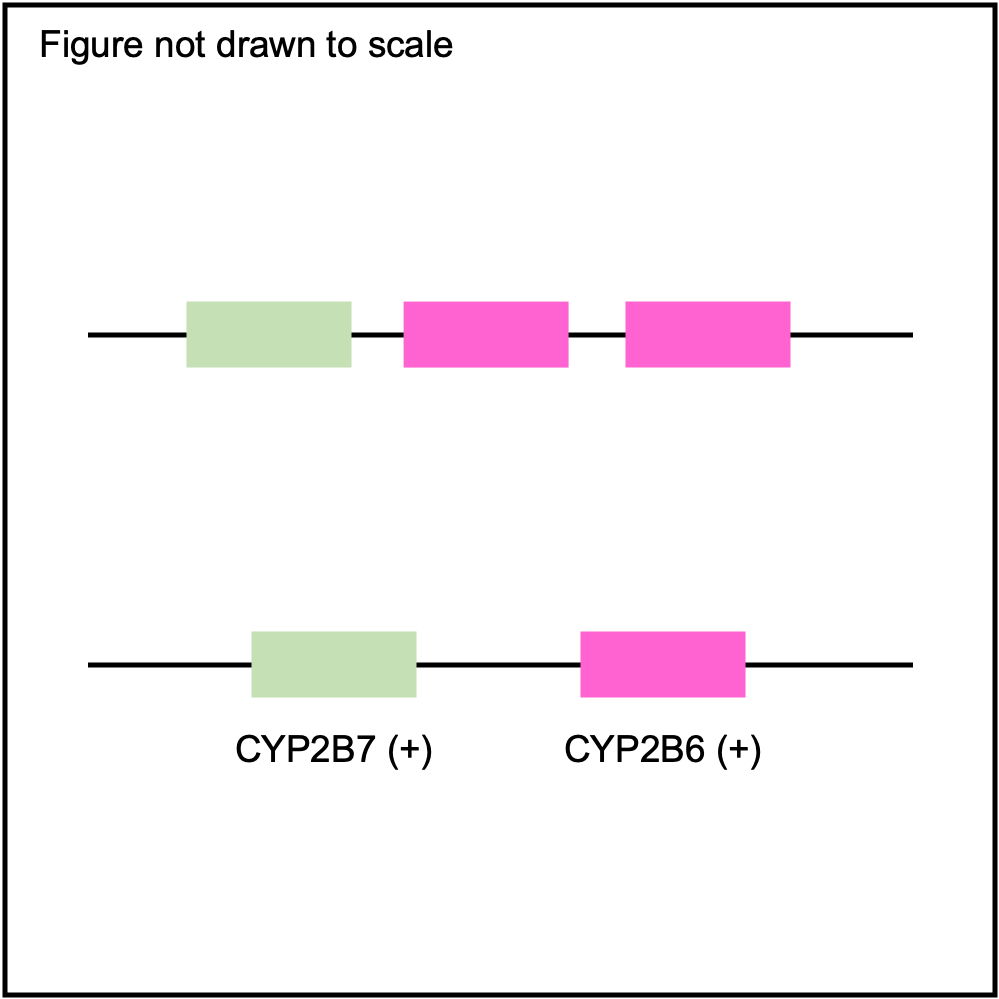
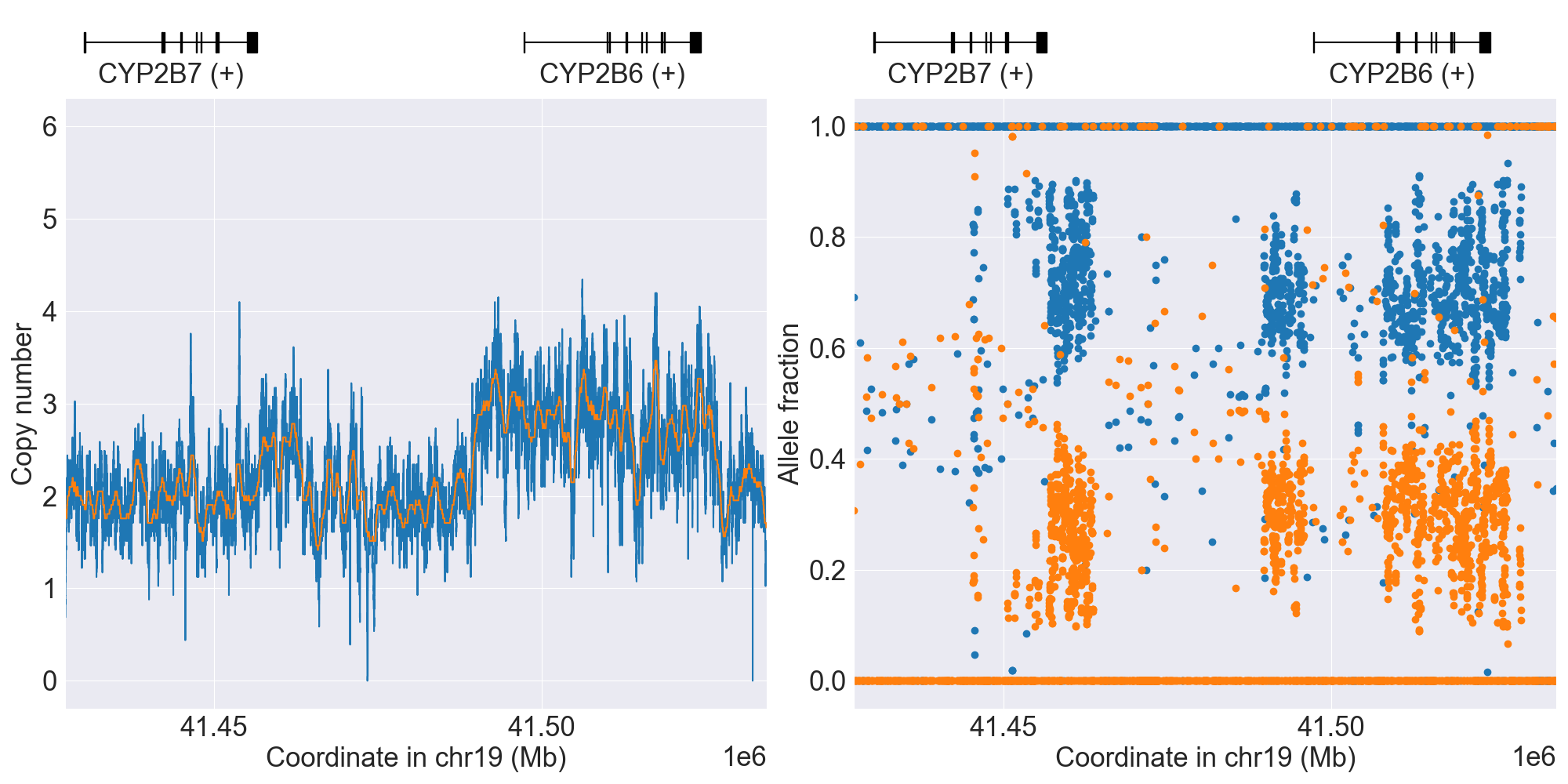
*29 |
Hybrid1 |
*6/*29 |
WGS |
NA19178 |
0.4.1 |
*29 has exons 1-4 of CYP2B7 origin and exons 5-9 of CYP2A6 origin (breakpoint in intron 4). |
|||||
Tandem1 |
Indeterminate |
WGS |
HG01806 |
0.16.0 |
|||||||
PartialDup1 |
Indeterminate |
WGS |
HG03784 |
0.16.0 |
|||||||
PartialDup2 |
Indeterminate |
WGS |
HG02790 |
0.16.0 |
|||||||
ParalogWholeDel1 |
Indeterminate |
WGS |
HG03235 |
0.16.0 |
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
PyPGx was recently applied to the entire high-coverage WGS dataset from 1KGP (N=2,504). Click here to see individual SV calls for CYP2B6, and corresponding copy number profiles and allele fraction profiles.
Phenotype summary for CYP2B6
Diplotype-phenotype mapping is used for phenotype prediction.
Phenotype
Example
Priority
Ultrarapid Metabolizer
*4/*4
Normal/Routine/Low Risk
Rapid Metabolizer
*1/*4
Normal/Routine/Low Risk
Normal Metabolizer
*1/*2
Normal/Routine/Low Risk
Intermediate Metabolizer
*1/*29
Abnormal/Priority/High Risk
Poor Metabolizer
*6/*6
Abnormal/Priority/High Risk
Indeterminate
*1/*3
None
Recommendations for CYP2B6
Efavirenz
“Consider initiating efavirenz with a decreased dose of either 400 or 200 mg/day for patients who are CYP2B6 poor metabolizers. Consider initiating efavirenz with a decreased dose of 400 mg/day for patients who are CYP2B6 intermediate metabolizers.” (Source: PharmGKB)
Resources for CYP2B6
CYP2C8
Resources for CYP2C8
CYP2C9
Phenotype summary for CYP2C9
Activity score is used for phenotype prediction.
Phenotype |
Activity Score |
Example |
Priority |
|---|---|---|---|
Normal Metabolizer |
2 == score |
*1/*1 |
Normal/Routine/Low Risk |
Intermediate Metabolizer |
1 <= score < 2 |
*1/*2 |
Abnormal/Priority/High Risk |
Poor Metabolizer |
0 <= score < 1 |
*2/*3 |
Abnormal/Priority/High Risk |
Indeterminate |
Unknown score |
*1/*7 |
Normal/Routine/Low Risk |
Recommendations for CYP2C9
Celecoxib
“The CPIC Dosing Guideline for celecoxib, flurbiprofen, ibuprofen and lornoxicam recommends initiating therapy with 25-50% of the lowest recommended starting dose for CYP2C9 poor metabolizers and initiating therapy with lowest recommended starting dose for CYP2C9 intermediate metabolizers with activity score of 1. See full guideline for further details and supporting evidence.” (Source: PharmGKB)
Flurbiprofen
“The CPIC Dosing Guideline for celecoxib, flurbiprofen, ibuprofen and lornoxicam recommends initiating therapy with 25-50% of the lowest recommended starting dose for CYP2C9 poor metabolizers and initiating therapy with lowest recommended starting dose for CYP2C9 intermediate metabolizers with activity score of 1. See full guideline for further details and supporting evidence.” (Source: PharmGKB)
Fluvastatin
“CYP2C9 IMs should avoid fluvastatin doses greater than 40mg while CYP2C9 PMs should avoid doses greater than 20mg. If higher doses are required for desired efficacy, an alternative statin should be considered. Patients with SLCO1B1 poor function should also avoid fluvastatin doses greater than 40mg and and adjust doses of fluvastatin based on disease-specific guidelines. Patients with both SLCO1B1 poor function and CYP2C9 IM/PM should be prescribed an alternative statin depending on the desired potency.” (Source: PharmGKB)
Ibuprofen
“The CPIC Dosing Guideline for celecoxib, flurbiprofen, ibuprofen and lornoxicam recommends initiating therapy with 25-50% of the lowest recommended starting dose for CYP2C9 poor metabolizers and initiating therapy with lowest recommended starting dose for CYP2C9 intermediate metabolizers with activity score of 1. See full guideline for further details and supporting evidence.” (Source: PharmGKB)
Lornoxicam
“The CPIC Dosing Guideline for celecoxib, flurbiprofen, ibuprofen and lornoxicam recommends initiating therapy with 25-50% of the lowest recommended starting dose for CYP2C9 poor metabolizers and initiating therapy with lowest recommended starting dose for CYP2C9 intermediate metabolizers with activity score of 1. See full guideline for further details and supporting evidence.” (Source: PharmGKB)
Meloxicam
“The CPIC Dosing Guideline for meloxicam recommends alternative therapy for CYP2C9 poor metabolizers due to markedly prolonged half-life, and initiating therapy with 50% of the lowest recommended starting dose or choose an alternative therapy for CYP2C9 intermediate metabolizers with activity score of 1. See full guideline for further details and supporting evidence.” (Source: PharmGKB)
Piroxicam
“The CPIC Dosing Guideline for piroxicam recommends that CYP2C9 poor metabolizers and intermediate metabolizers with activity score of 1 should choose an alternative therapy not metabolized by CYP2C9 or not significantly impacted by CYP2C9 genetic variants in vivo or choose an NSAID metabolized by CYP2C9 but with a shorter half-life. See full guideline for further details and supporting evidence.” (Source: PharmGKB)
Tenoxicam
“The CPIC Dosing Guideline for tenoxicam recommends that CYP2C9 poor metabolizers and intermediate metabolizers with activity score of 1 should choose an alternative therapy not metabolized by CYP2C9 or not significantly impacted by CYP2C9 genetic variants in vivo or choose an NSAID metabolized by CYP2C9 but with a shorter half-life. See full guideline for further details and supporting evidence.” (Source: PharmGKB)
Resources for CYP2C9
CYP2C19
Phenotype summary for CYP2C19
Diplotype-phenotype mapping is used for phenotype prediction.
Phenotype |
Example |
Priority |
|---|---|---|
Ultrarapid Metabolizer |
*17/*17 |
Abnormal/Priority/High Risk |
Rapid Metabolizer |
*1/*17 |
Abnormal/Priority/High Risk |
Normal Metabolizer |
*1/*1 |
Normal/Routine/Low Risk |
Likely Intermediate Metabolizer |
*1/*10 |
Abnormal/Priority/High Risk |
Intermediate Metabolizer |
*1/*2 |
Abnormal/Priority/High Risk |
Likely Poor Metabolizer |
*10/*22 |
Abnormal/Priority/High Risk |
Poor Metabolizer |
*2/*2 |
Abnormal/Priority/High Risk |
Indeterminate |
*1/*12 |
None |
Recommendations for CYP2C19
Amitriptyline
“The CPIC Dosing Guideline update for amitriptyline recommends an alternative drug for CYP2D6 ultrarapid or poor metabolizers and CYP2C19 ultrarapid, rapid or poor metabolizers. If amitriptyline is warranted, consider a 50% dose reduction in CYP2D6 or CYP2C19 poor metabolizers. For CYP2D6 intermediate metabolizers, a 25% dose reduction should be considered.” (Source: PharmGKB)
Citalopram
“The CPIC Dosing Guideline for the selective serotonin reuptake inhibitors citalopram and escitalopram recommends an alternative drug not predominantly metabolized by CYP2C19 for CYP2C19 ultrarapid metabolizers. For CYP2C19 poor metabolizers, consider a 50% reduction of recommended starting dose and titrate to response or select alternative drug not predominantly metabolized by CYP2C19.” (Source: PharmGKB)
Clomipramine
“Tricyclic antidepressants have comparable pharmacokinetic properties, it may be reasonable to apply the CPIC Dosing Guideline for amitriptyline and CYP2C19, CYP2D6 to other tricyclics including clomipramine. The CPIC Dosing Guideline update for amitriptyline recommends an alternative drug for CYP2D6 ultrarapid or poor metabolizers and CYP2C19 ultrarapid, rapid or poor metabolizers. If amitriptyline is warranted, consider a 50% dose reduction in CYP2D6 or CYP2C19 poor metabolizers. For CYP2D6 intermediate metabolizers, a 25% dose reduction should be considered.” (Source: PharmGKB)
Clopidogrel
“The CPIC Dosing Guideline for clopidogrel recommends an alternative antiplatelet therapy for CYP2C19 poor or intermediate metabolizers (cardiovascular indications: prasugrel or ticagrelor if no contraindication; neurovascular indications: alternative P2Y12 inhibitor if clinically indicated and no contraindication.)” (Source: PharmGKB)
Dexlansoprazole
“The CPIC Dosing Guideline recommendations for dexlansoprazole are based on the similarity in its metabolism and lansoprazole and extrapolated from the first-generation PPIs. The guideline recommends to increase the starting daily dose and to monitor efficacy in CYP2C19 ultrarapid metabolizer. For CYP2C19 rapid and normal metabolizers in the treatment of H. pylori infection and erosive esophagitis increasing the dose might be considered after initiation with the standard starting daily dose. The recommendations for intermediate and poor metabolizers for chronic therapy (>12 weeks) and efficacy achieved is to consider 50% reduction in daily dose. See full guideline for further details and supporting evidence.” (Source: PharmGKB)
Doxepin
“Tricyclic antidepressants have comparable pharmacokinetic properties, it may be reasonable to apply the CPIC Dosing Guideline for amitriptyline and CYP2C19, CYP2D6 to other tricyclics including doxepin. The CPIC Dosing Guideline update for amitriptyline recommends an alternative drug for CYP2D6 ultrarapid or poor metabolizers and CYP2C19 ultrarapid, rapid or poor metabolizers. If amitriptyline is warranted, consider a 50% dose reduction in CYP2D6 or CYP2C19 poor metabolizers. For CYP2D6 intermediate metabolizers, a 25% dose reduction should be considered.” (Source: PharmGKB)
Escitalopram
“The CPIC Dosing Guideline for the selective serotonin reuptake inhibitors citalopram and escitalopram recommends an alternative drug not predominantly metabolized by CYP2C19 for CYP2C19 ultrarapid metabolizers. For CYP2C19 poor metabolizers, consider a 50% reduction of recommended starting dose and titrate to response or select alternative drug not predominantly metabolized by CYP2C19.” (Source: PharmGKB)
Imipramine
“Tricyclic antidepressants have comparable pharmacokinetic properties, it may be reasonable to apply the CPIC Dosing Guideline for amitriptyline and CYP2C19, CYP2D6 to other tricyclics including imipramine. The CPIC Dosing Guideline update for amitriptyline recommends an alternative drug for CYP2D6 ultrarapid or poor metabolizers and CYP2C19 ultrarapid, rapid or poor metabolizers. If amitriptyline is warranted, consider a 50% dose reduction in CYP2D6 or CYP2C19 poor metabolizers. For CYP2D6 intermediate metabolizers, a 25% dose reduction should be considered.” (Source: PharmGKB)
Lansoprazole
“The CPIC Dosing Guideline for omeprazole, lansoprazole, pantoprazole recommends to increase the starting daily dose and to monitor efficacy in CYP2C19 ultrarapid metabolizer. For CYP2C19 rapid and normal metabolizers in the treatment of H. pylori infection and erosive esophagitis increasing the dose might be considered after initiation with the standard starting daily dose. The recommendations for intermediate and poor metabolizer for chronic therapy (>12 weeks) and efficacy achieved is to consider 50% reduction in daily dose. See full guideline for further details and supporting evidence.” (Source: PharmGKB)
Omeprazole
“The CPIC Dosing Guideline for omeprazole, lansoprazole, pantoprazole recommends to increase the starting daily dose and to monitor efficacy in CYP2C19 ultrarapid metabolizer. For CYP2C19 rapid and normal metabolizers in the treatment of H. pylori infection and erosive esophagitis increasing the dose might be considered after initiation with the standard starting daily dose. The recommendations for intermediate and poor metabolizer for chronic therapy (>12 weeks) and efficacy achieved is to consider 50% reduction in daily dose. See full guideline for further details and supporting evidence.” (Source: PharmGKB)
Pantoprazole
“The CPIC Dosing Guideline for omeprazole, lansoprazole, pantoprazole recommends to increase the starting daily dose and to monitor efficacy in CYP2C19 ultrarapid metabolizer. For CYP2C19 rapid and normal metabolizers in the treatment of H. pylori infection and erosive esophagitis increasing the dose might be considered after initiation with the standard starting daily dose. The recommendations for intermediate and poor metabolizer for chronic therapy (>12 weeks) and efficacy achieved is to consider 50% reduction in daily dose. See full guideline for further details and supporting evidence.” (Source: PharmGKB)
Sertraline
“The CPIC Dosing Guideline for the selective serotonin reuptake inhibitor sertraline recommends to consider a 50% reduction of recommended starting dose and titrate to response or select alternative drug not predominantly metabolized by CYP2C19 for CYP2C19 poor metabolizers.” (Source: PharmGKB)
Voriconazole
“The CPIC dosing guideline for voriconazole recommends selecting an alternative agent that is not dependent on CYP2C19 metabolism in adults who are CYP2C19 ultrarapid metabolizers, rapid metabolizers or poor metabolizers. In pediatric patients, an alternative agent should be used in patients who are ultrarapid metabolizers or poor metabolizers. In pediatric rapid metabolizers, therapy should be initiated at recommended standard case dosing, then therapeutic dosing monitoring should be used to titrate dose to therapeutic trough concentrations.” (Source: PharmGKB)
Trimipramine
“Tricyclic antidepressants have comparable pharmacokinetic properties, it may be reasonable to apply the CPIC Dosing Guideline for amitriptyline and CYP2C19, CYP2D6 to other tricyclics including trimipramine. The CPIC Dosing Guideline update for amitriptyline recommends an alternative drug for CYP2D6 ultrarapid or poor metabolizers and CYP2C19 ultrarapid, rapid or poor metabolizers. If amitriptyline is warranted, consider a 50% dose reduction in CYP2D6 or CYP2C19 poor metabolizers. For CYP2D6 intermediate metabolizers, a 25% dose reduction should be considered.” (Source: PharmGKB)
Resources for CYP2C19
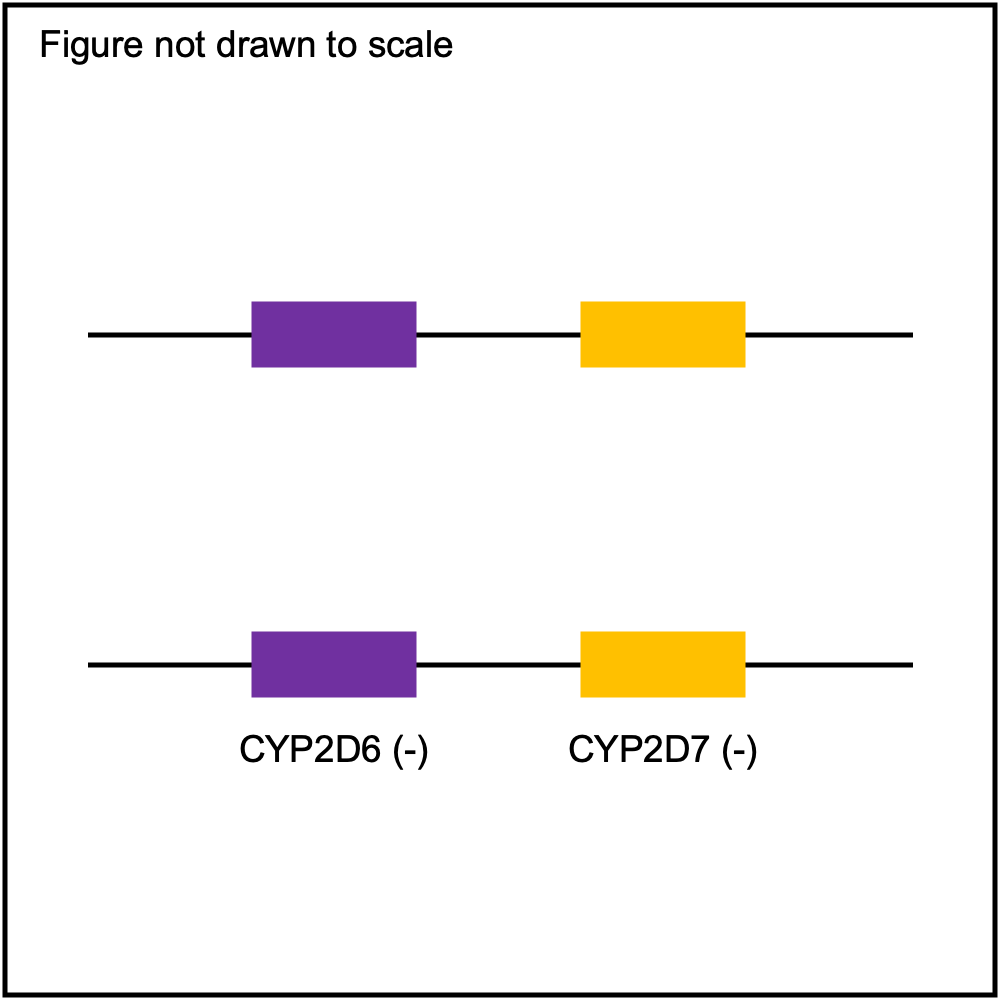
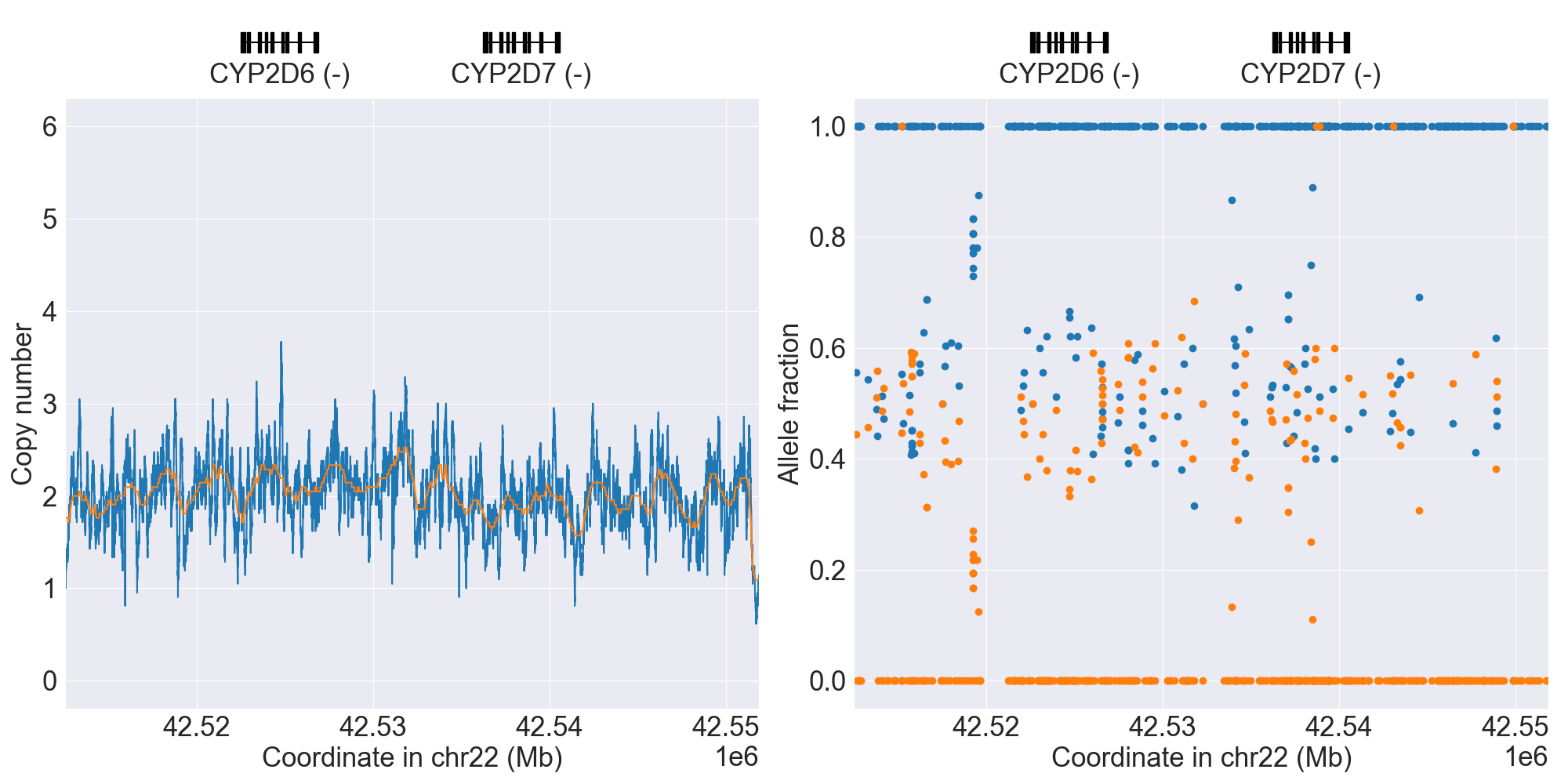
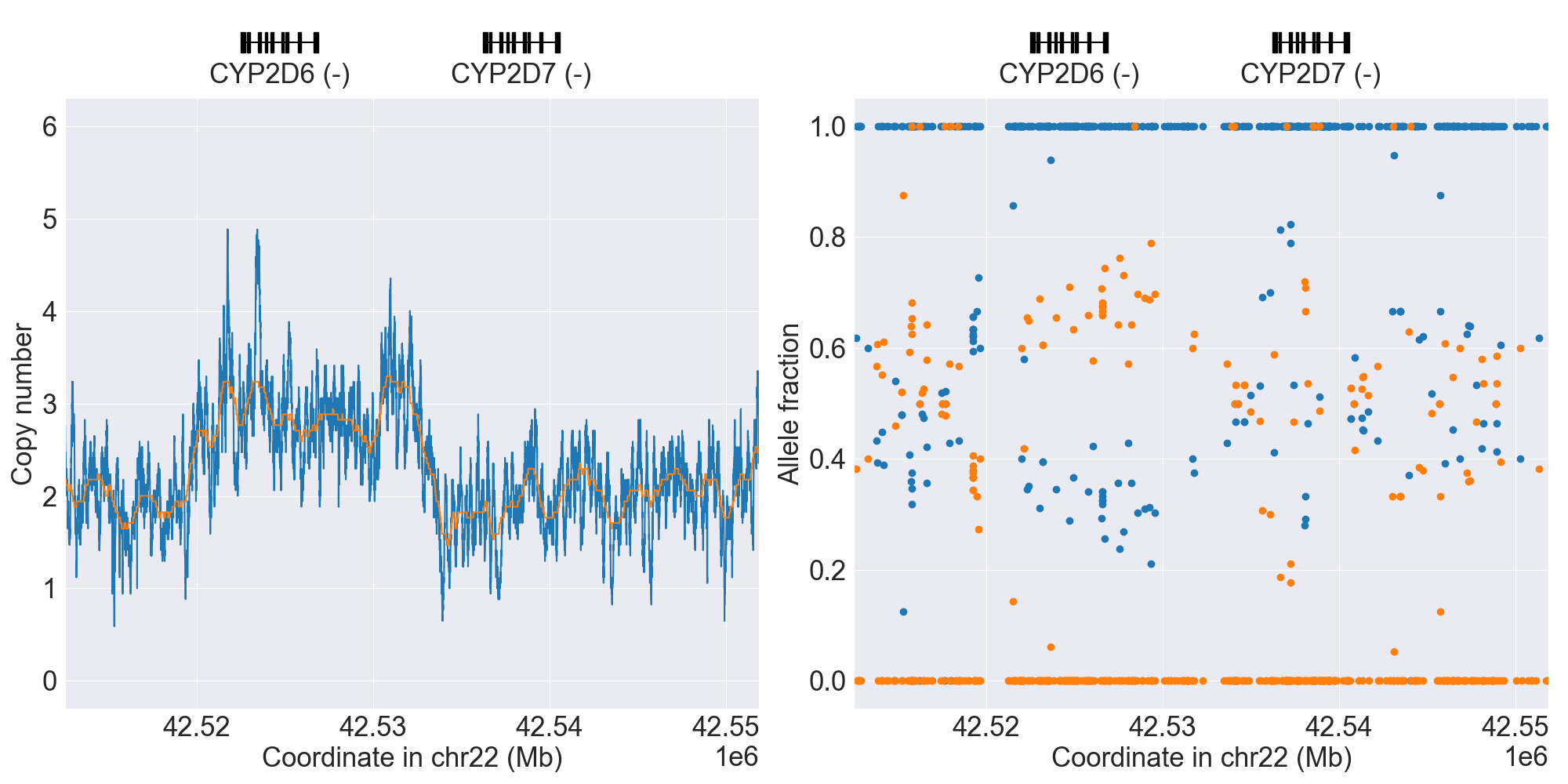
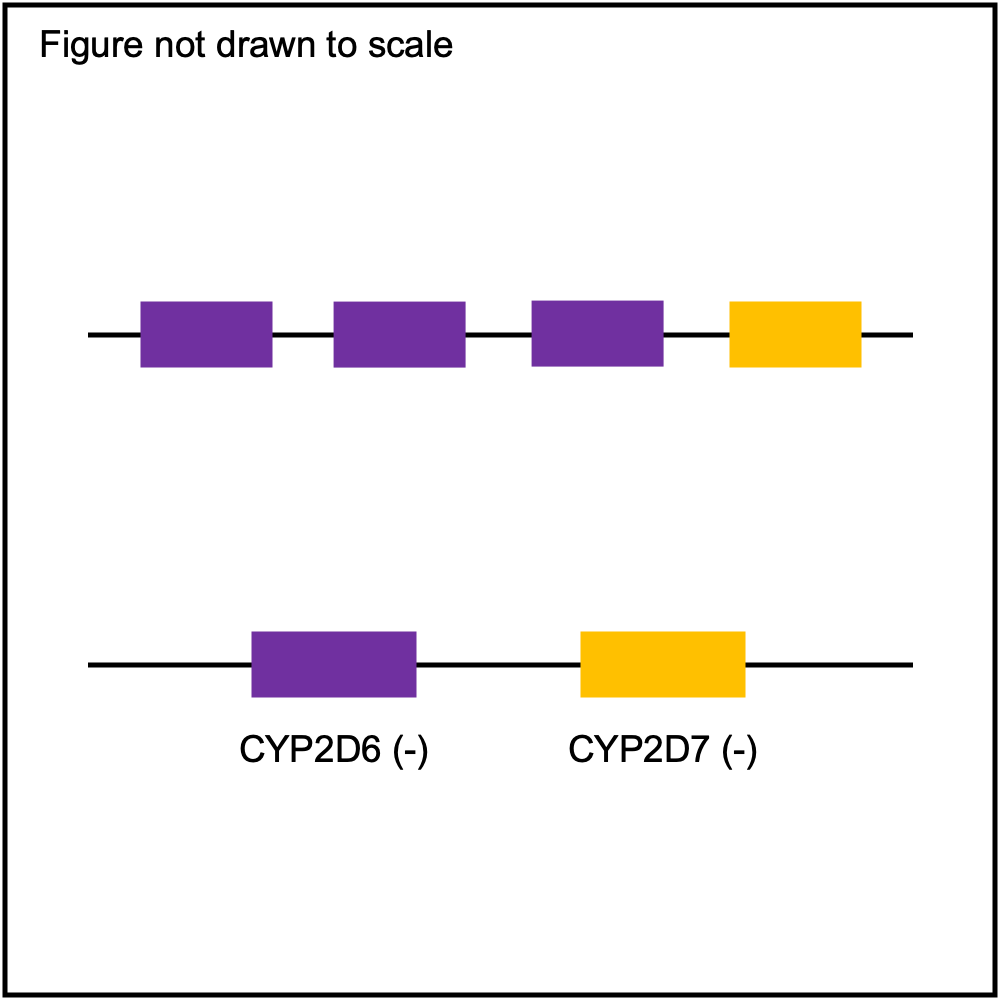
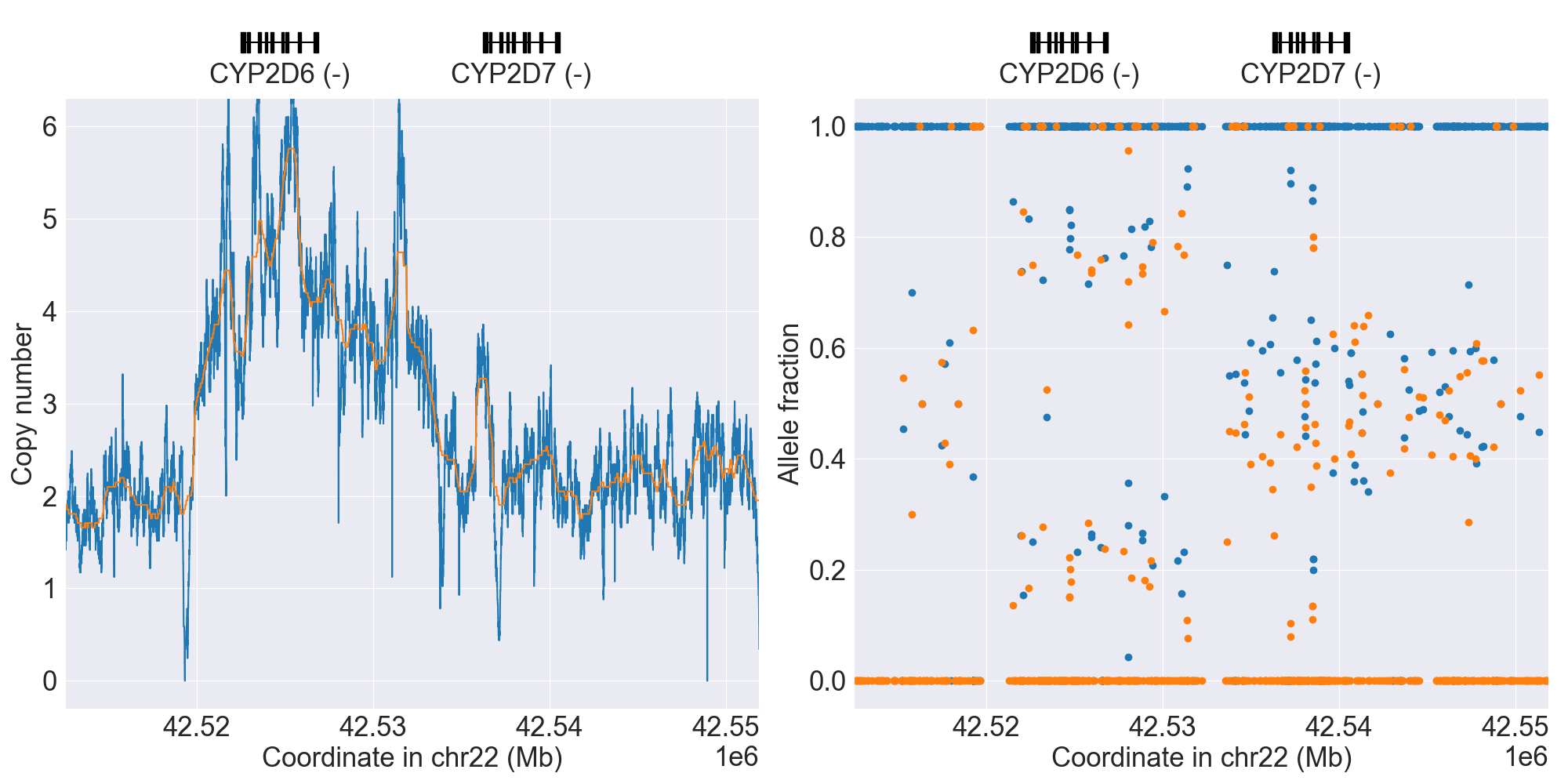
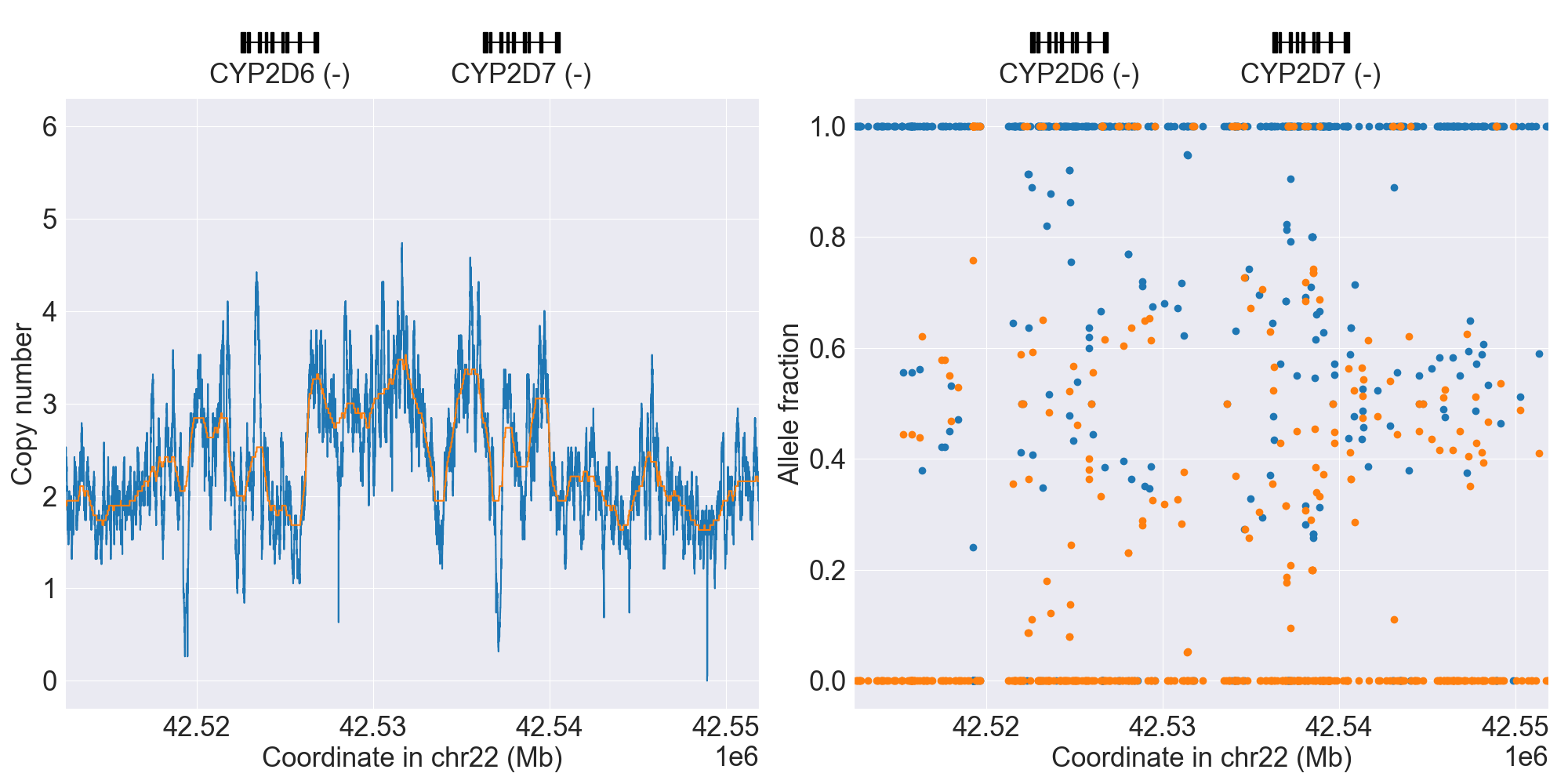
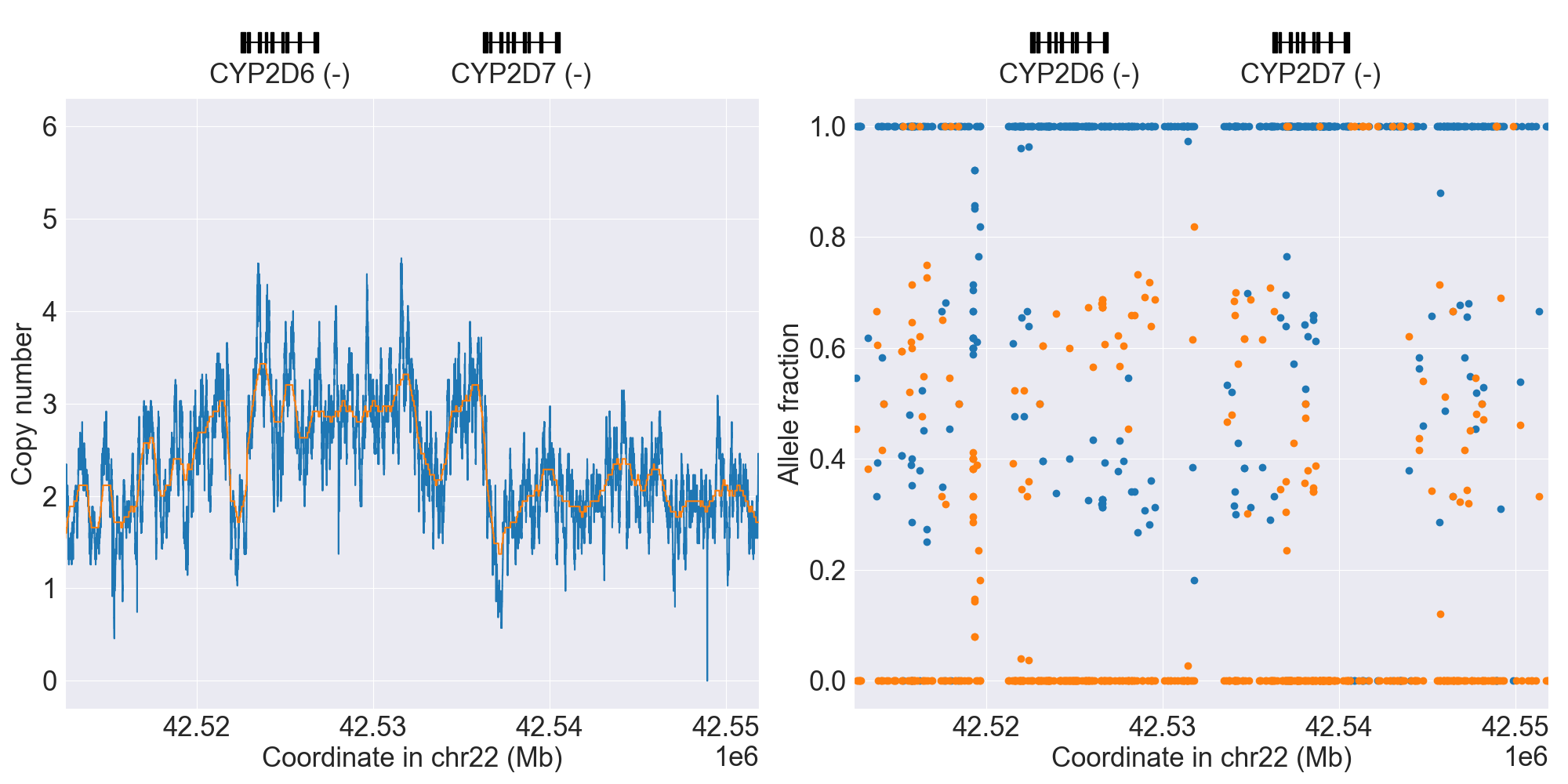
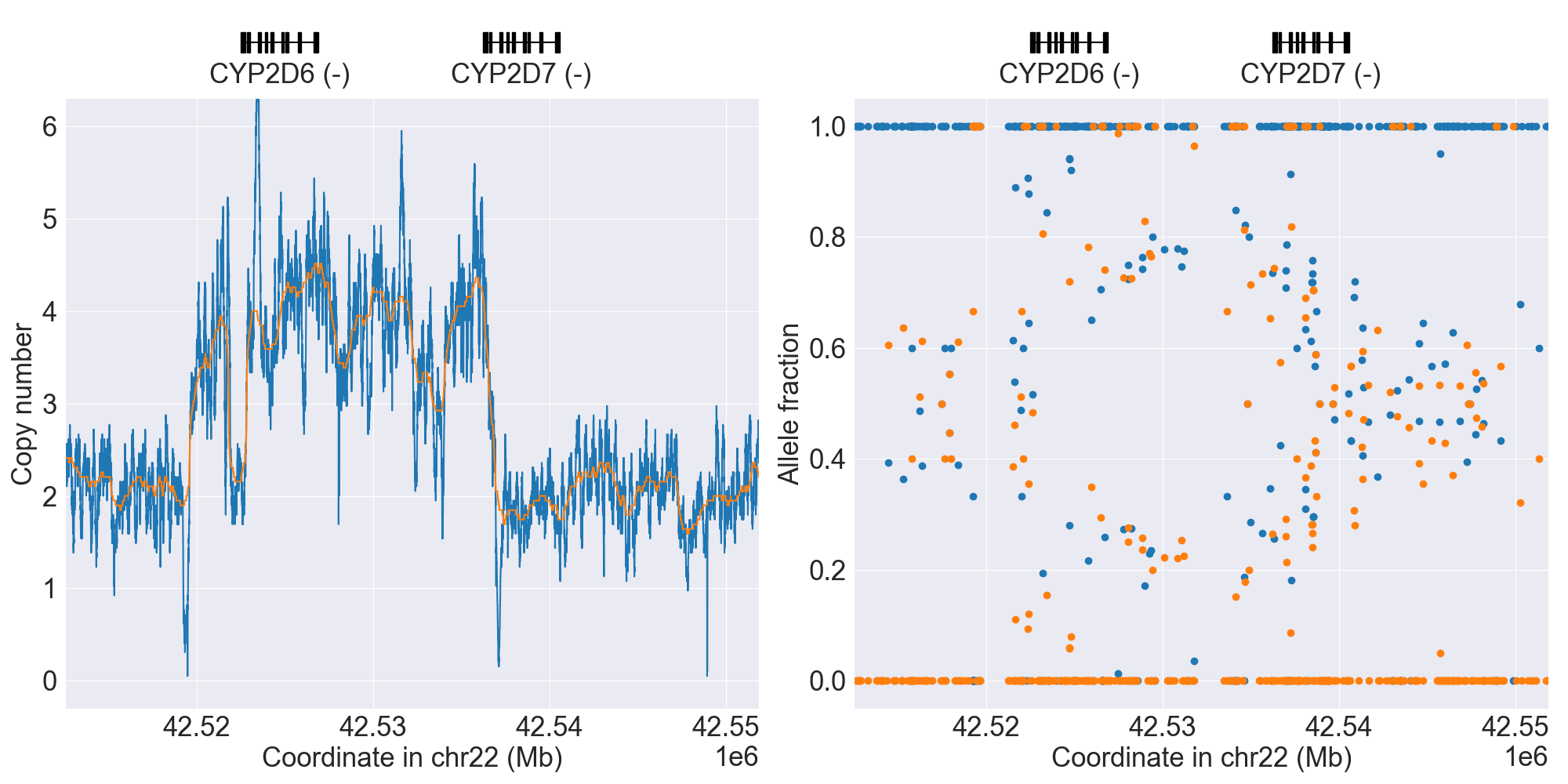
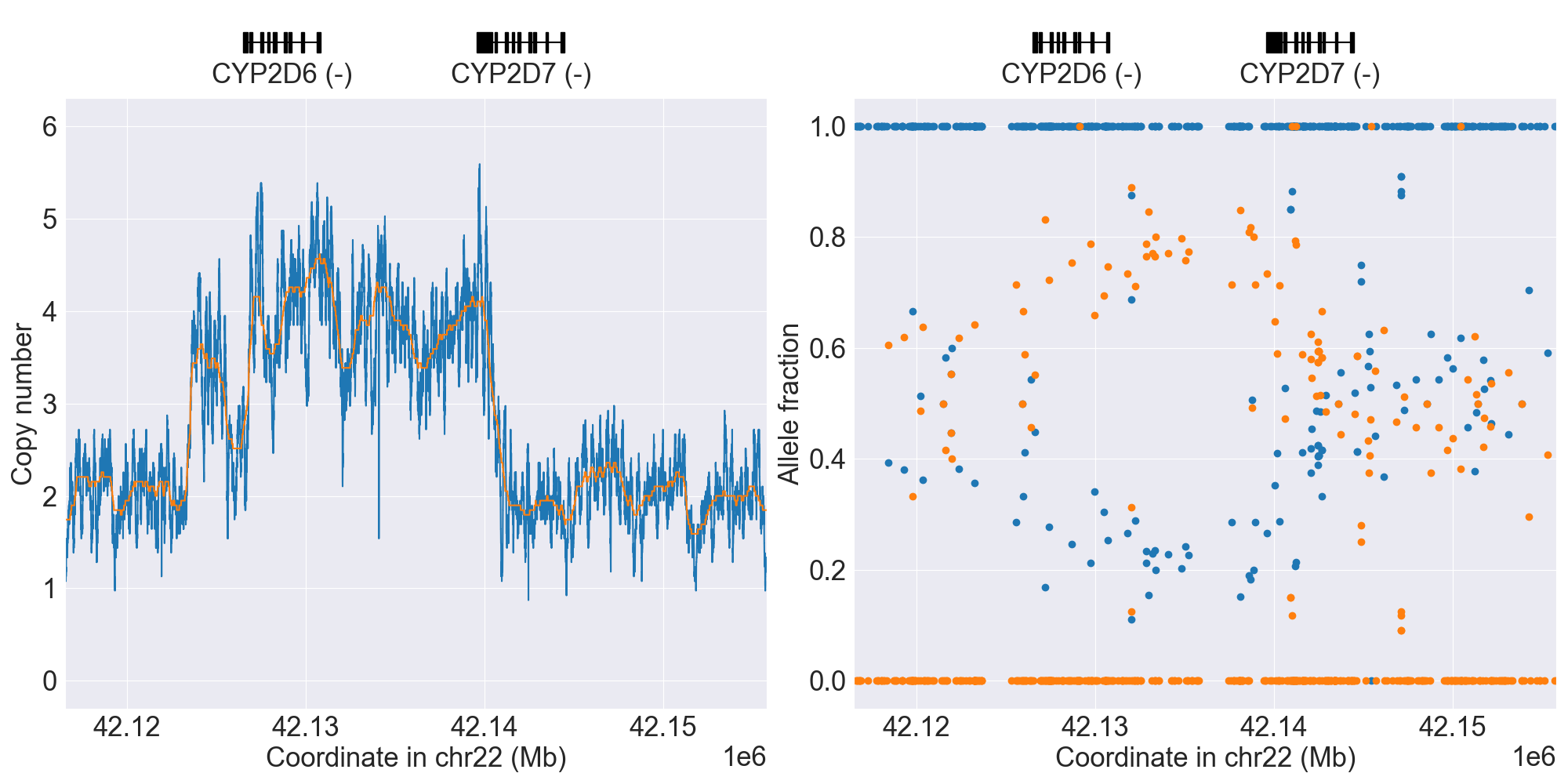
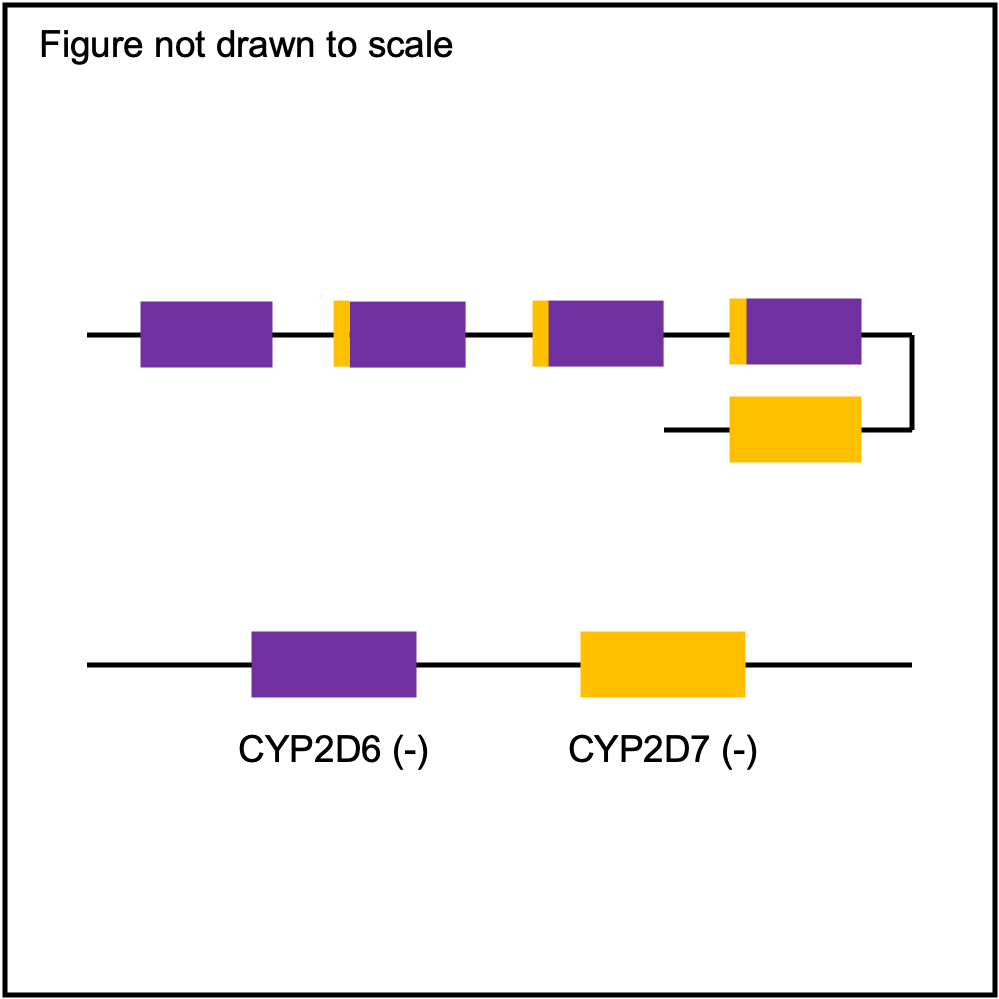
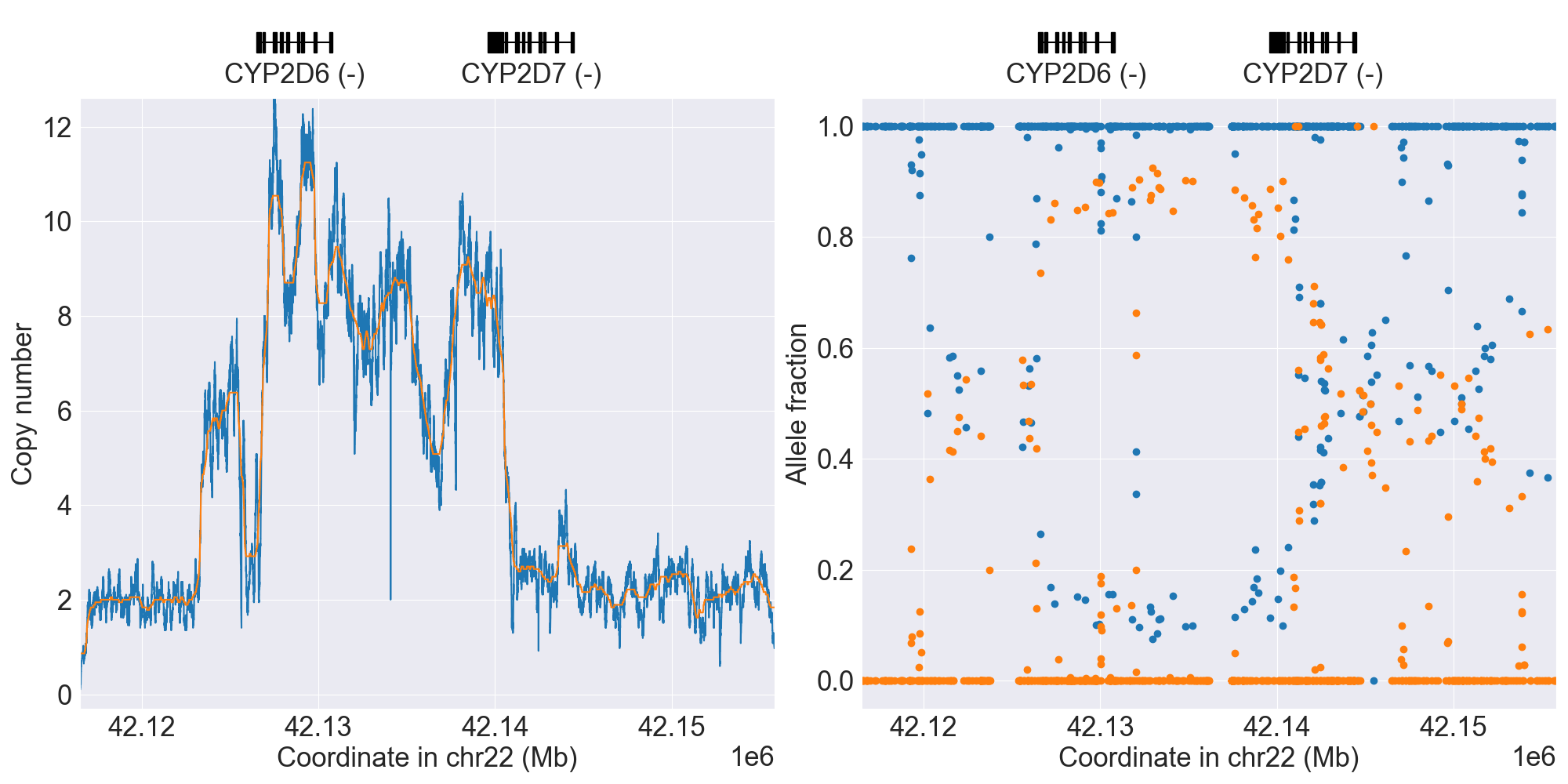
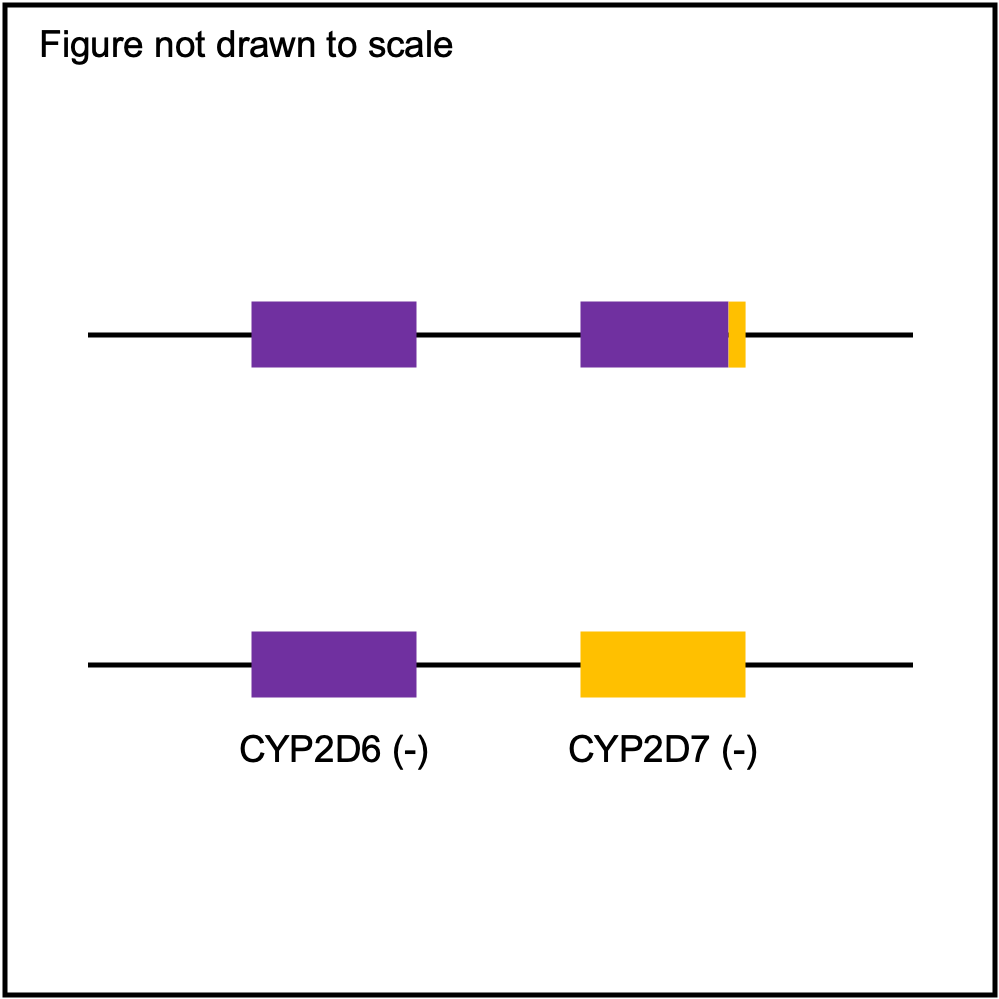
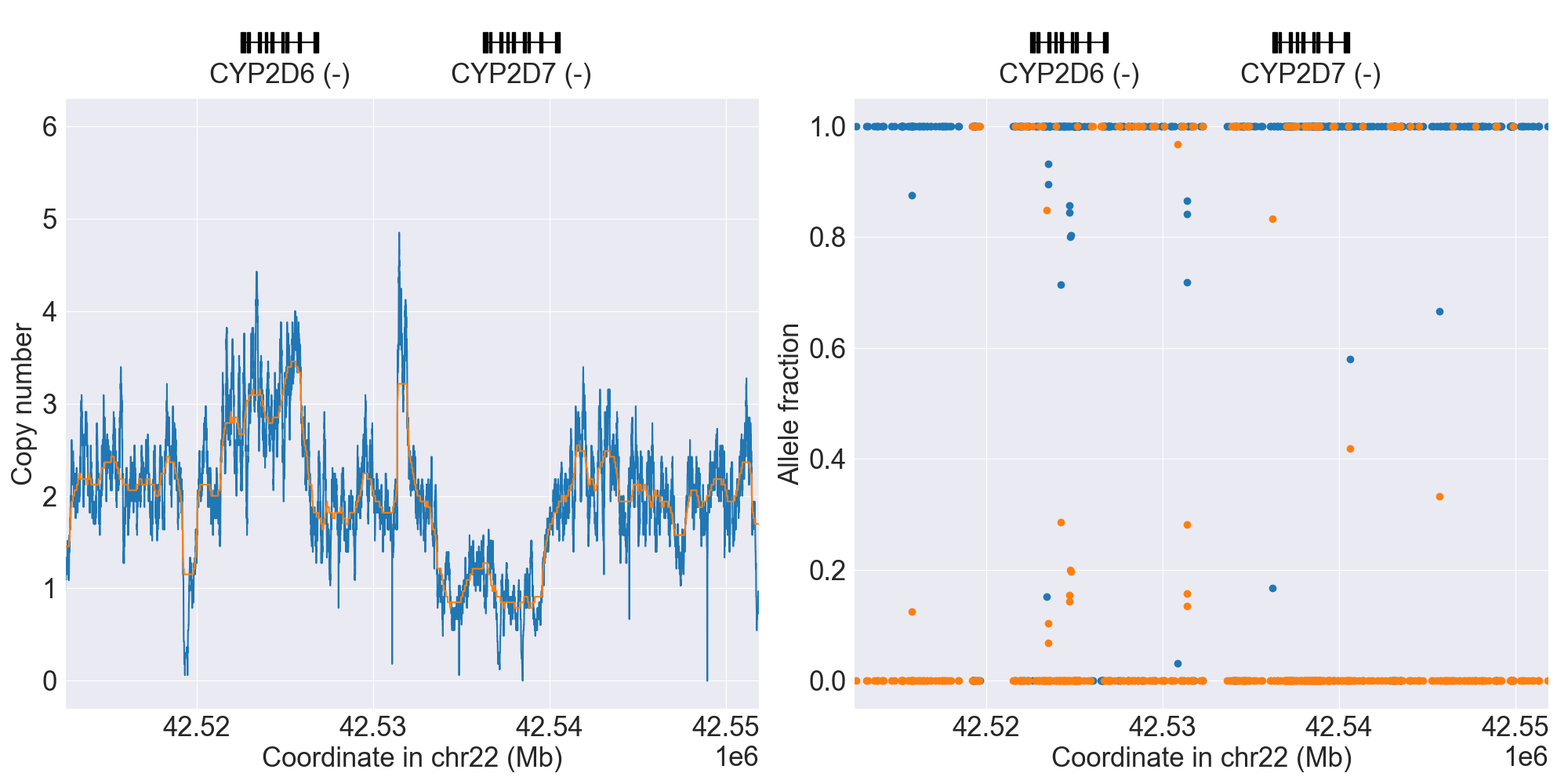
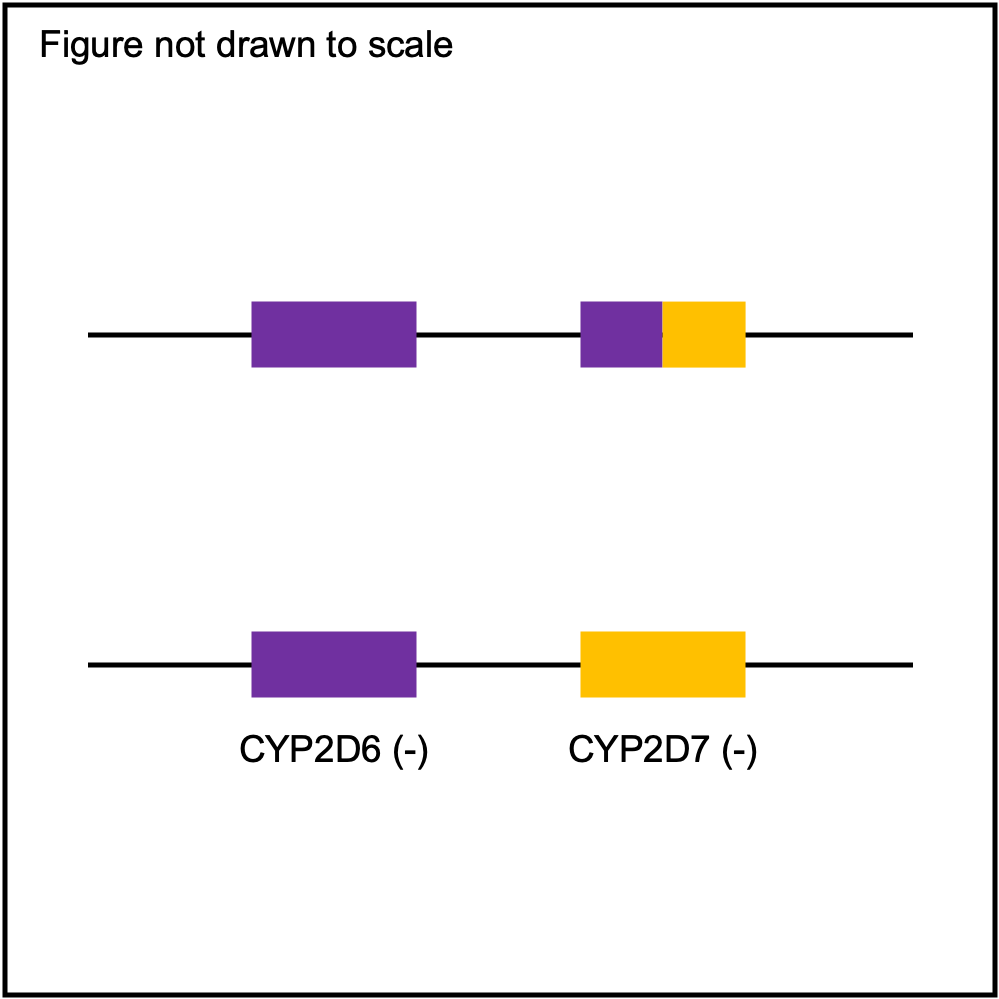
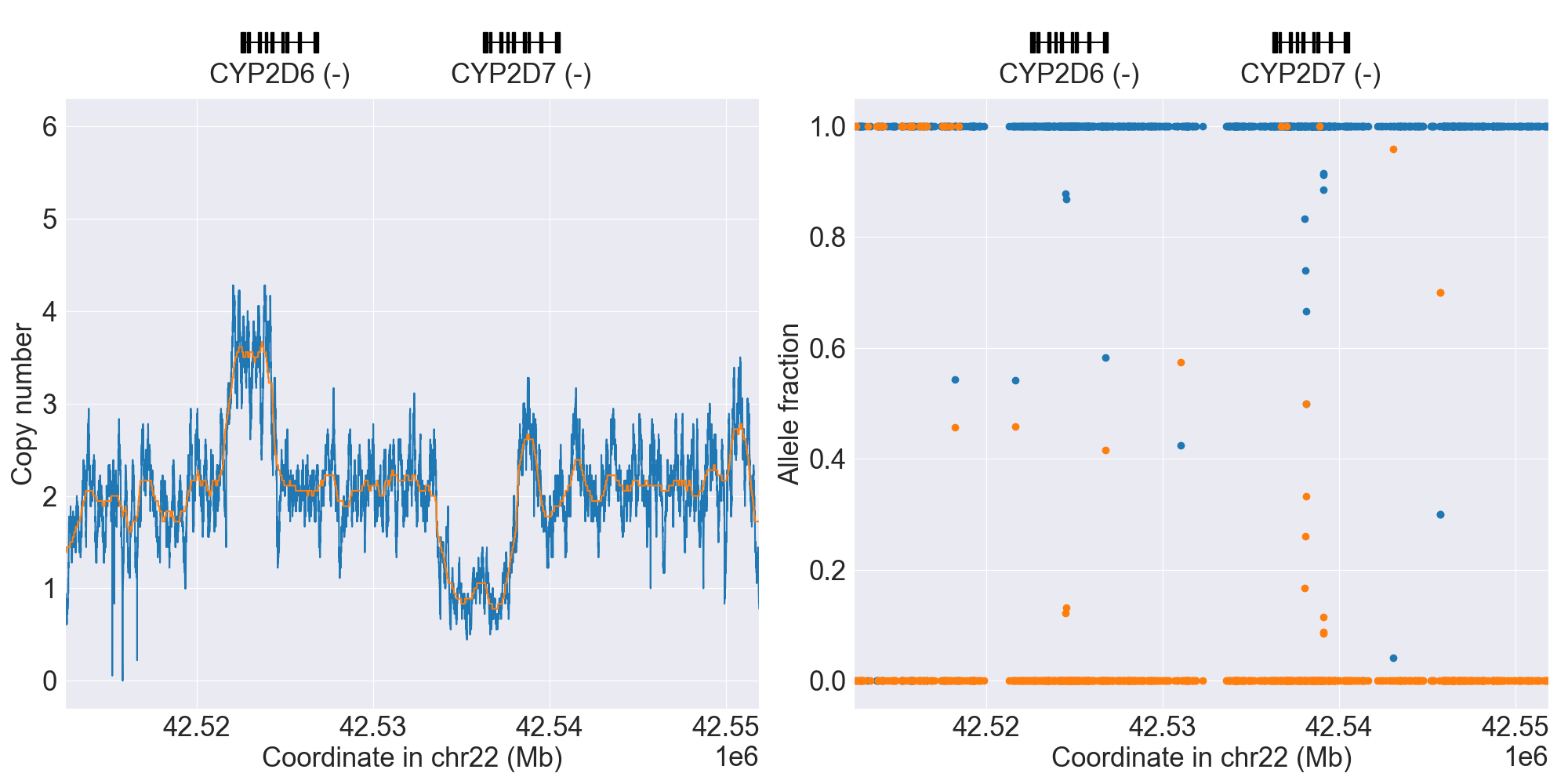
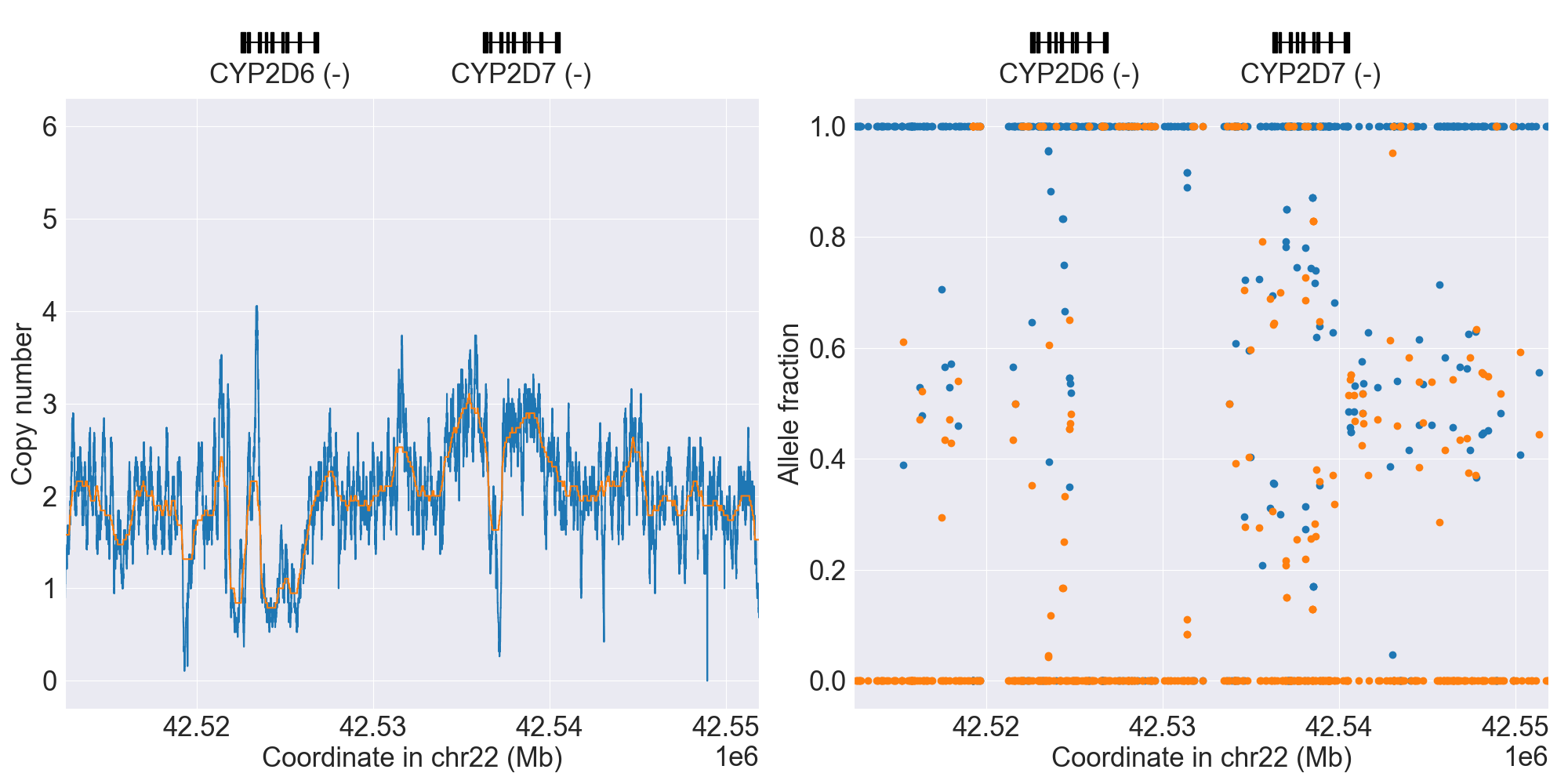
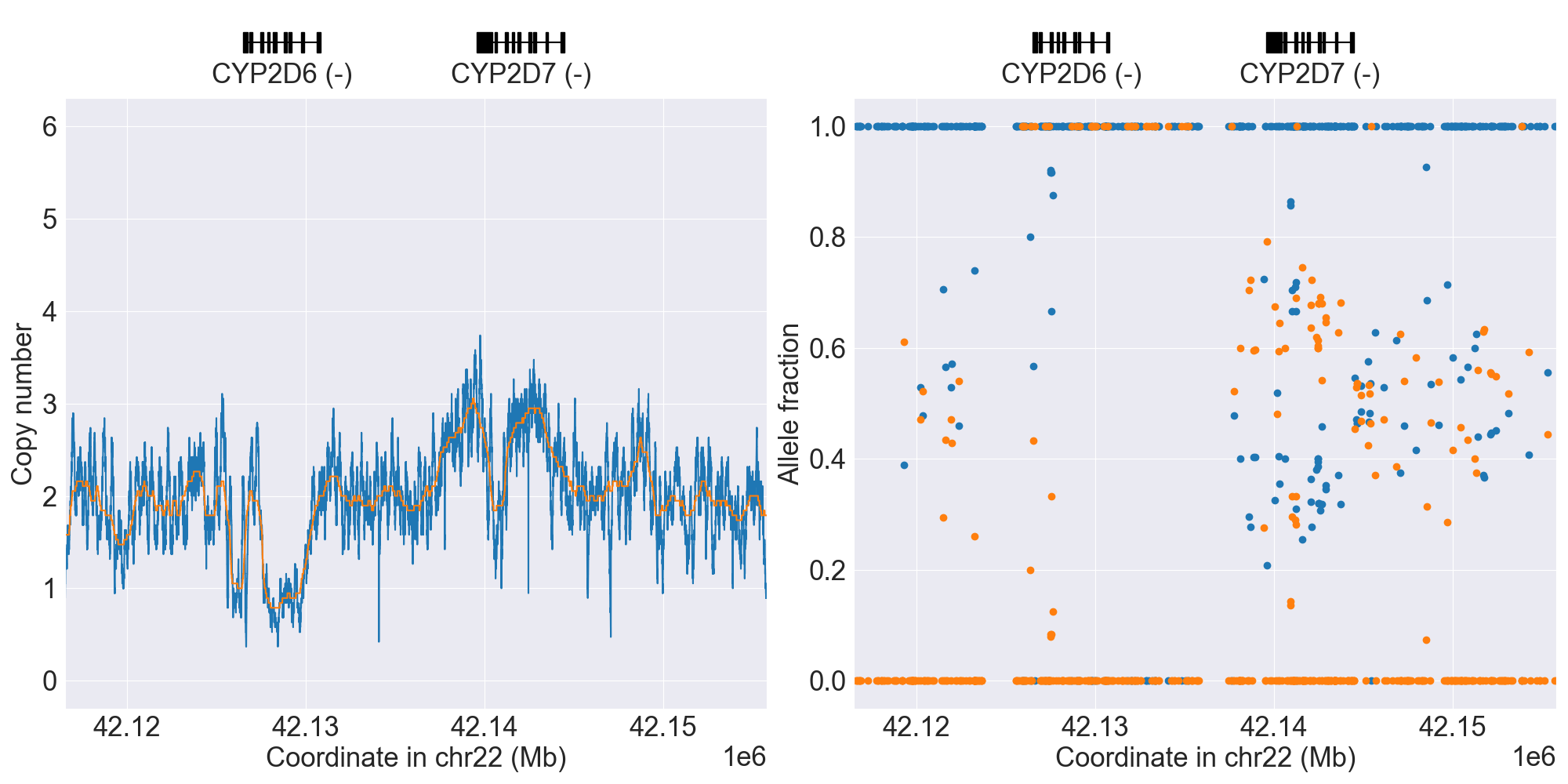
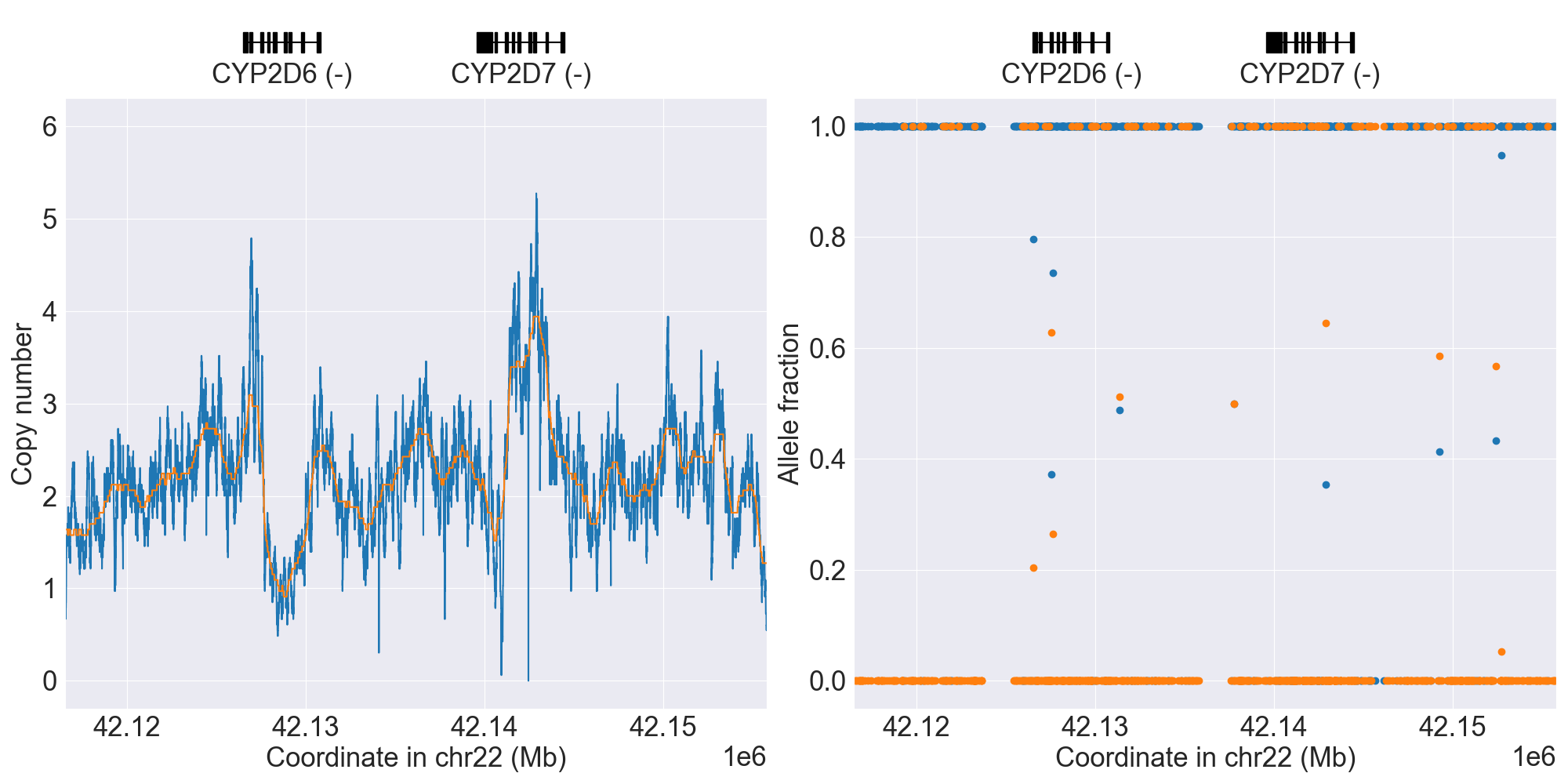
CYP2D6
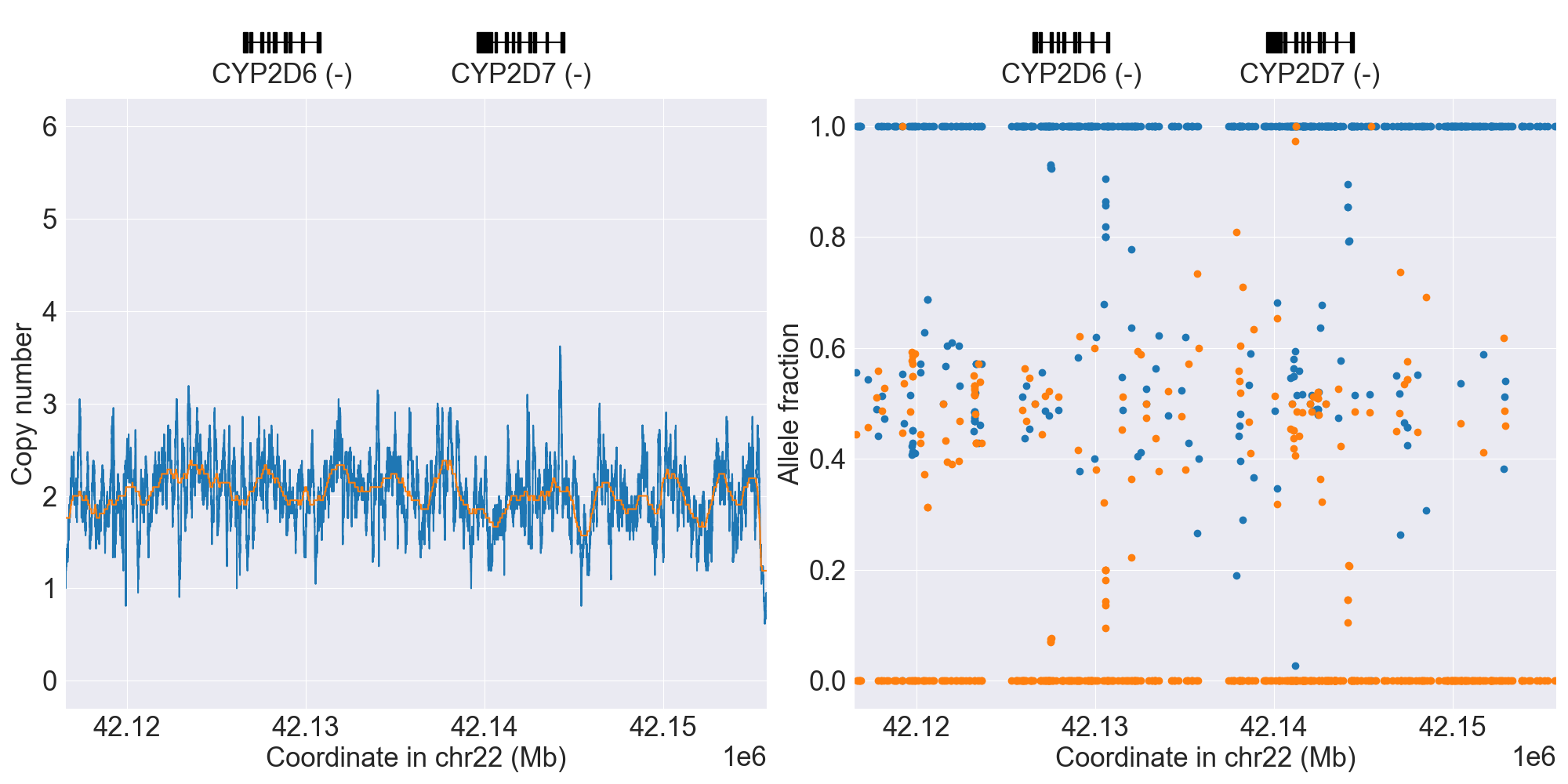
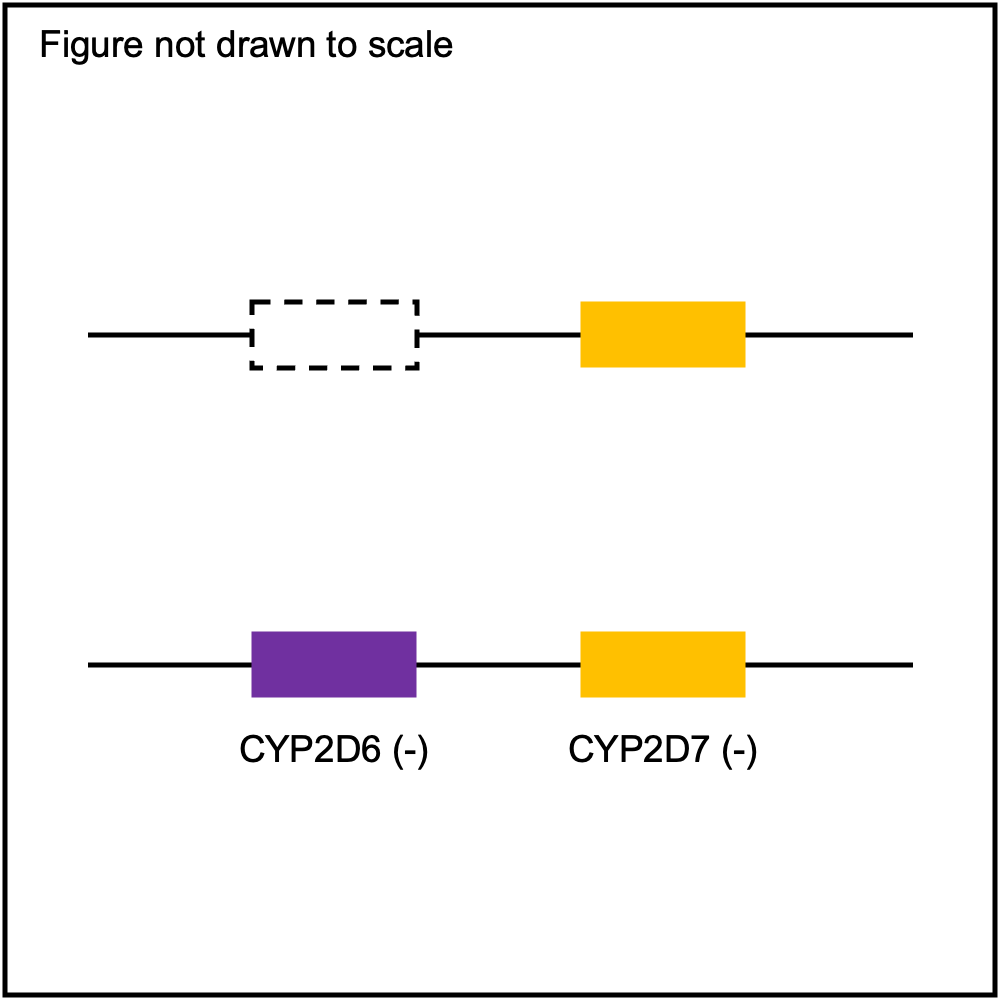
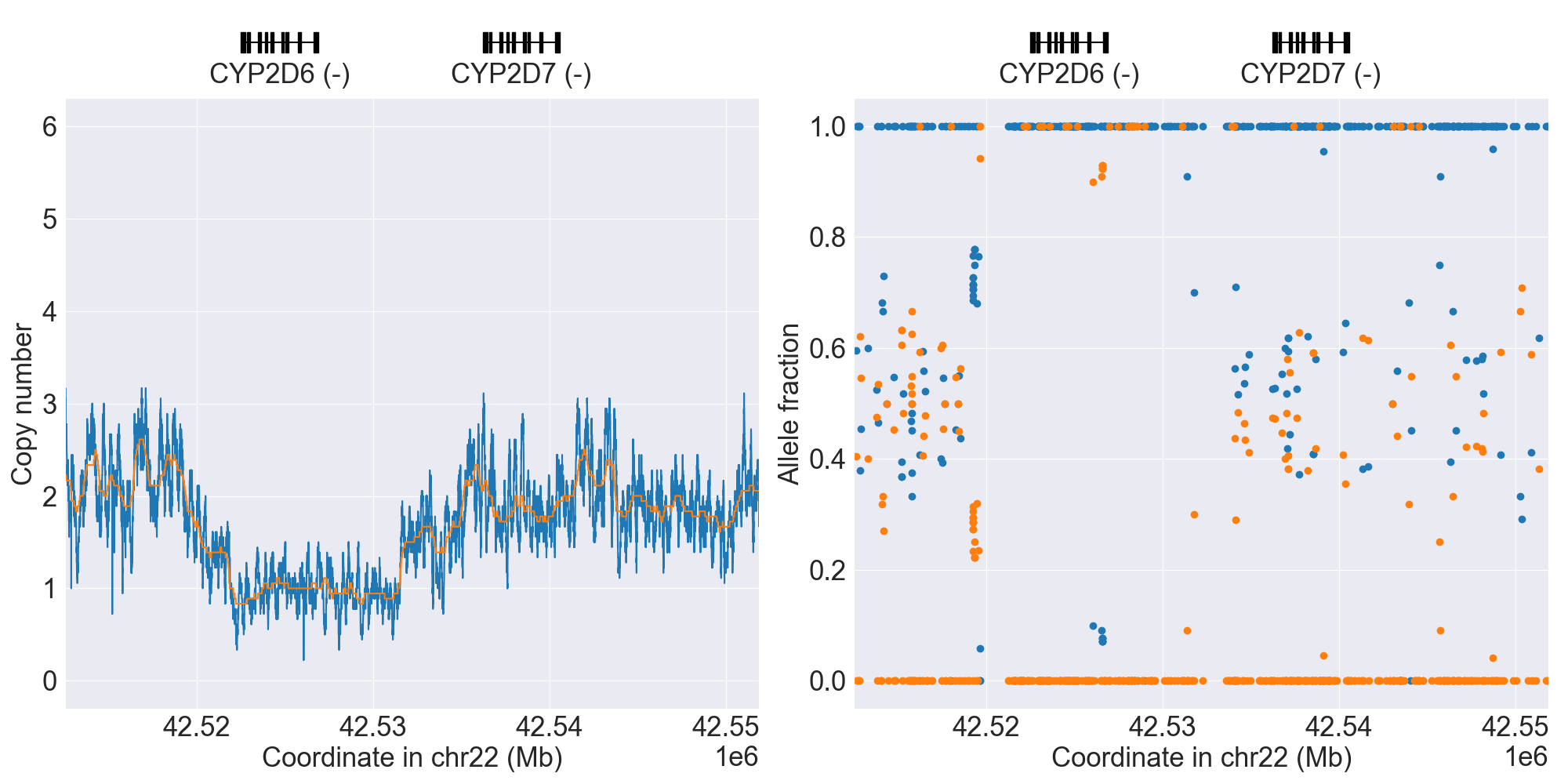
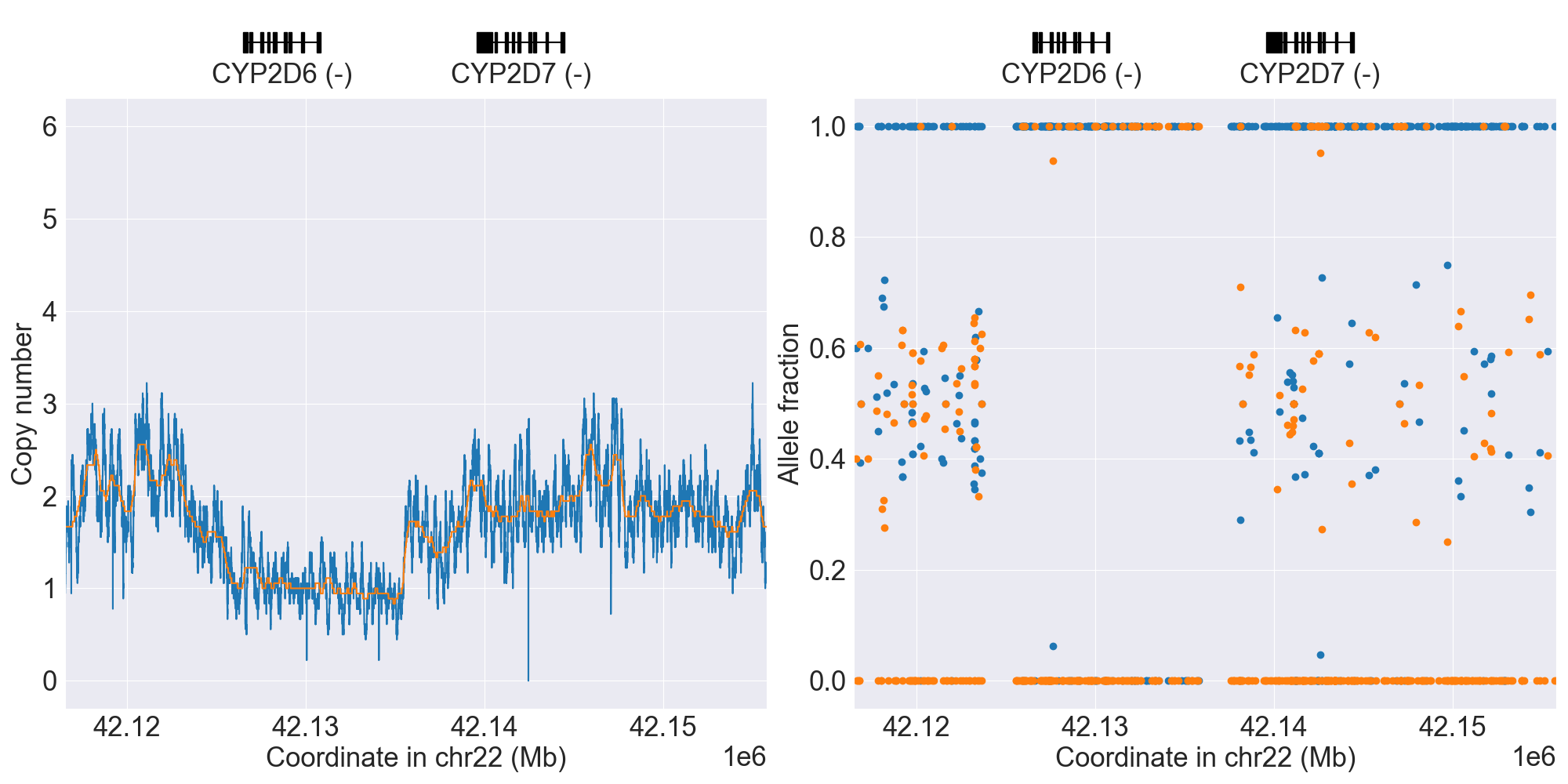
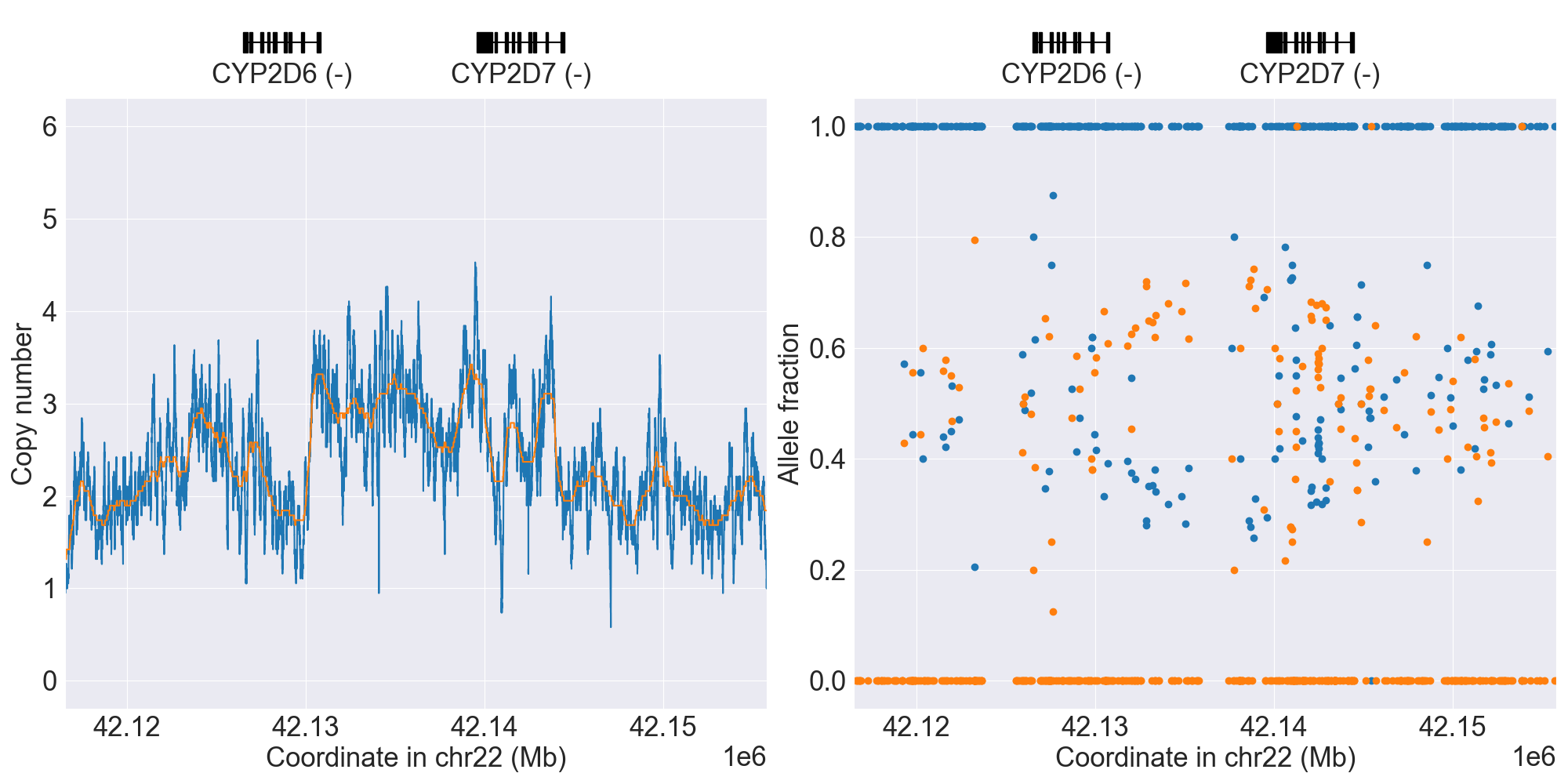
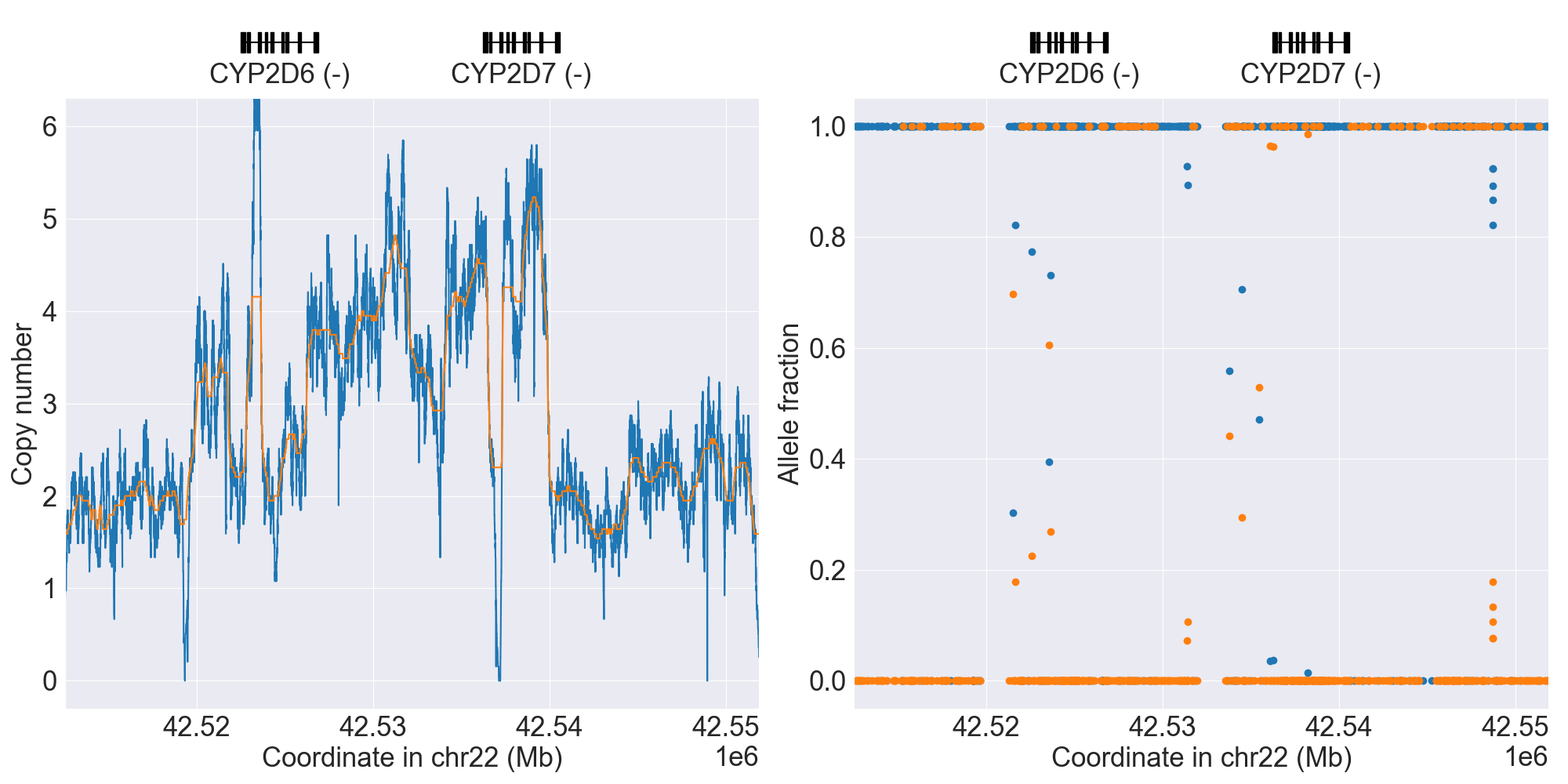
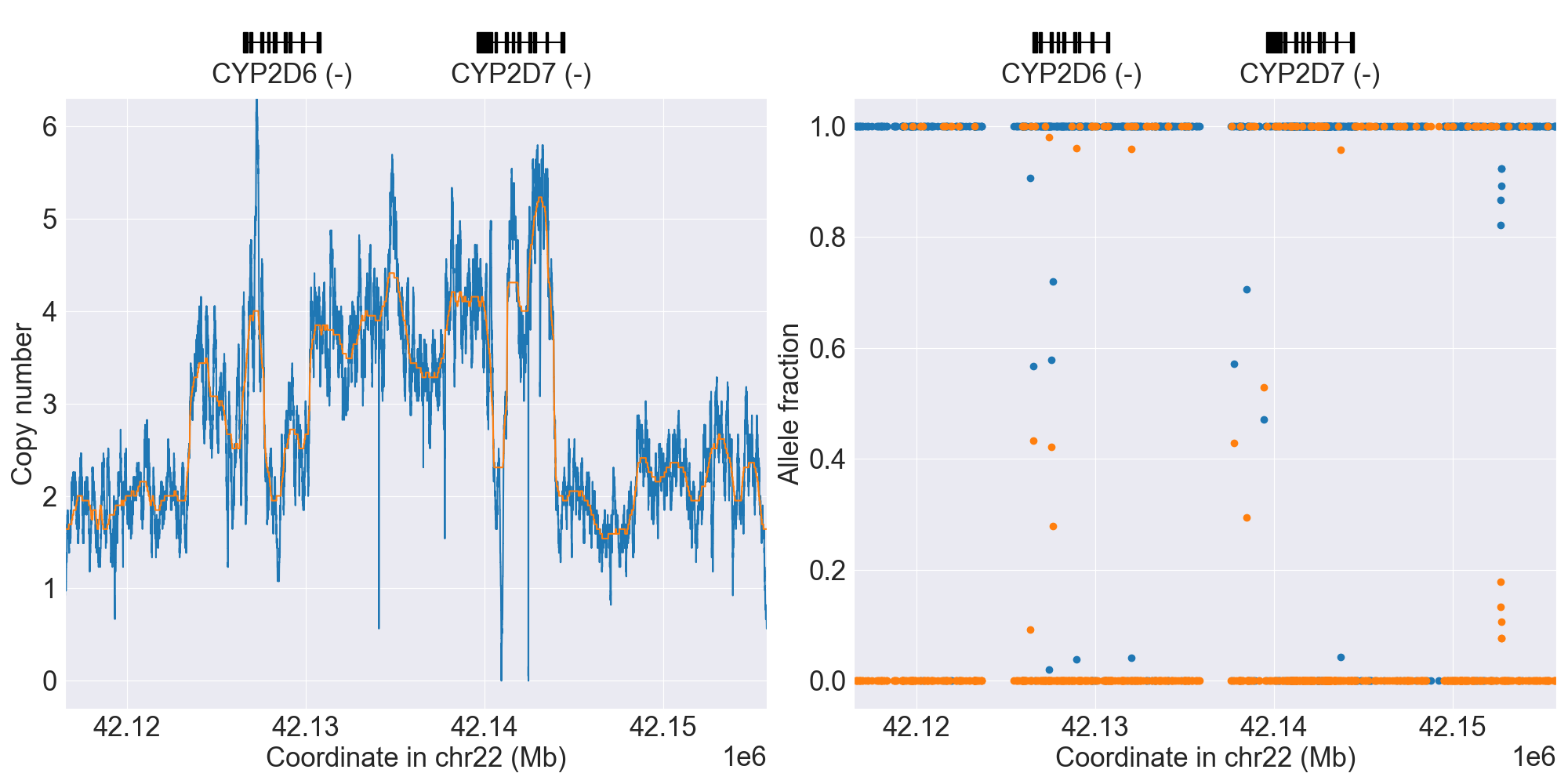
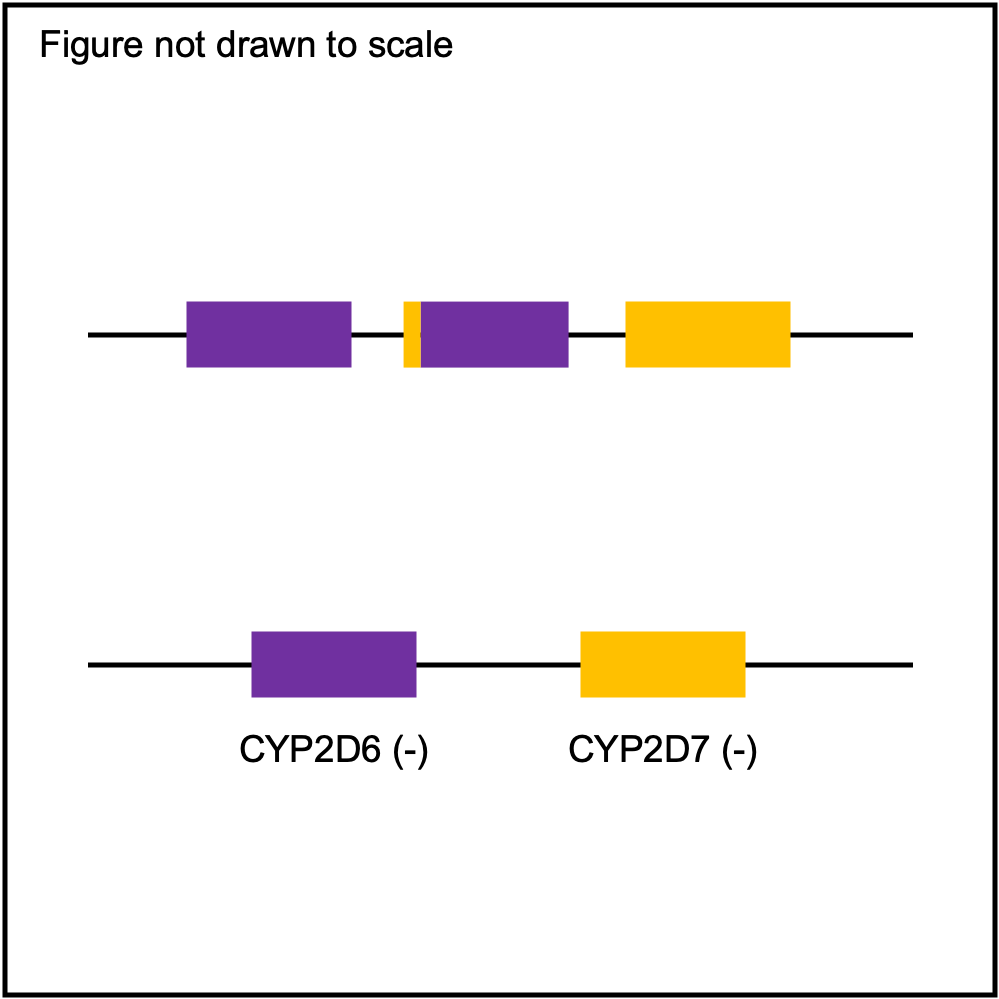
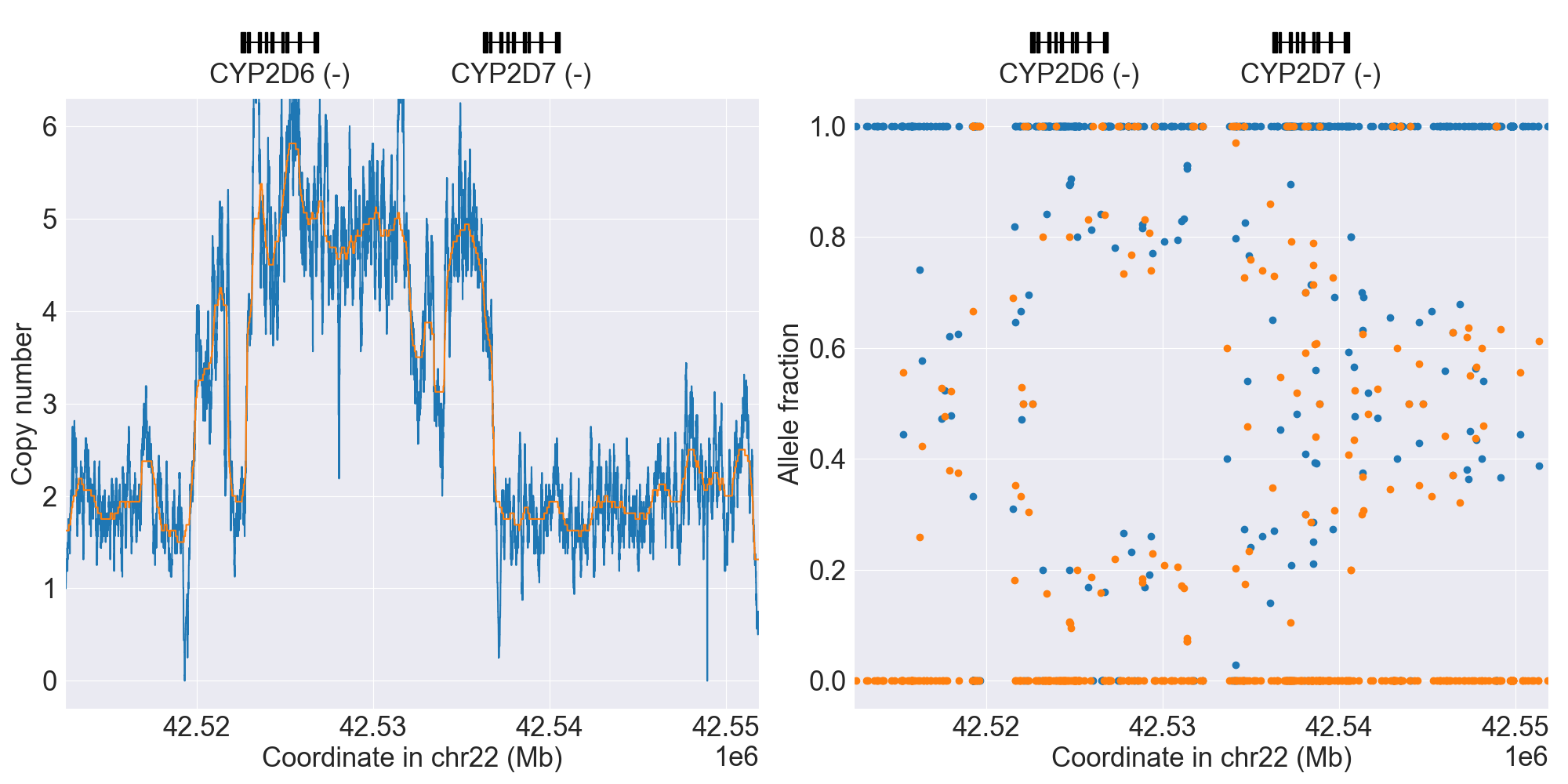
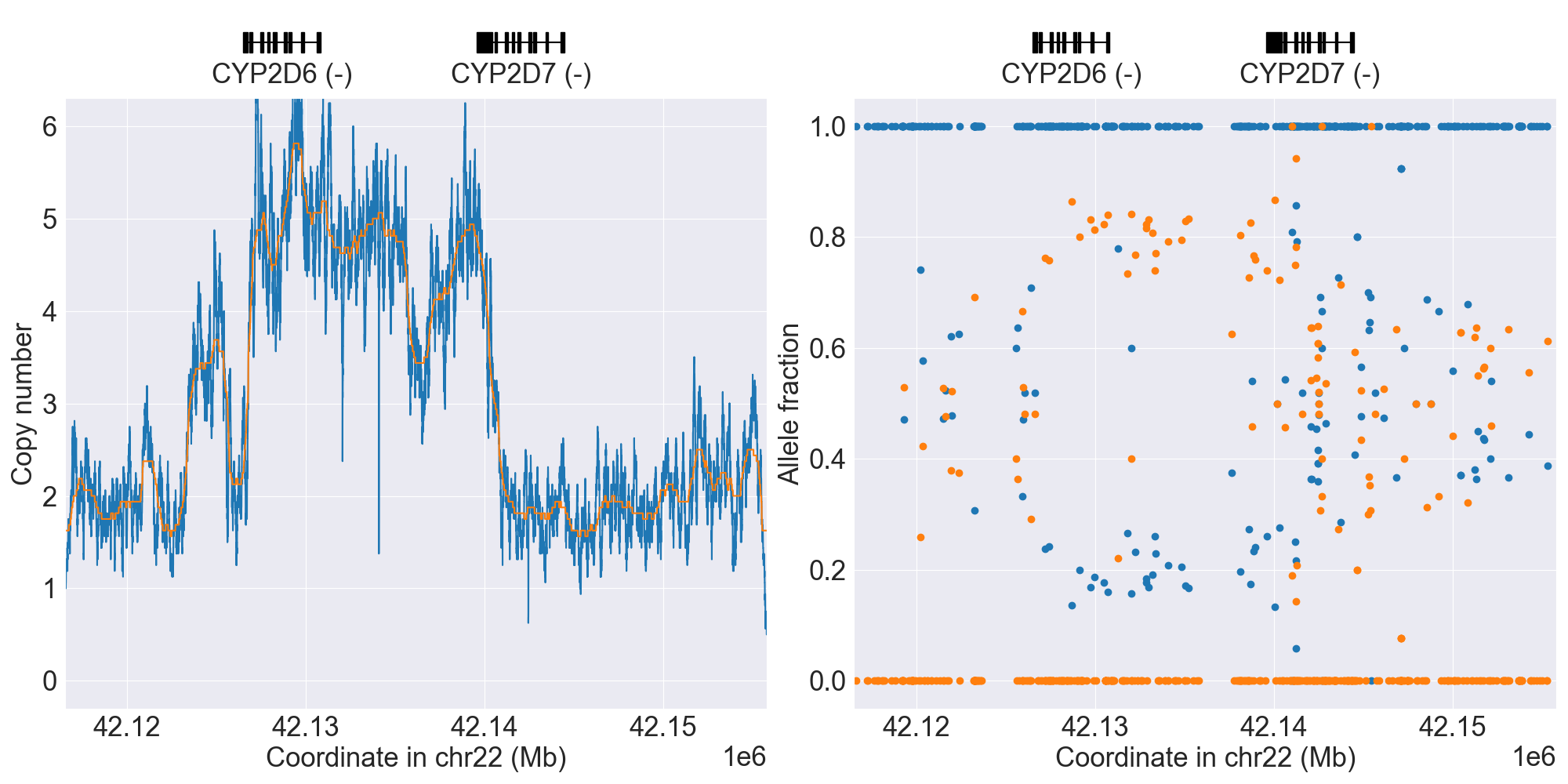
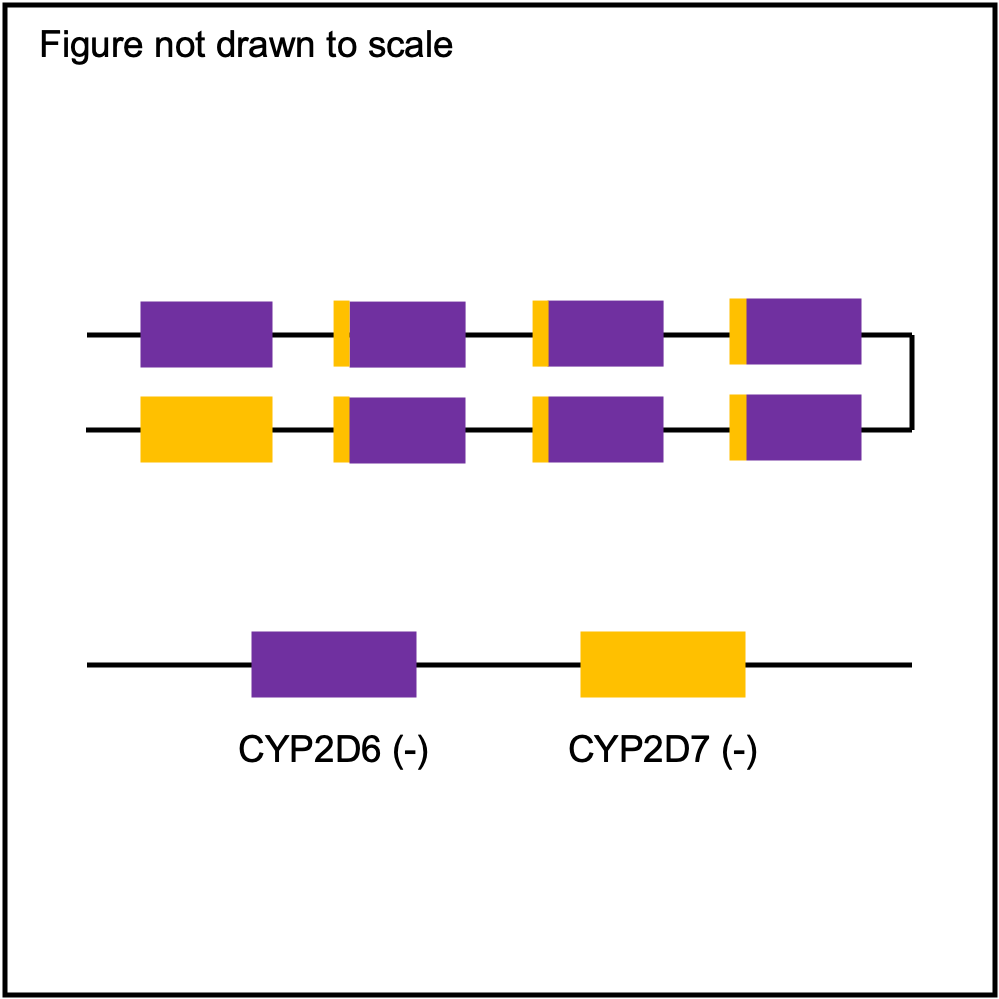
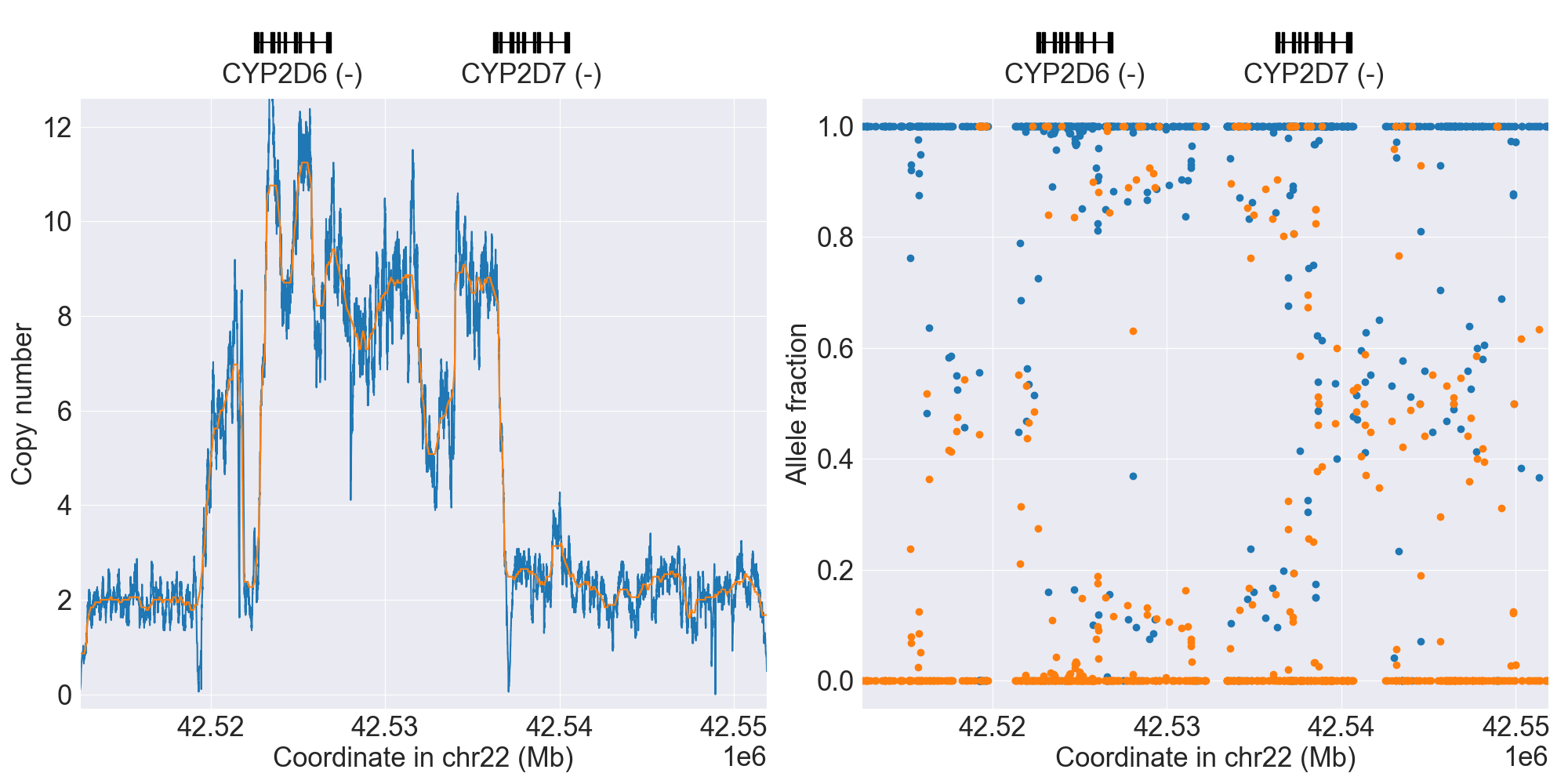
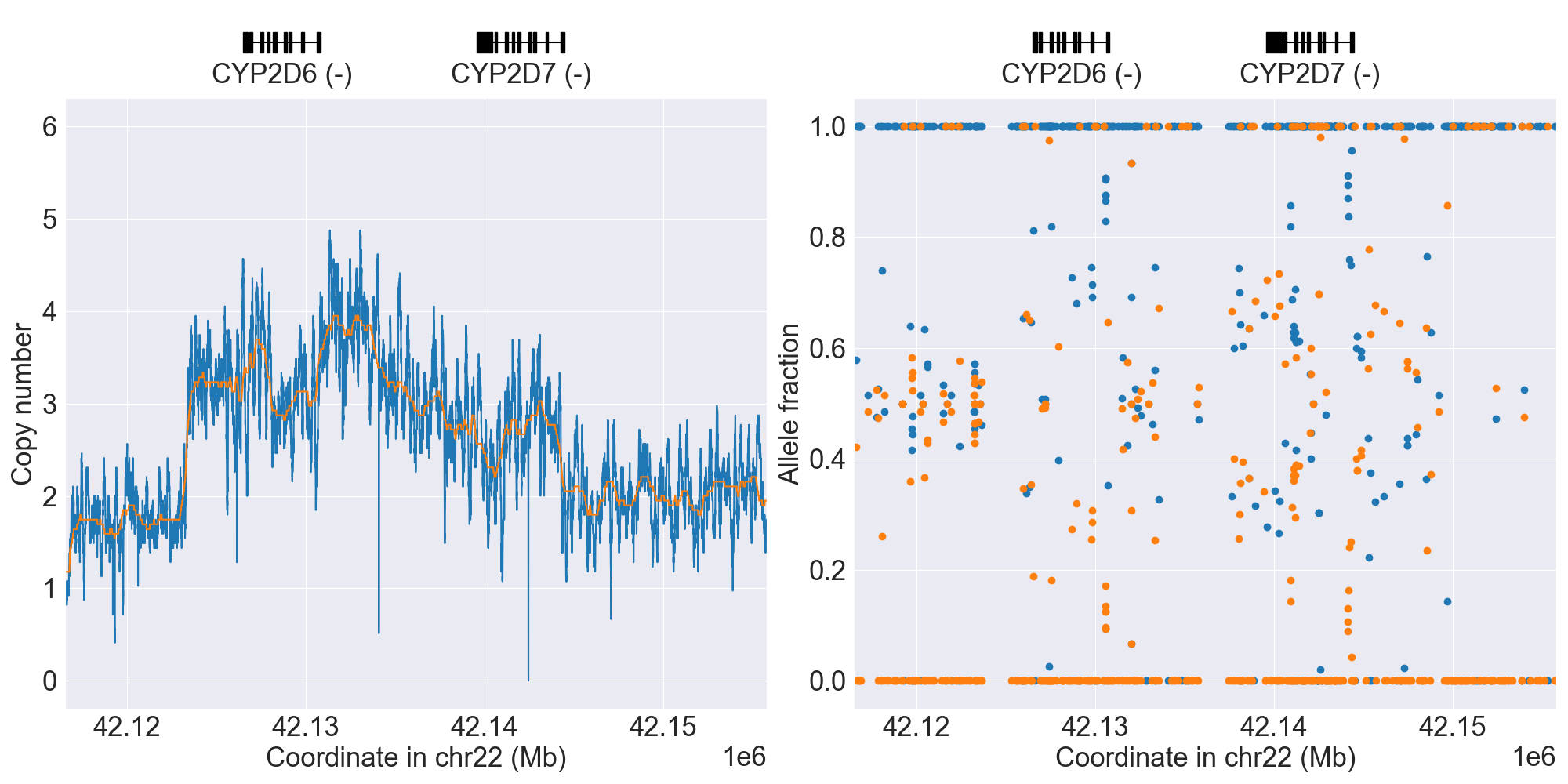
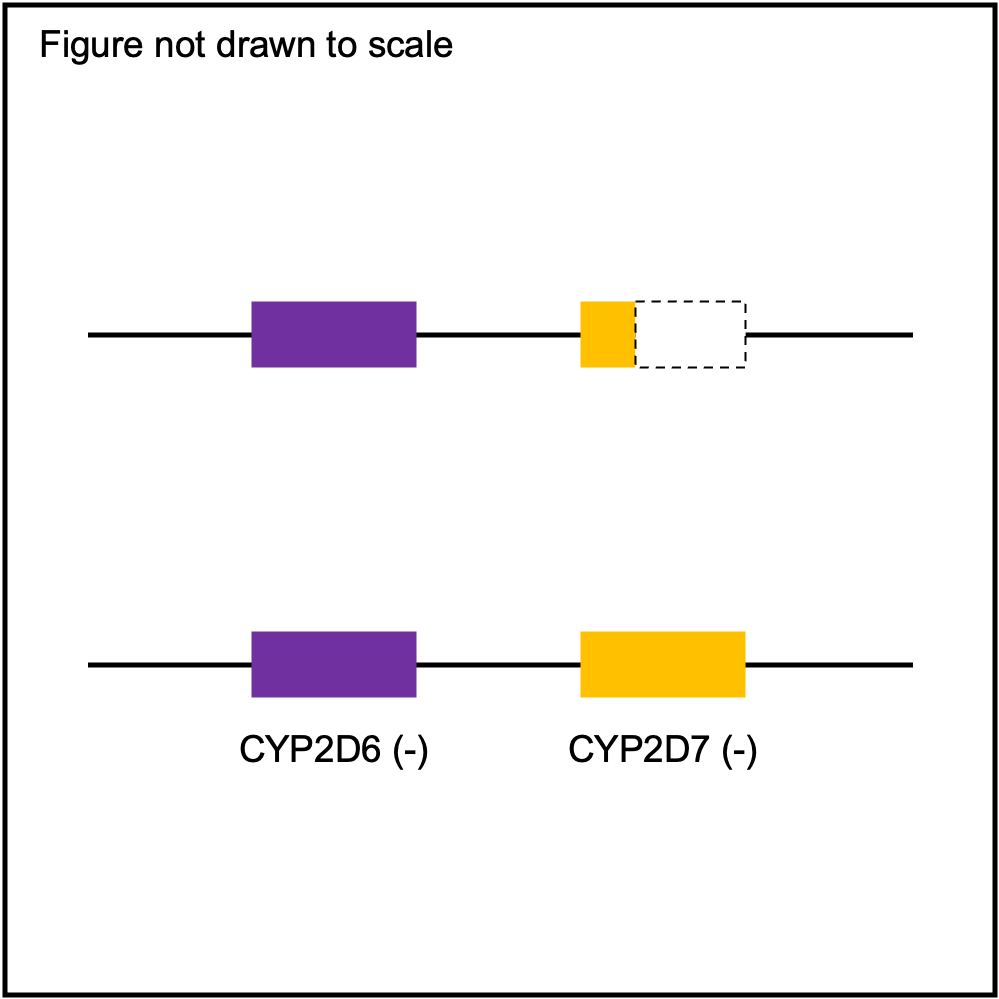
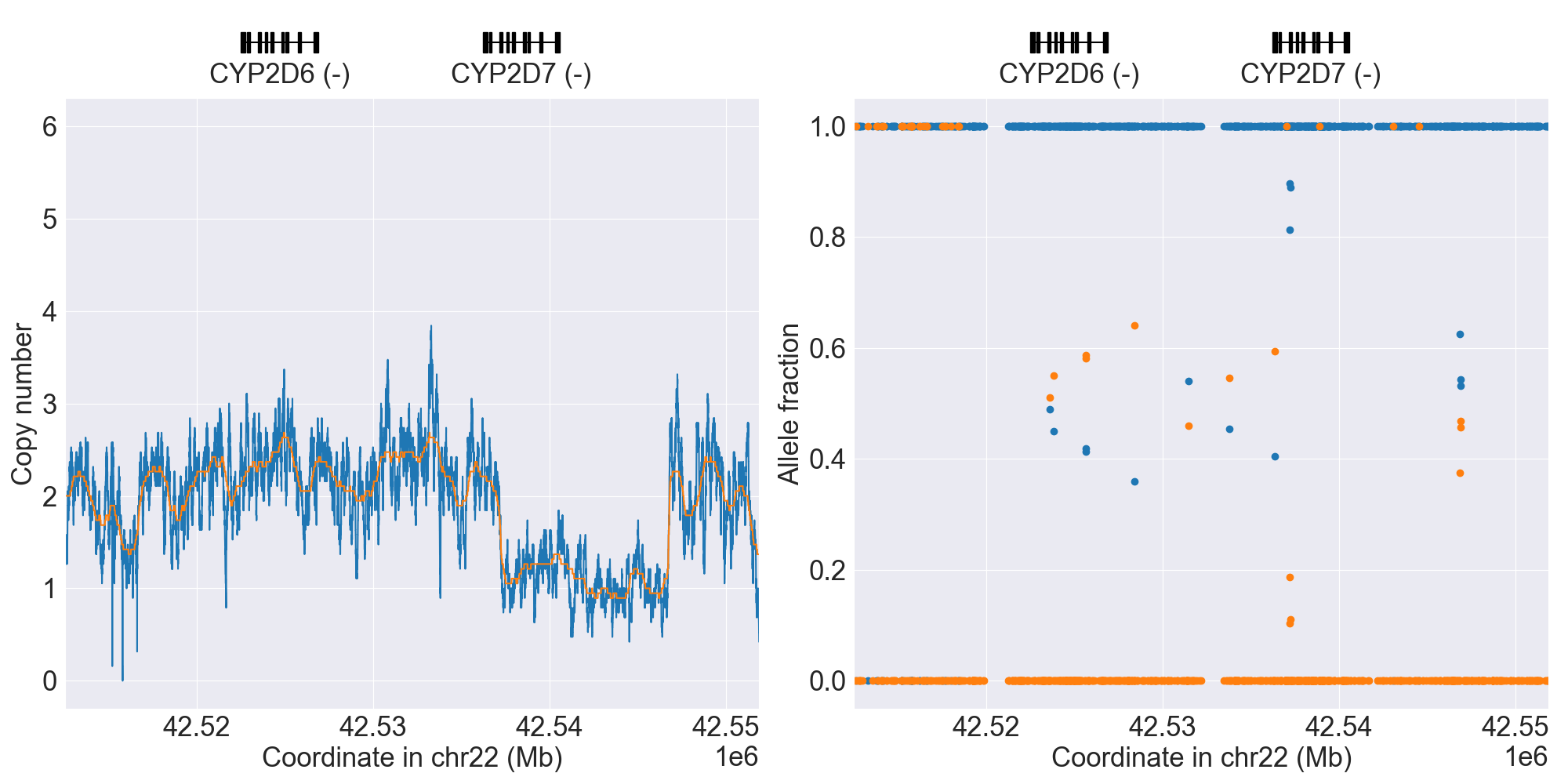
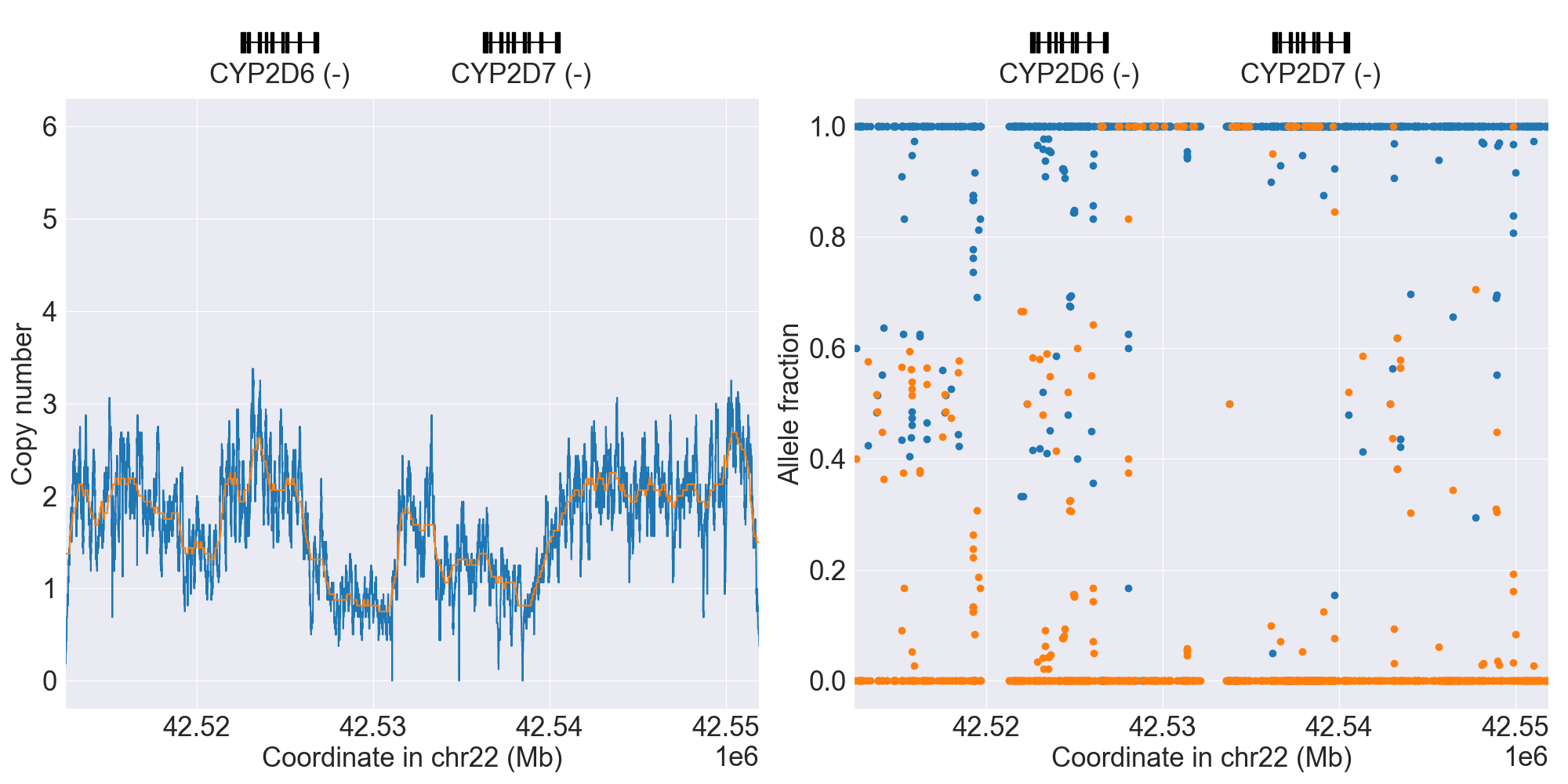
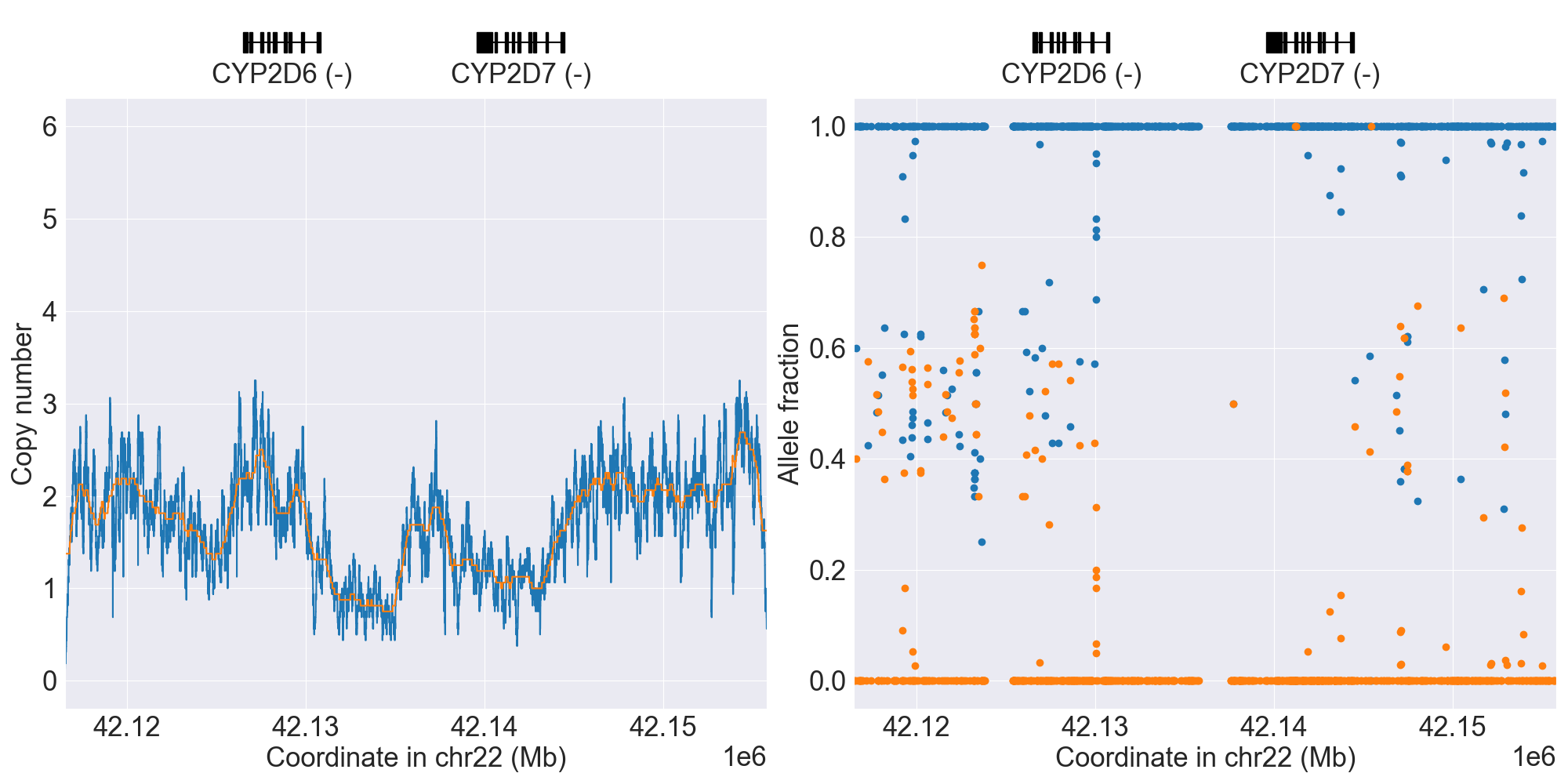
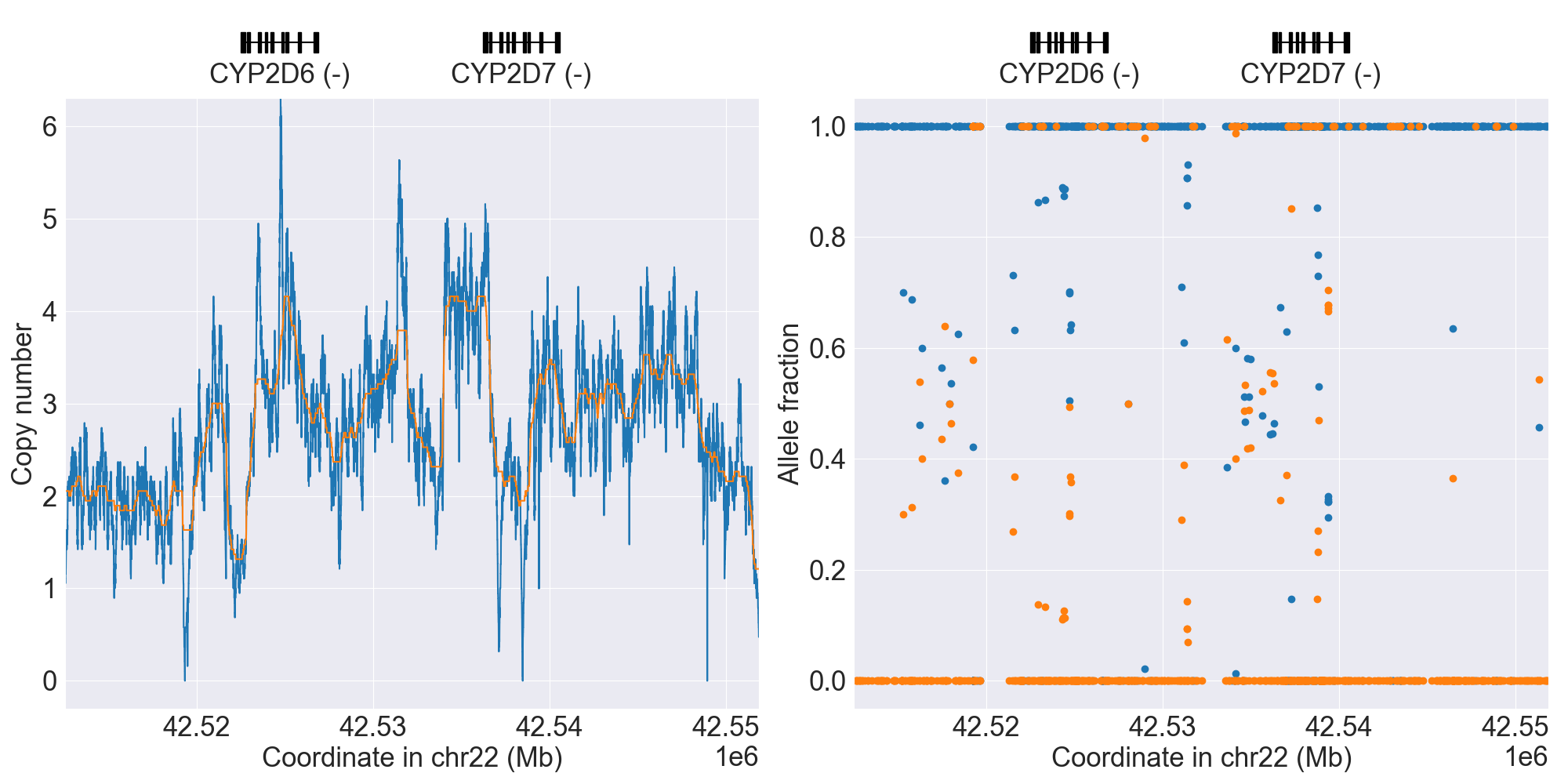
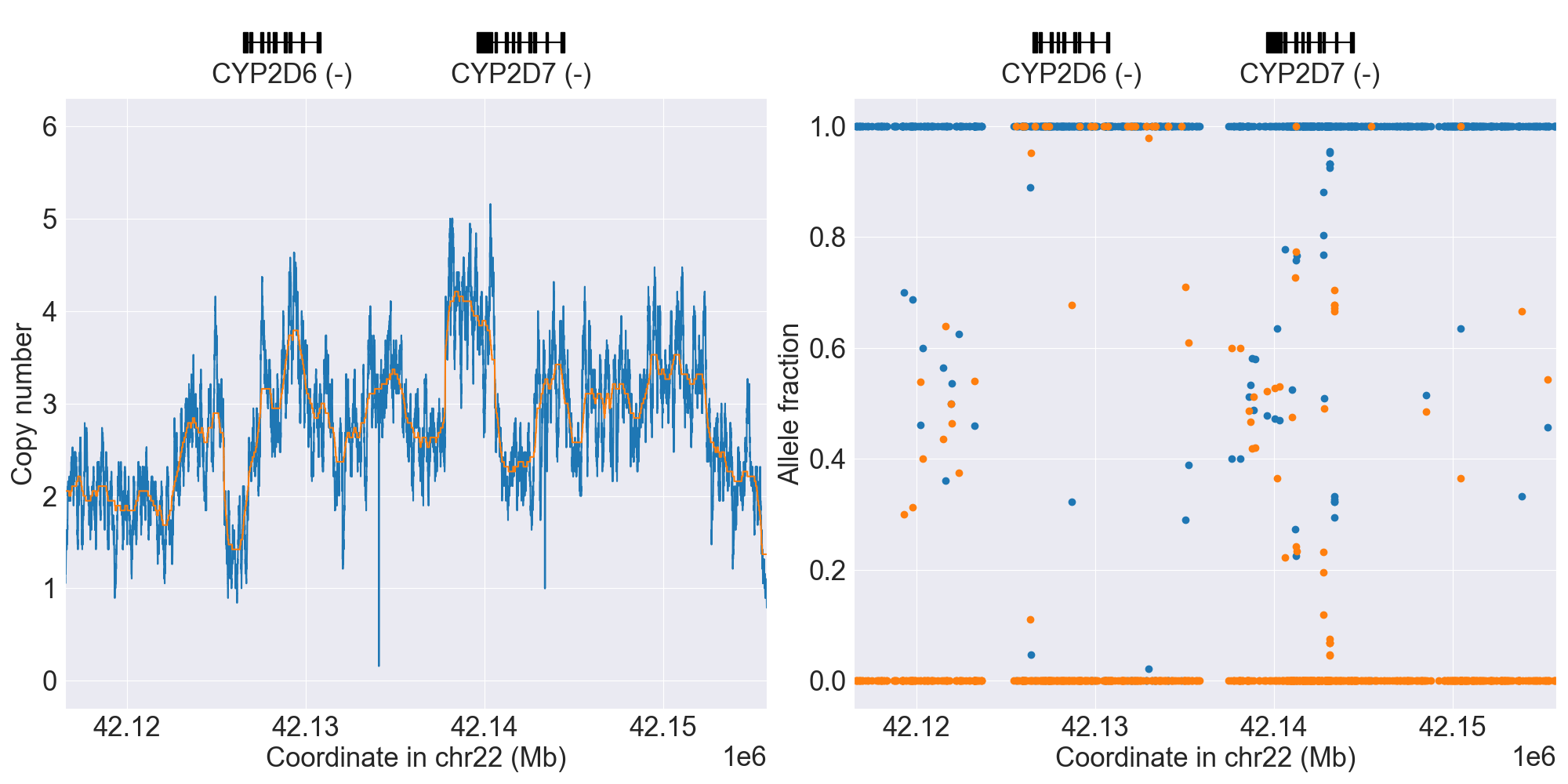
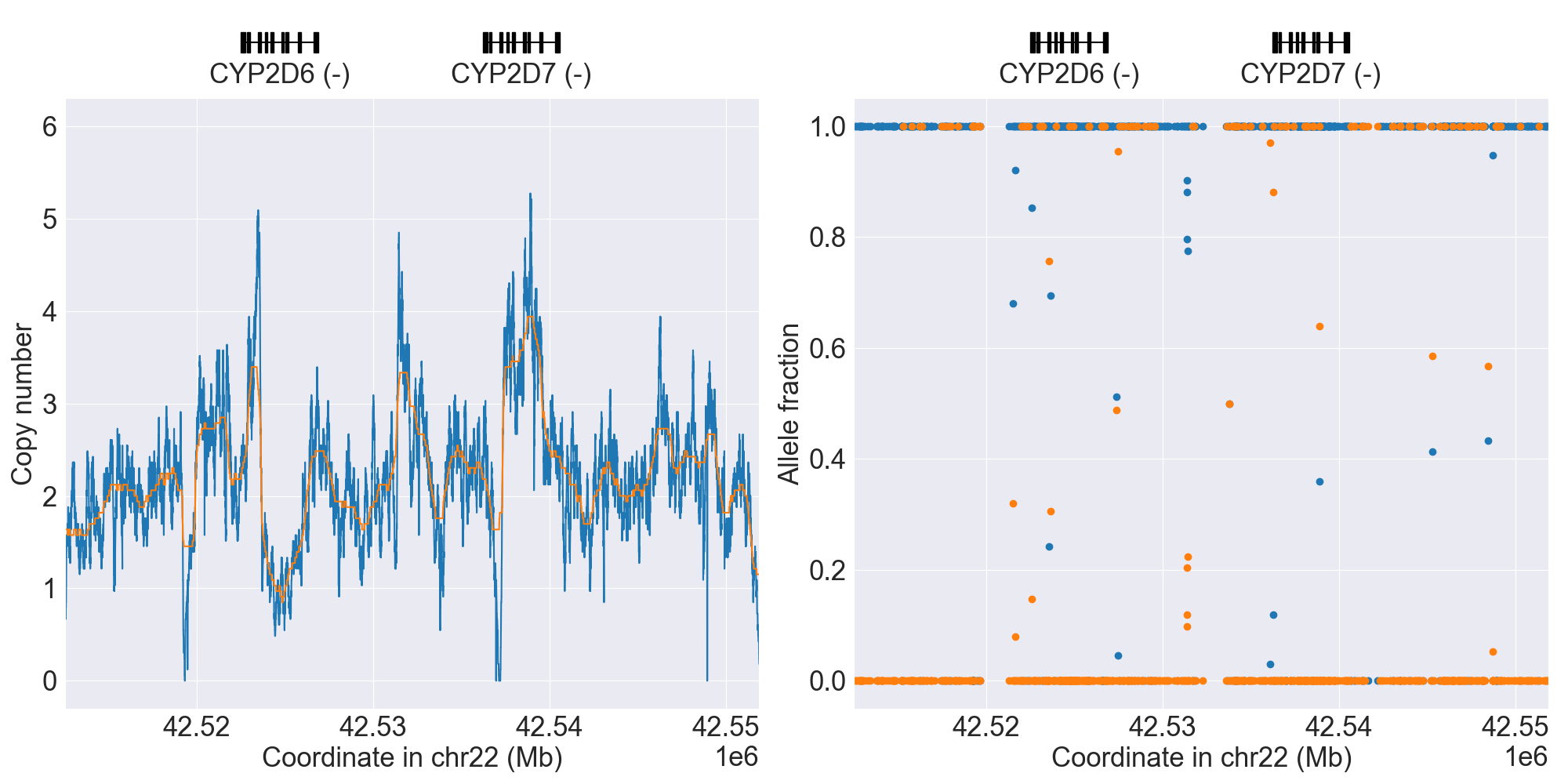
SV summary for CYP2D6
Below is comprehensive summary of SV described from real NGS studies:
SV Alleles |
SV Name |
Genotype |
Reference |
Gene Model |
GRCh37 |
GRCh38 |
Data Type |
Source |
Coriell ID |
Version |
Description |
|---|---|---|---|---|---|---|---|---|---|---|---|
Normal |
*1/*2 |
WGS |
NA11839 |
0.4.1 |
|||||||
*5 |
WholeDel1 |
*5/*29 |
WGS |
NA18861 |
0.4.1 |
||||||
*5 |
WholeDel1Hom |
*5/*5 |
WGS |
0.10.0 |
|||||||
*4x2 |
WholeDup1 |
*2/*4x2 |
WGS |
NA19819 |
0.4.1 |
||||||
*1x3 |
WholeMultip1 |
*1x3/*10 |
WGS |
NA19190 |
0.12.0 |
||||||
*68+*4 |
Tandem1A |
*139/*68+*4 |
WGS |
NA11832 |
0.4.1 |
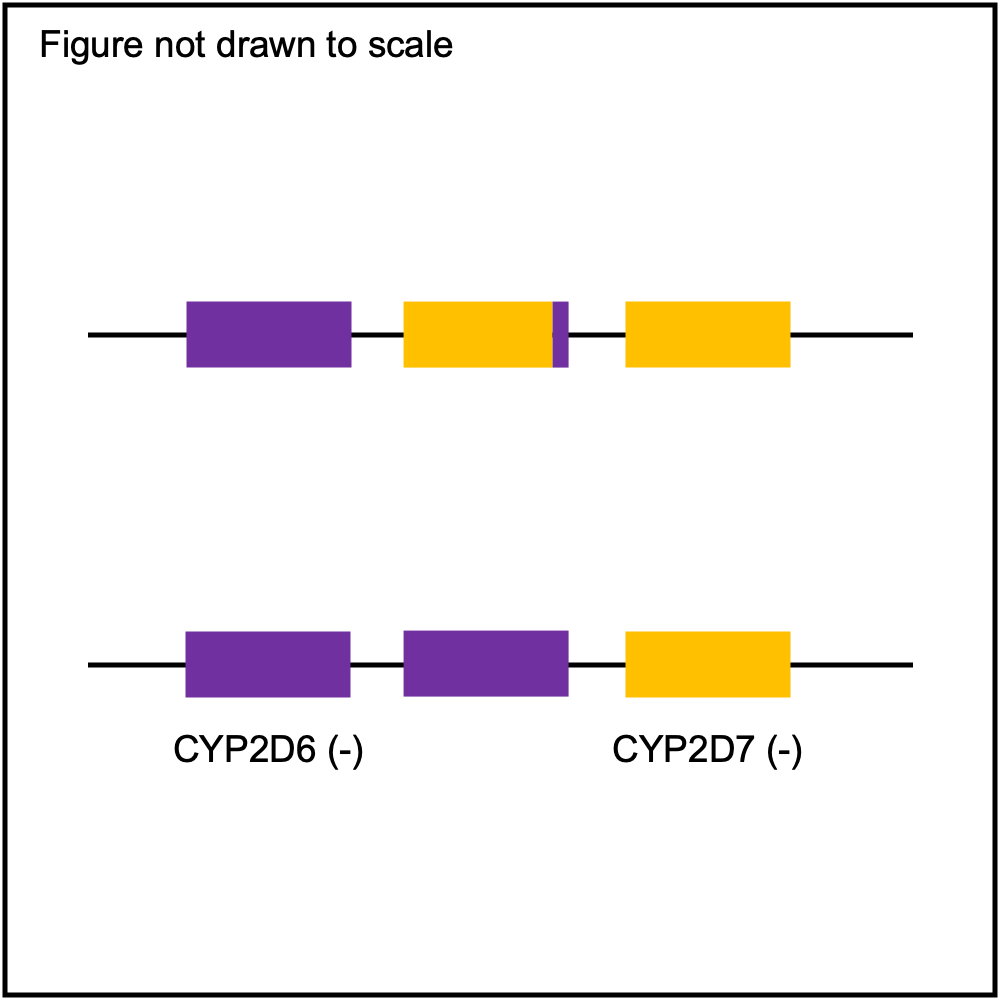
*68 has exon 1 of CYP2D6 origin and exons 2-9 of CYP2D7 origin (breakpoint in intron 1). |
|||||
*68+*4 |
Tandem1B |
*68+*4/*68+*4 |
WGS |
NA12282 |
0.12.0 |
||||||
*36+*10 |
Tandem2A |
*2/*36+*10 |
WGS |
NA18564 |
0.4.1 |
*36 has exons 1-8 of CYP2D6 origin and exon 9 of CYP2D7 origin (breakpoint in exon 9). |
|||||
*36x2+*10 |
Tandem2B |
*1/*36x2+*10 |
WGS |
NA18524 |
0.4.1 |
||||||
*36x3+*10 |
Tandem2C |
*1/*36x3+*10 |
WGS |
0.10.0 |
|||||||
Tandem2F |
Indeterminate |
WGS |
HG00458 |
0.15.0 |
|||||||
*13+*1 |
Tandem3 |
*1/*13+*1 |
WGS |
0.11.0 |
|||||||
Tandem4 |
Indeterminate |
WGS |
NA19719 |
0.14.0 |
|||||||
*5, *68+*4 |
WholeDel1+Tandem1A |
*5/*68+*4 |
WGS |
HG01190 |
0.4.1 |
||||||
*2x2, *68+*4 |
WholeDup1+Tandem1A |
*2x2/*68+*4 |
WGS |
NA21781 |
0.4.1 |
||||||
ParalogPartialDel1 |
*2/*41 |
WGS |
NA19316 |
0.13.0 |
|||||||
WholeDel1+Tandem3 |
Indeterminate |
WGS |
HG03803 |
0.16.0 |
|||||||
Unknown1 |
Indeterminate |
WGS |
NA18555 |
0.12.0 |
|||||||
Unknown2 |
Indeterminate |
WGS |
NA19982 |
0.14.0 |
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
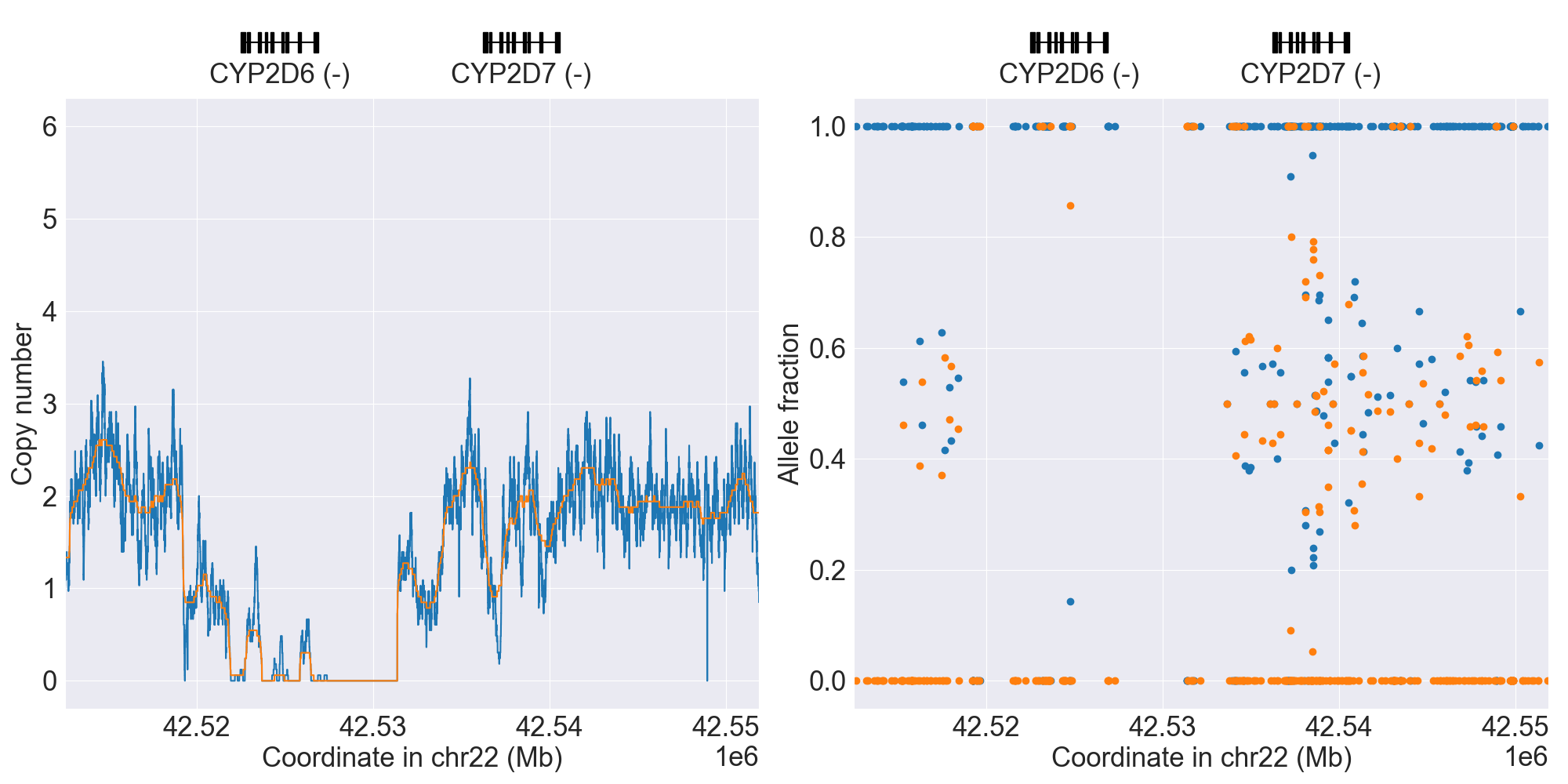
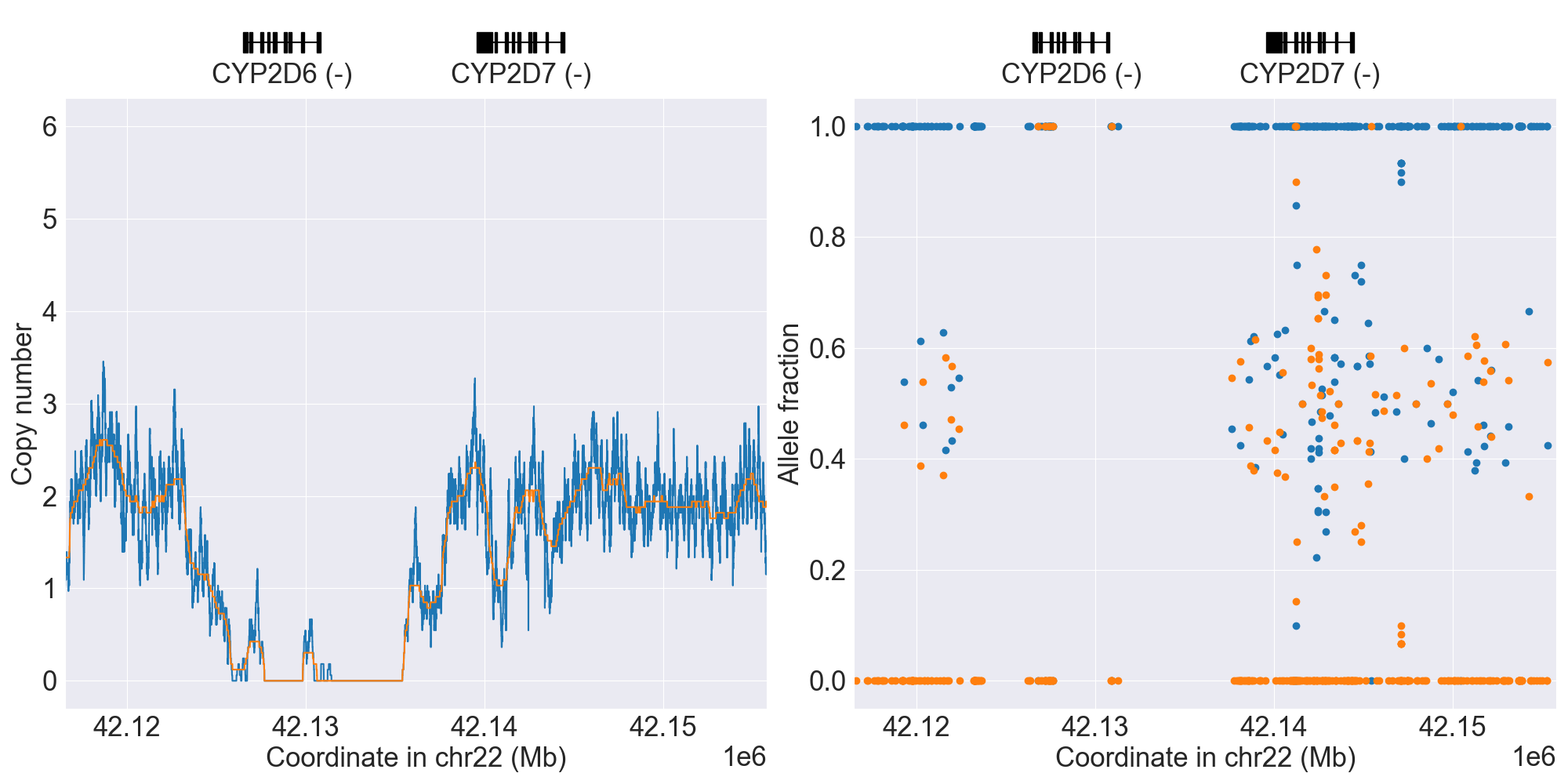
PyPGx was recently applied to the entire high-coverage WGS dataset from 1KGP (N=2,504). Click here to see individual SV calls for CYP2D6, and corresponding copy number profiles and allele fraction profiles.
Phenotype summary for CYP2D6
Activity score is used for phenotype prediction.
Phenotype |
Activity Score |
Example |
Priority |
|---|---|---|---|
Ultrarapid Metabolizer |
2.5 <= score |
*1/*2x2 |
Abnormal/Priority/High Risk |
Normal Metabolizer |
1.25 <= score < 2.5 |
*1/*1 |
Normal/Routine/Low Risk |
Intermediate Metabolizer |
0.25 <= score < 1.25 |
*1/*4 |
Abnormal/Priority/High Risk |
Poor Metabolizer |
0 <= score < 0.25 |
*4/*5 |
Abnormal/Priority/High Risk |
Indeterminate |
Unknown score |
*1/*22 |
None |
Recommendations for CYP2D6
Amitriptyline
“The CPIC Dosing Guideline update for amitriptyline recommends an alternative drug for CYP2D6 ultrarapid or poor metabolizers and CYP2C19 ultrarapid, rapid or poor metabolizers. If amitriptyline is warranted, consider a 50% dose reduction in CYP2D6 or CYP2C19 poor metabolizers. For CYP2D6 intermediate metabolizers, a 25% dose reduction should be considered.” (Source: PharmGKB)
Atomoxetine
“The CPIC Dosing Guideline for atomoxetine provides therapeutic recommendations for CYP2D6 ultrarapid, normal, intermediate, and poor metabolizer, which includes guidance for plasma drug concentration testing, as a means to estimate atomoxetine exposure, if no clinical response and in the absence of adverse events after 2 weeks of therapy.” (Source: PharmGKB)
Clomipramine
“Tricyclic antidepressants have comparable pharmacokinetic properties, it may be reasonable to apply the CPIC Dosing Guideline for amitriptyline and CYP2C19, CYP2D6 to other tricyclics including clomipramine. The CPIC Dosing Guideline update for amitriptyline recommends an alternative drug for CYP2D6 ultrarapid or poor metabolizers and CYP2C19 ultrarapid, rapid or poor metabolizers. If amitriptyline is warranted, consider a 50% dose reduction in CYP2D6 or CYP2C19 poor metabolizers. For CYP2D6 intermediate metabolizers, a 25% dose reduction should be considered.” (Source: PharmGKB)
Codeine
“Alternate non-tramadol analgesics are recommended for CYP2D6 ultrarapid and poor metabolizers. A label recommended age- or weight-specific dose of codeine is warranted for CYP2D6 normal and intermediate metabolizers.” (Source: PharmGKB)
Desipramine
“Tricyclic antidepressants have comparable pharmacokinetic properties, it may be reasonable to apply the CPIC Dosing Guideline for amitriptyline/nortriptyline and CYP2C19, CYP2D6 to other tricyclics including desipramine. The CPIC Dosing Guideline update for nortriptyline recommends a 25% dose reduction for CYP2D6 intermediate metabolizers. For CYP2D6 ultrarapid or poor metabolizers, an alternative drug should be considered. If nortriptyline is warranted, consider a 50% dose reduction in CYP2D6 poor metabolizers.” (Source: PharmGKB)
Doxepin
“Tricyclic antidepressants have comparable pharmacokinetic properties, it may be reasonable to apply the CPIC Dosing Guideline for amitriptyline and CYP2C19, CYP2D6 to other tricyclics including doxepin. The CPIC Dosing Guideline update for amitriptyline recommends an alternative drug for CYP2D6 ultrarapid or poor metabolizers and CYP2C19 ultrarapid, rapid or poor metabolizers. If amitriptyline is warranted, consider a 50% dose reduction in CYP2D6 or CYP2C19 poor metabolizers. For CYP2D6 intermediate metabolizers, a 25% dose reduction should be considered.” (Source: PharmGKB)
Fluvoxamine
“The CPIC Dosing Guideline for the selective serotonin reuptake inhibitor fluvoxamine recommends to consider a 25-50% reduction of recommended starting dose and titrate to response or use an alternative drug not metabolized by CYP2D6 for CYP2D6 poor metabolizers.” (Source: PharmGKB)
Hydrocodone
“CYP2D6 intermediate and poor metabolizers should initiate hydrocodone therapy using the label recommended age- or weight-specific dosing. However, if there is no response to hydrocodone in these patients, an alternative analgesic should be considered.
There is insufficient evidence to provide a dosing recommendation for hydrocodone in CYP2D6 ultrarapid metabolizers.” (Source: PharmGKB)
Imipramine
“Tricyclic antidepressants have comparable pharmacokinetic properties, it may be reasonable to apply the CPIC Dosing Guideline for amitriptyline and CYP2C19, CYP2D6 to other tricyclics including imipramine. The CPIC Dosing Guideline update for amitriptyline recommends an alternative drug for CYP2D6 ultrarapid or poor metabolizers and CYP2C19 ultrarapid, rapid or poor metabolizers. If amitriptyline is warranted, consider a 50% dose reduction in CYP2D6 or CYP2C19 poor metabolizers. For CYP2D6 intermediate metabolizers, a 25% dose reduction should be considered.” (Source: PharmGKB)
Nortriptyline
“The CPIC Dosing Guideline update for nortriptyline recommends a 25% dose reduction for CYP2D6 intermediate metabolizers. For CYP2D6 ultrarapid or poor metabolizers, an alternative drug should be considered. If nortriptyline is warranted, consider a 50% dose reduction in CYP2D6 poor metabolizers.” (Source: PharmGKB)
Ondansetron
“The CPIC dosing guideline for ondansetron recommends selecting an alternate drug for CYP2D6 ultrarapid metabolizers. It is recommended that the alternate drug not be predominantly metabolized by CYP2D6 (eg. granisetron).” (Source: PharmGKB)
Paroxetine
“The CPIC Dosing Guideline for the selective serotonin reuptake inhibitor paroxetine recommends an alternative drug not predominantly metabolized by CYP2D6 for CYP2D6 ultrarapid metabolizers and for CYP2D6 poor metabolizers. For CYP2D6 poor metabolizers, if paroxetine use is warranted, consider a 50% reduction of recommended starting dose and titrate to response.” (Source: PharmGKB)
Tamoxifen
“The CPIC Dosing Guideline for tamoxifen recommends the use of alternative hormonal therapy such as an aromatase inhibitor for postmenopausal women or aromatase inhibitor along with ovarian function suppression in premenopausal women for CYP2D6 poor metabolizer, if aromatase inhibitor use is not contraindicated. For CYP2D6 intermediate metabolizers and CYP2D6 allele combinations resulting in an activity score (AS) of 1 the recommendation is to consider the recommendations stated for the CYP2D6 poor metabolizer. If aromatase inhibitor use is contraindicated, consideration should be given to use a higher but FDA approved tamoxifen dose for CYP2D6 intermediate metabolizers and CYP2D6 allele combinations resulting in an AS of 1. For poor metabolizer, higher dose tamoxifen (40 mg/day) increases but does not normalize endoxifen concentrations and can be considered if there are contraindications to aromatase inhibitor therapy.” (Source: PharmGKB)
Tramadol
“Alternate non-codeine analgesics are recommended for CYP2D6 ultrarapid and poor metabolizers. A label recommended age- or weight-specific dose of tramadol is warranted for CYP2D6 normal and intermediate metabolizers.” (Source: PharmGKB)
Trimipramine
“Tricyclic antidepressants have comparable pharmacokinetic properties, it may be reasonable to apply the CPIC Dosing Guideline for amitriptyline and CYP2C19, CYP2D6 to other tricyclics including trimipramine. The CPIC Dosing Guideline update for amitriptyline recommends an alternative drug for CYP2D6 ultrarapid or poor metabolizers and CYP2C19 ultrarapid, rapid or poor metabolizers. If amitriptyline is warranted, consider a 50% dose reduction in CYP2D6 or CYP2C19 poor metabolizers. For CYP2D6 intermediate metabolizers, a 25% dose reduction should be considered.” (Source: PharmGKB)
Tropisetron
“The CPIC dosing guideline for tropisetron recommends selecting an alternate drug for CYP2D6 ultrarapid metabolizers. It is recommended that the alternate drug not be predominantly metabolized by CYP2D6 (eg. granisetron).” (Source: PharmGKB)
Filtered alleles for CYP2D6
Some alleles in PharmVar will not be called by PyPGx because one or more of their variants have a high false positive rate, likely due to read misalignment to the CYP2D7 pseudogene. Those alleles are listed in below table. If problematic variants are present in gnomAD, their links are provided so that you can look at filtering status, allele imbalance for heterozygotes, etc.
Problematic Variant |
Star Alleles |
GRCh37 |
GRCh38 |
|---|---|---|---|
rs769157652 (E410K) |
*27, *32 |
||
rs61745683 (V370I) |
*122 |
||
rs1058172 (R365H) |
*139 |
||
rs202102799 (Y355C) |
*127 |
||
rs17002853 (L231P) |
*131 |
Resources for CYP2D6
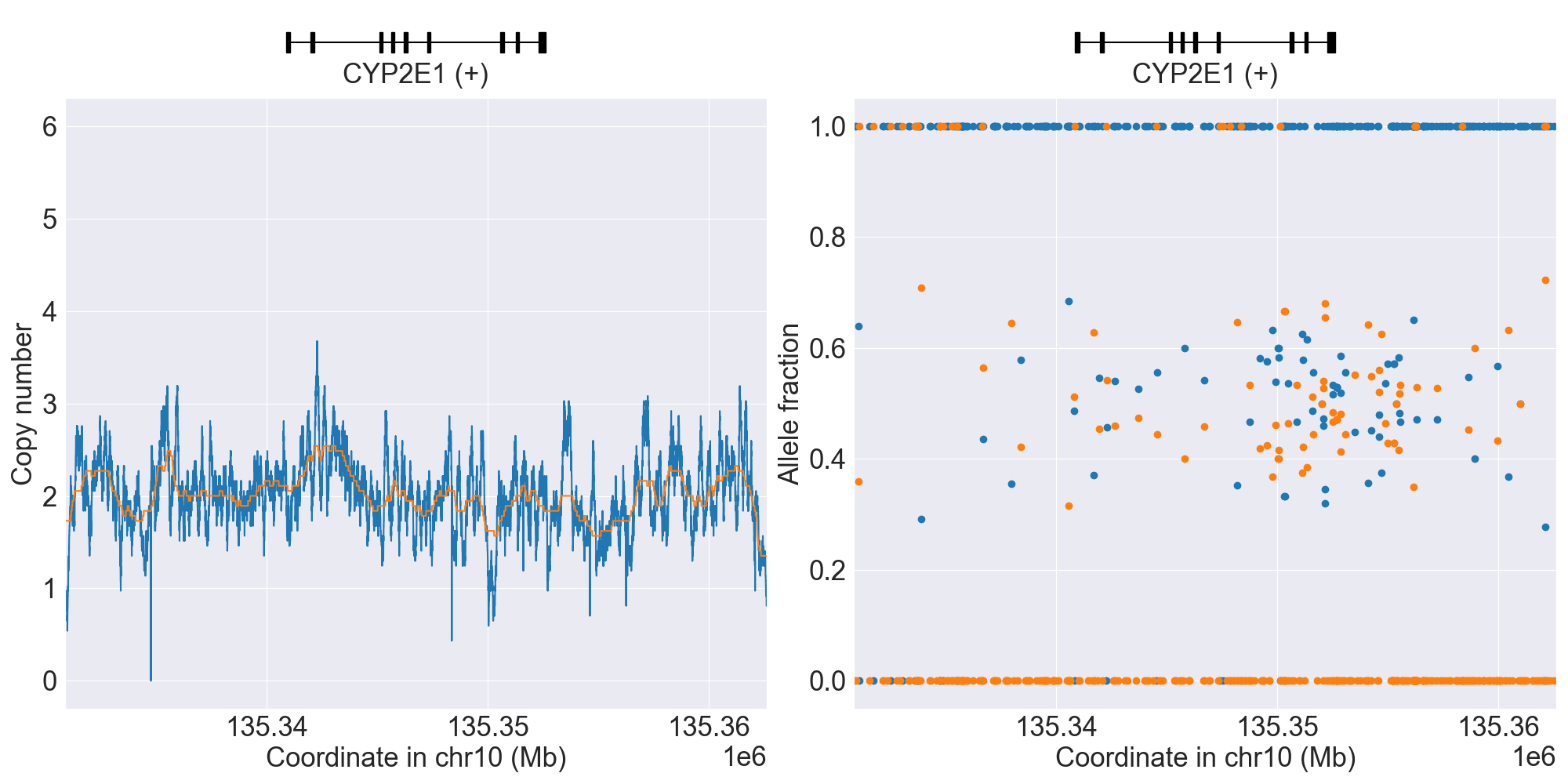
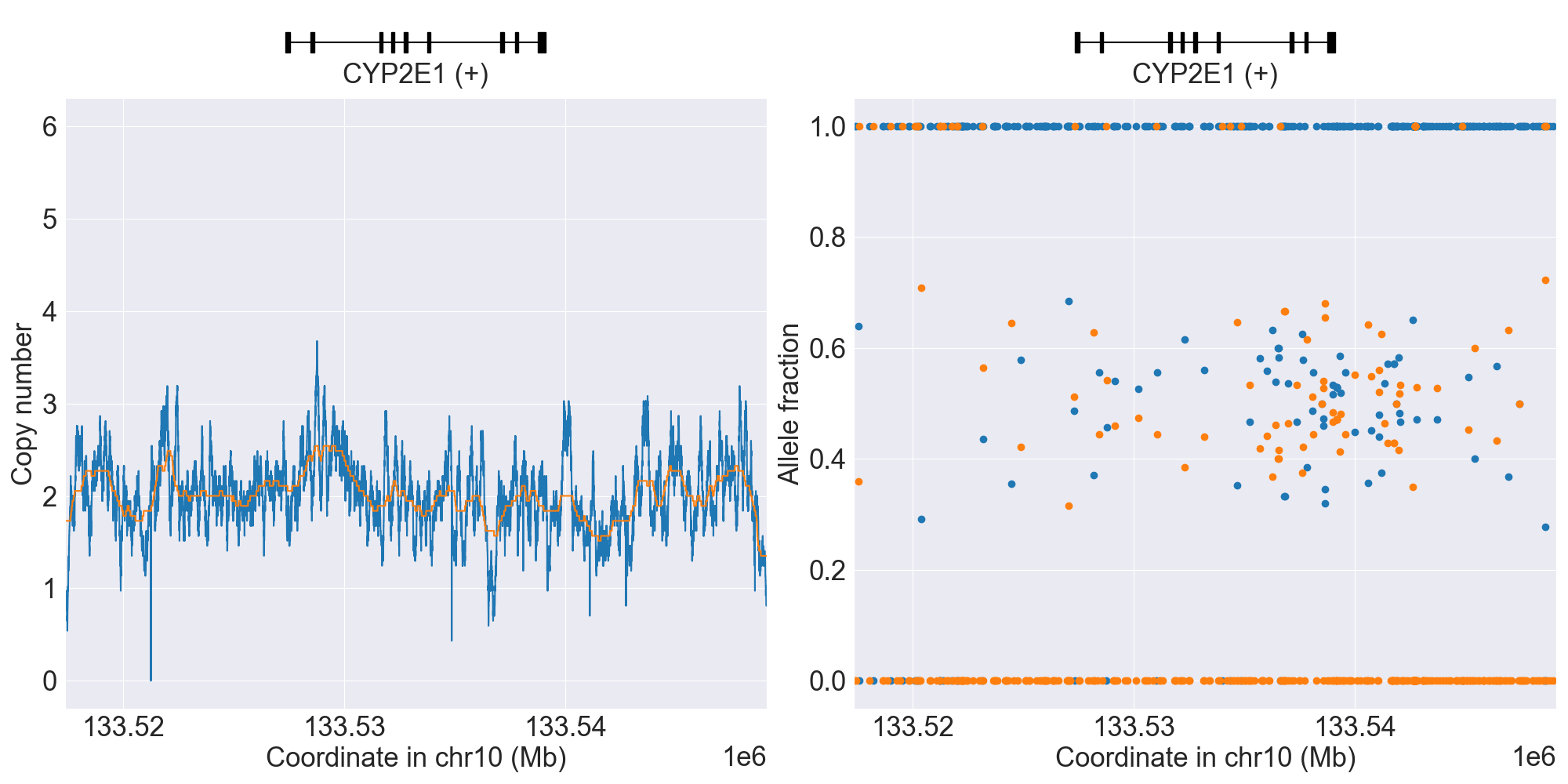
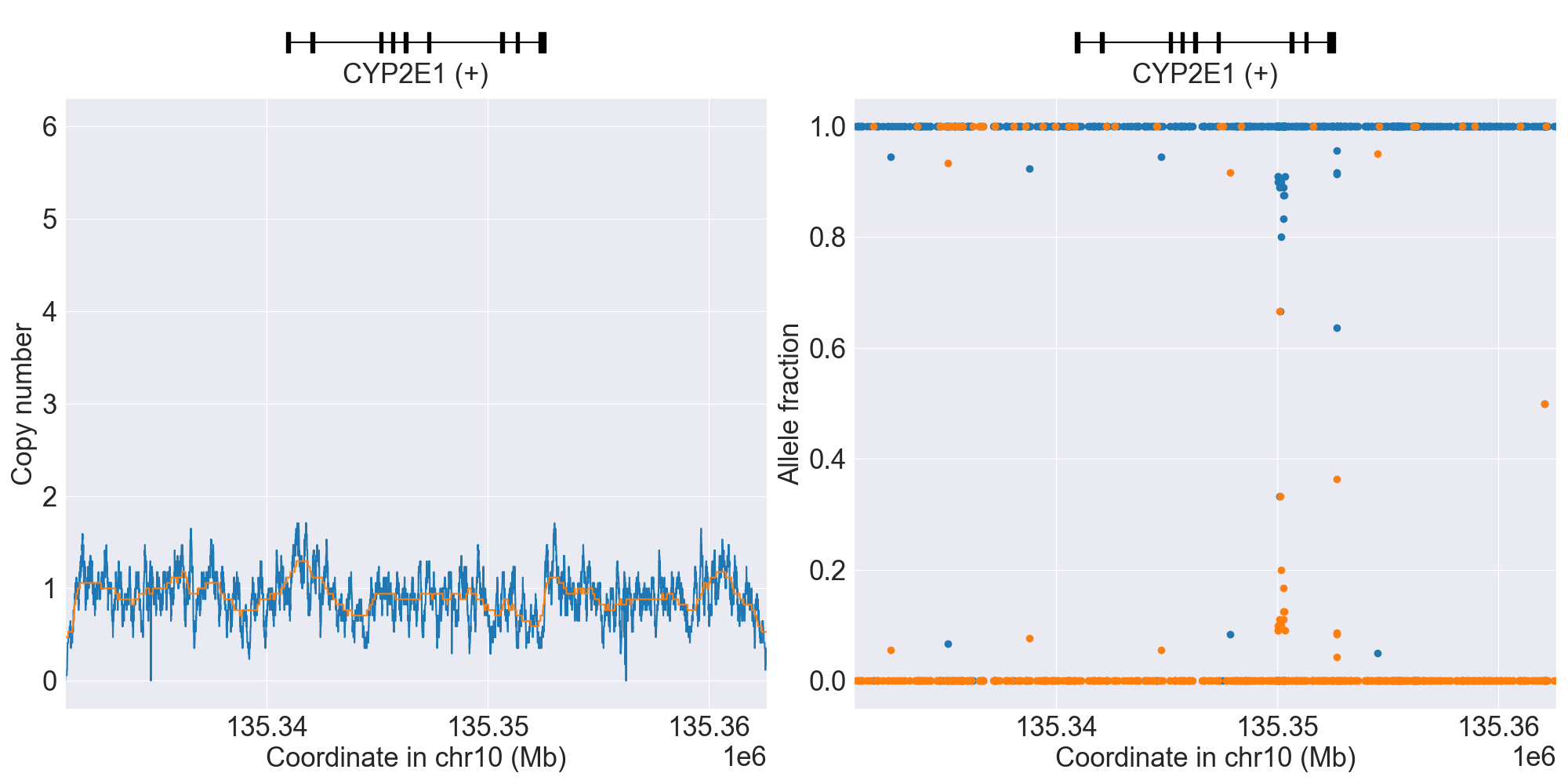
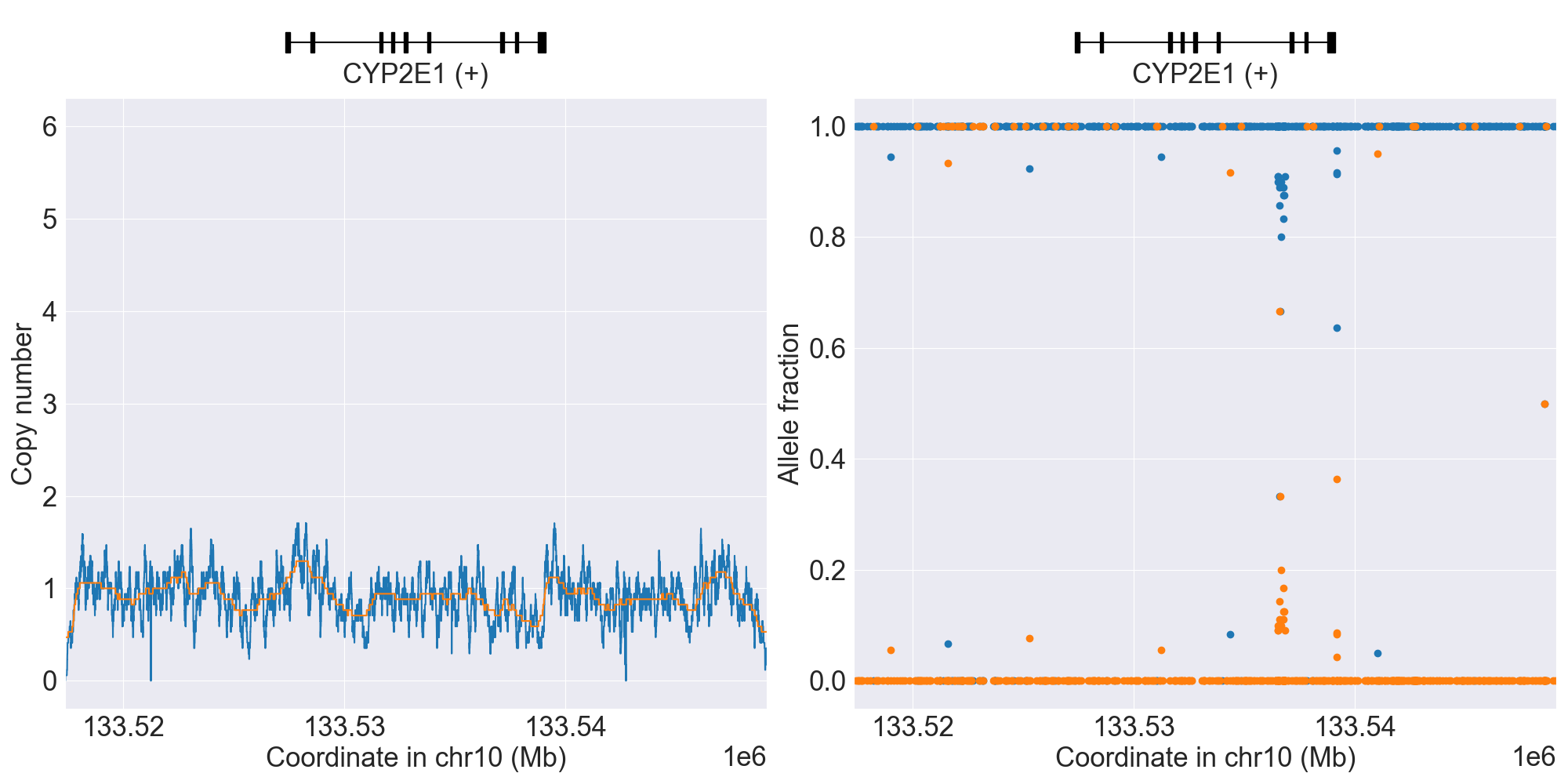
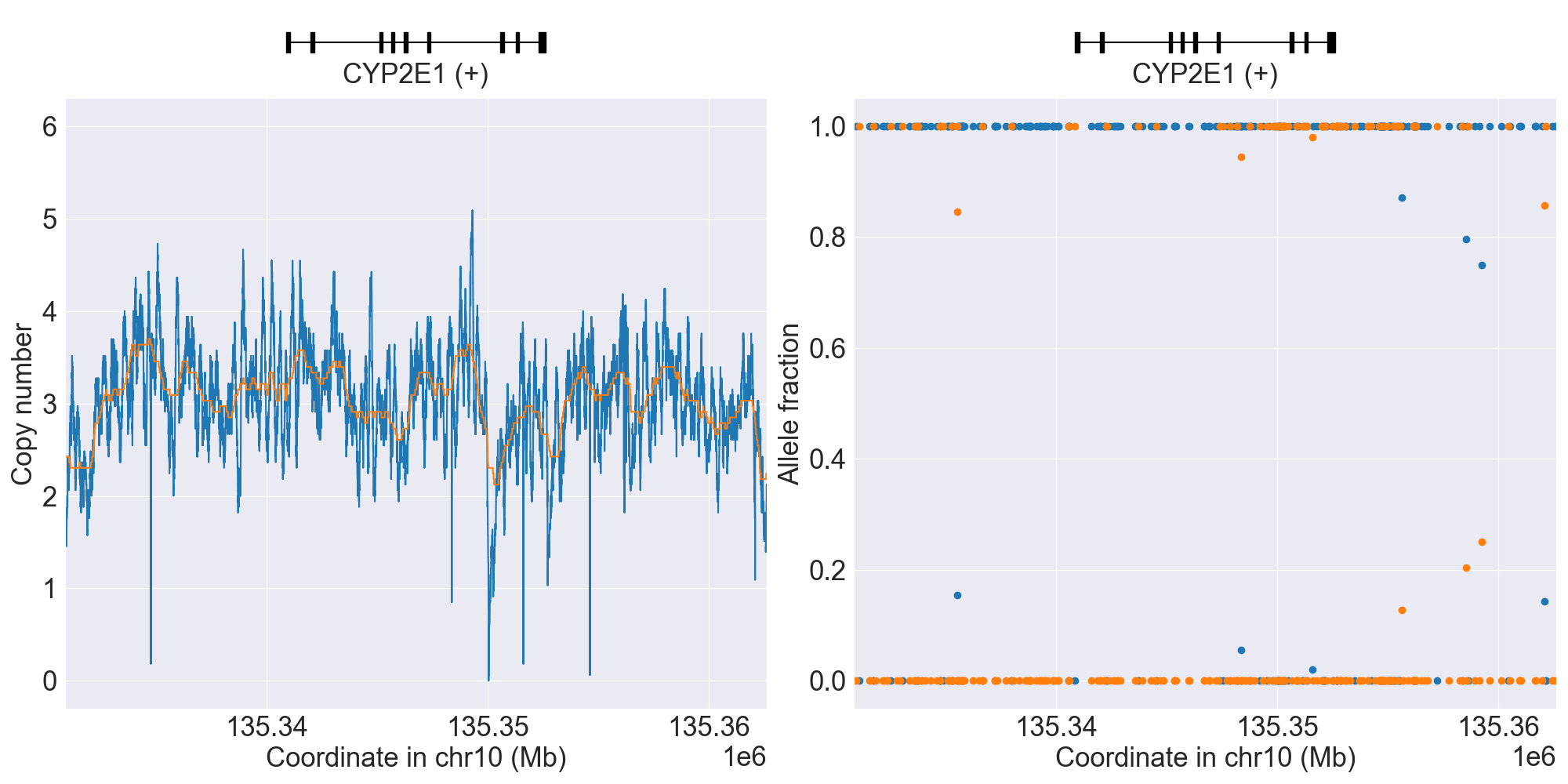
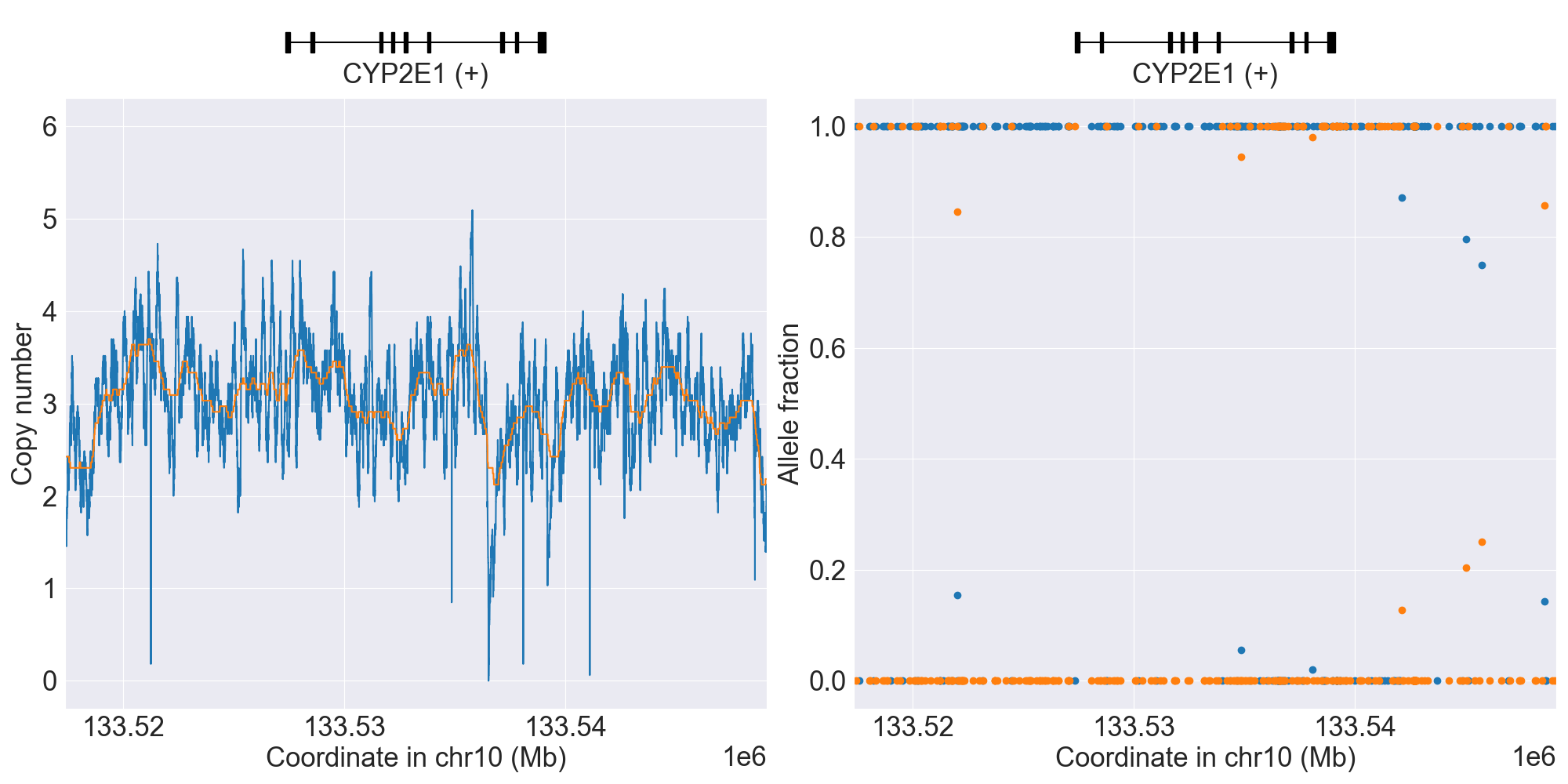
CYP2E1
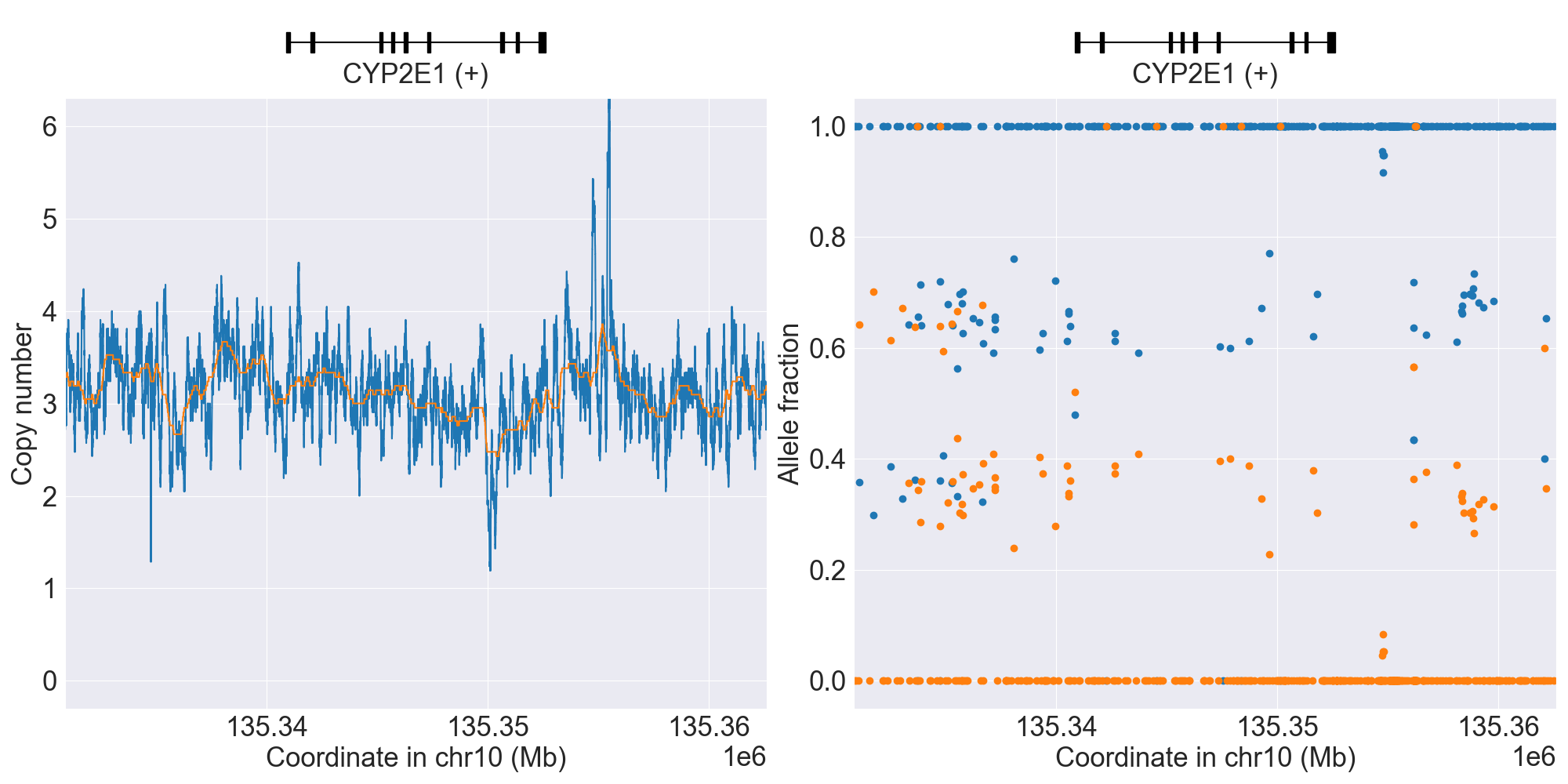
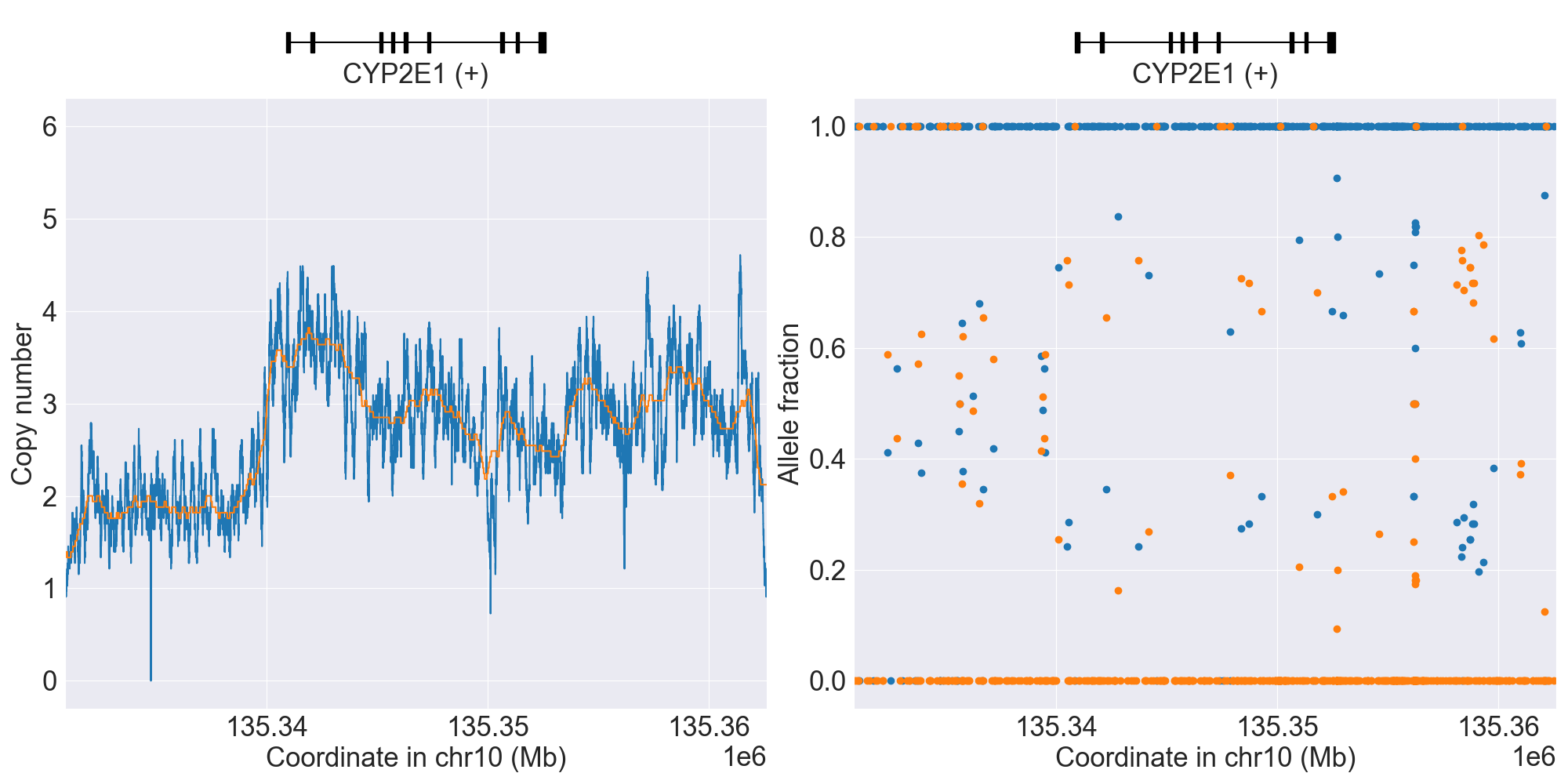
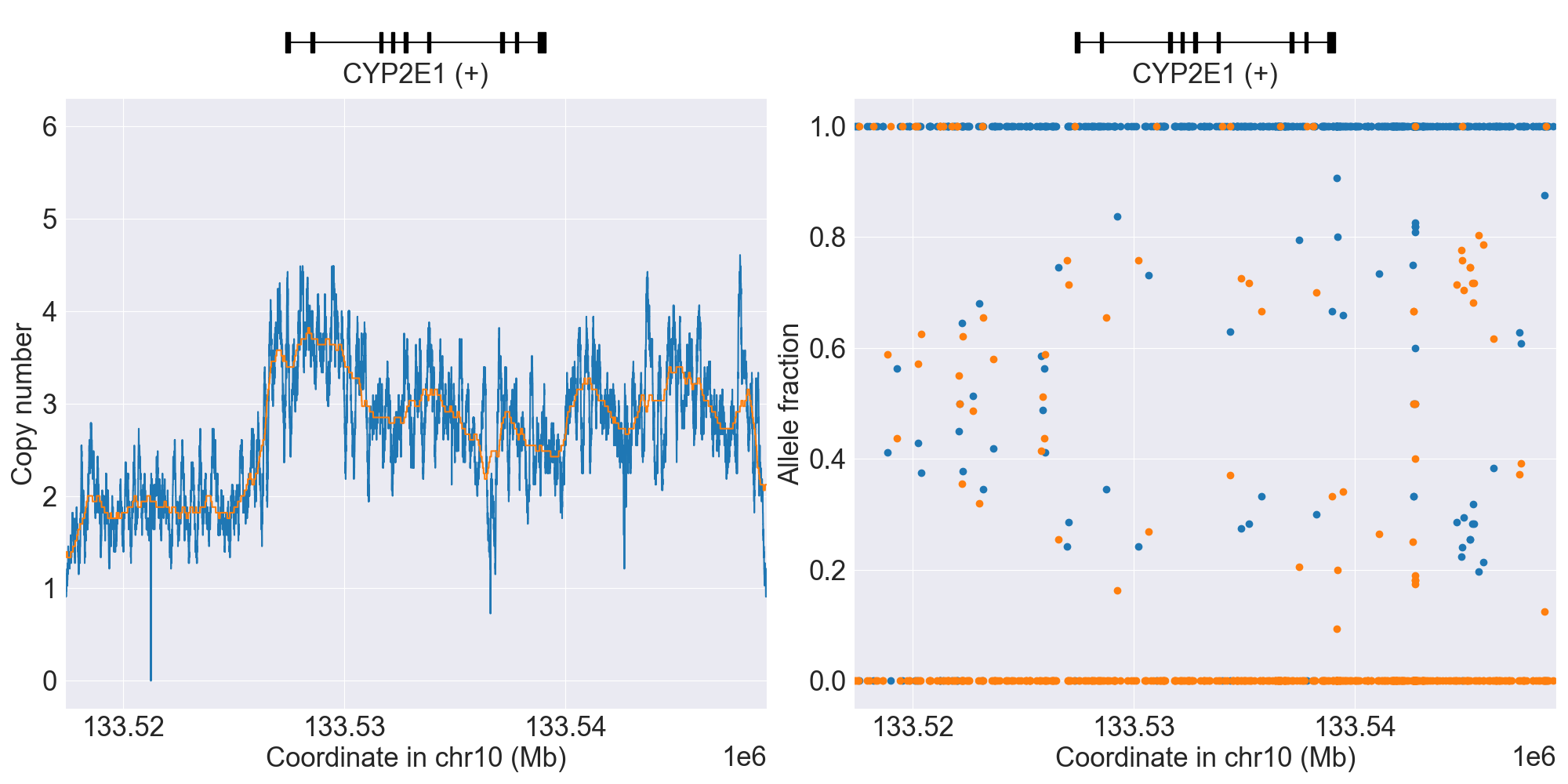
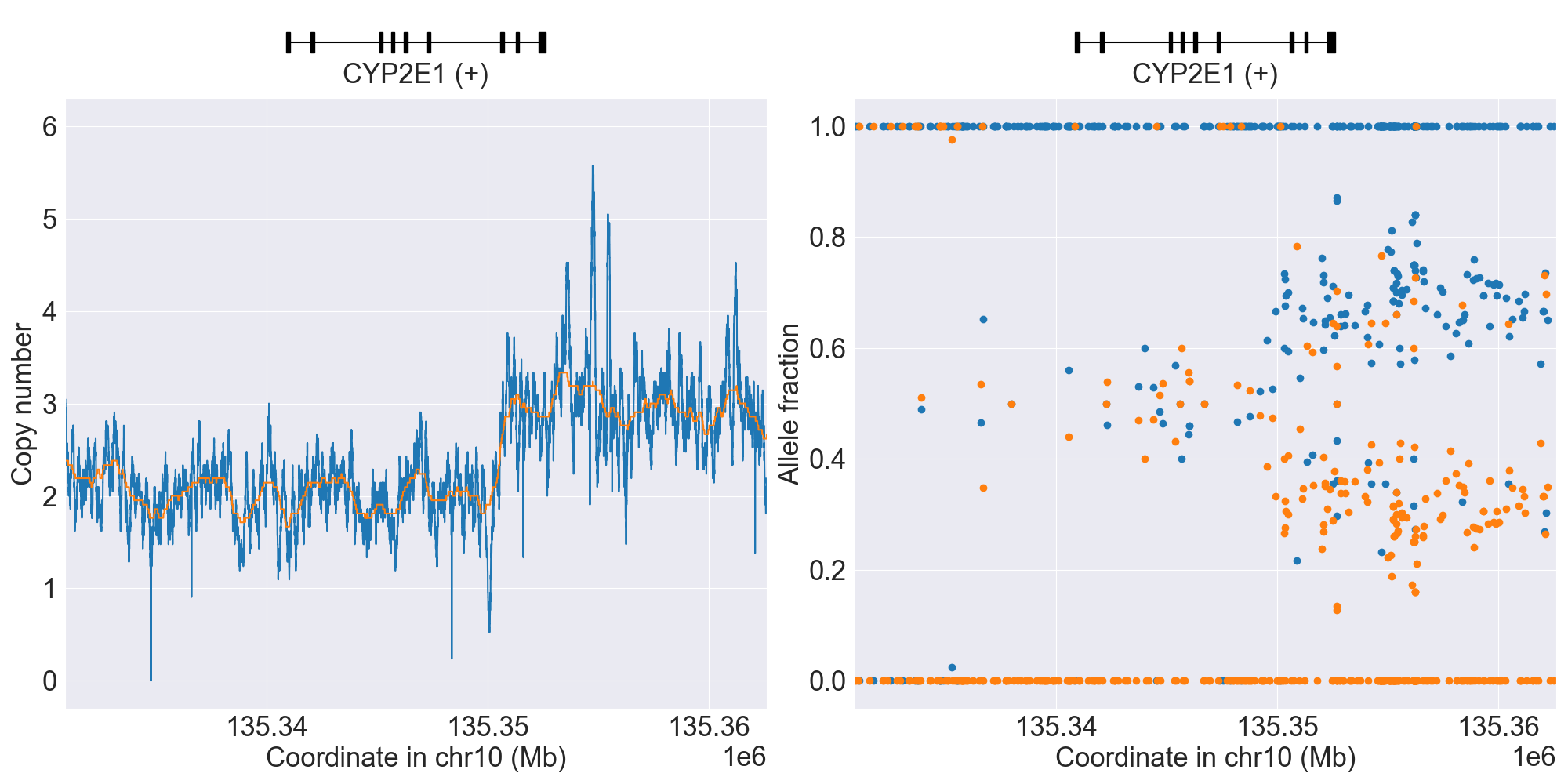
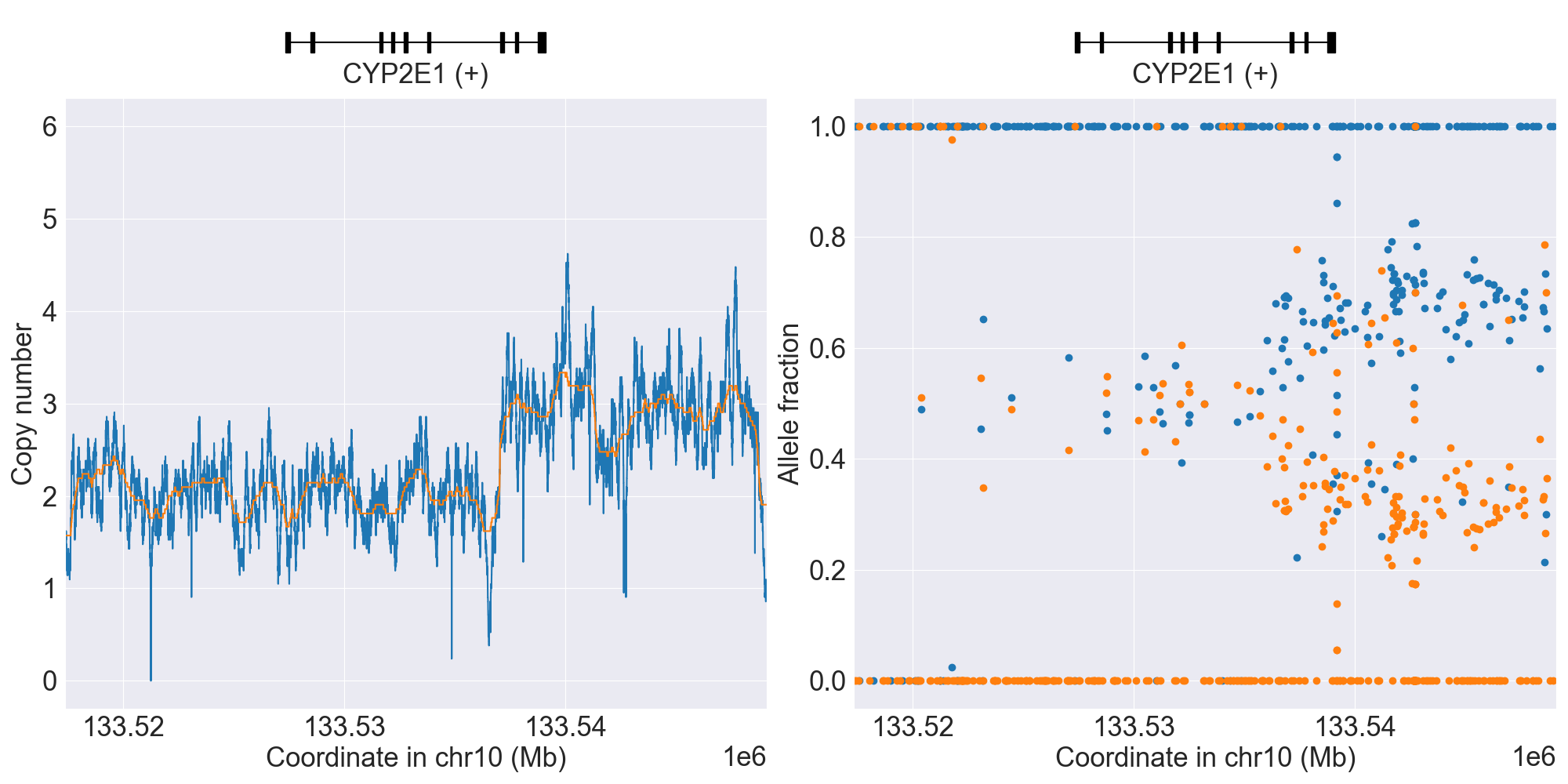
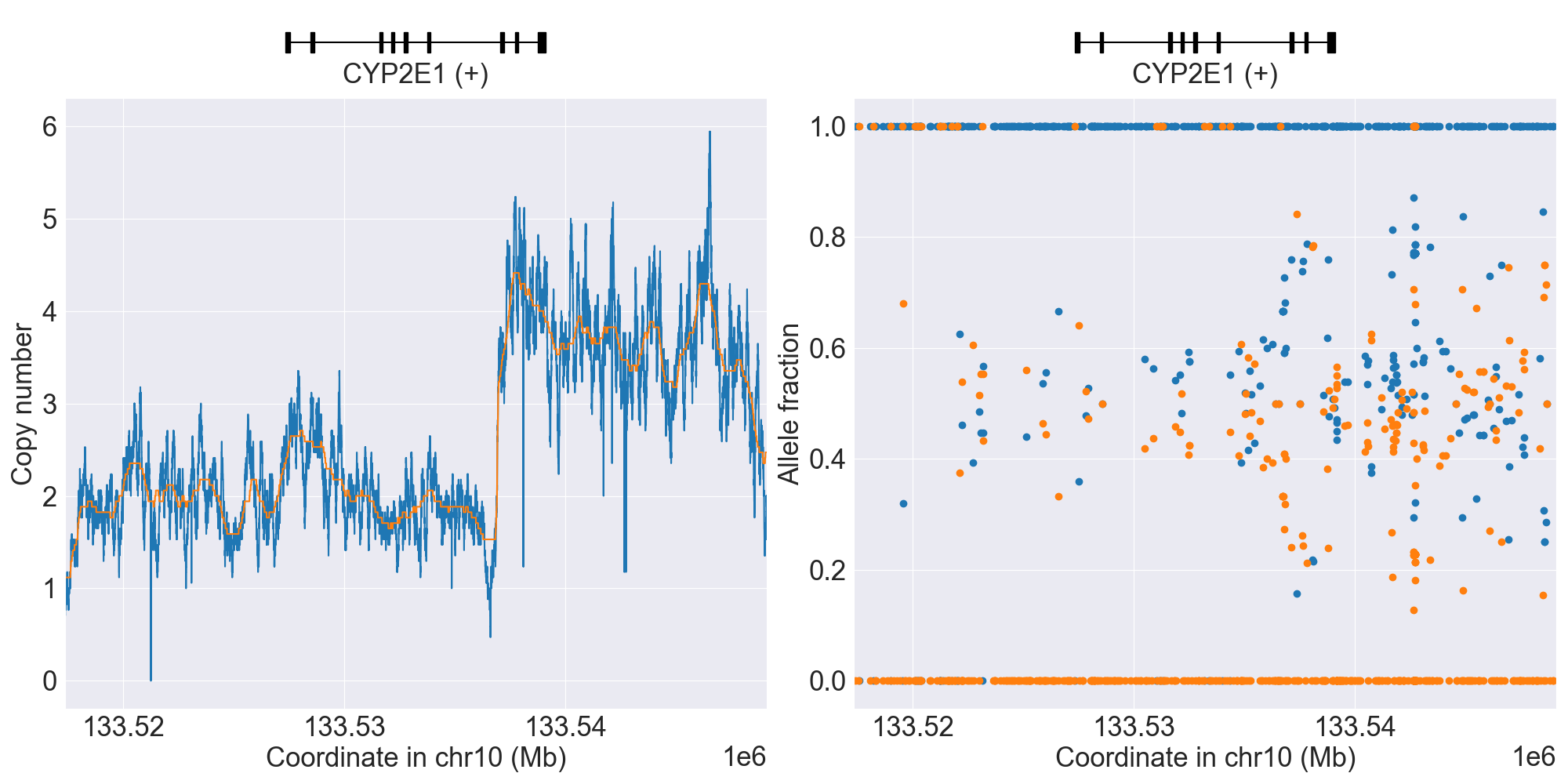
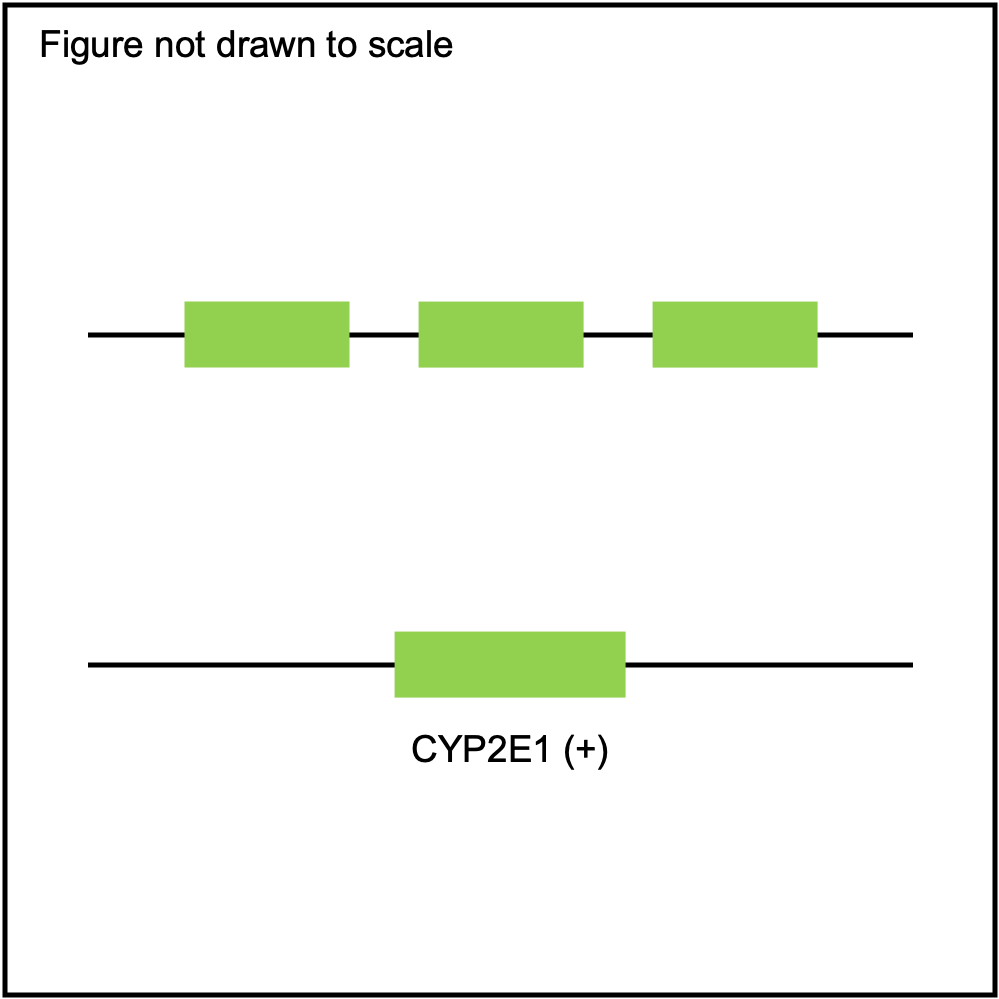
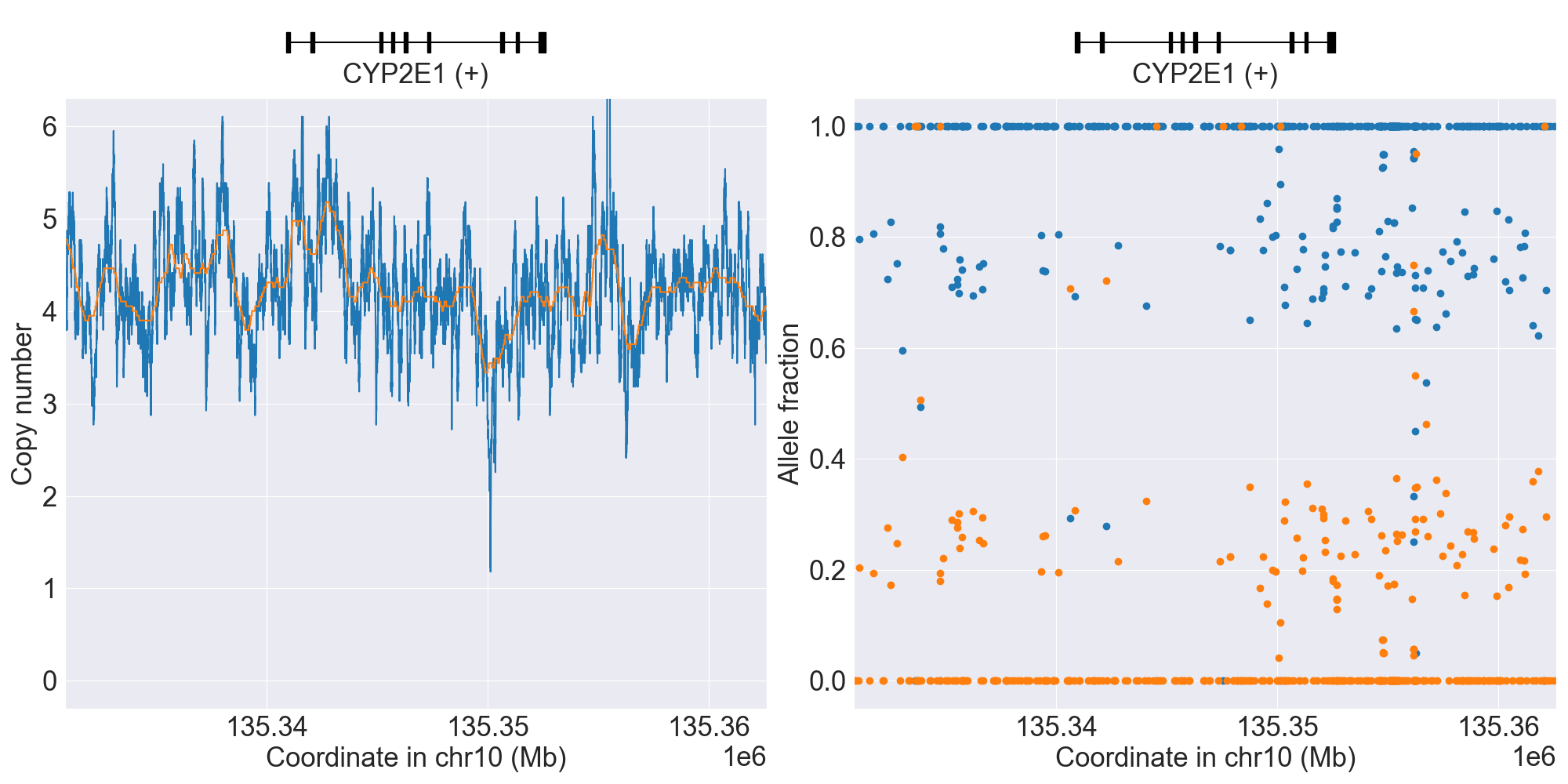
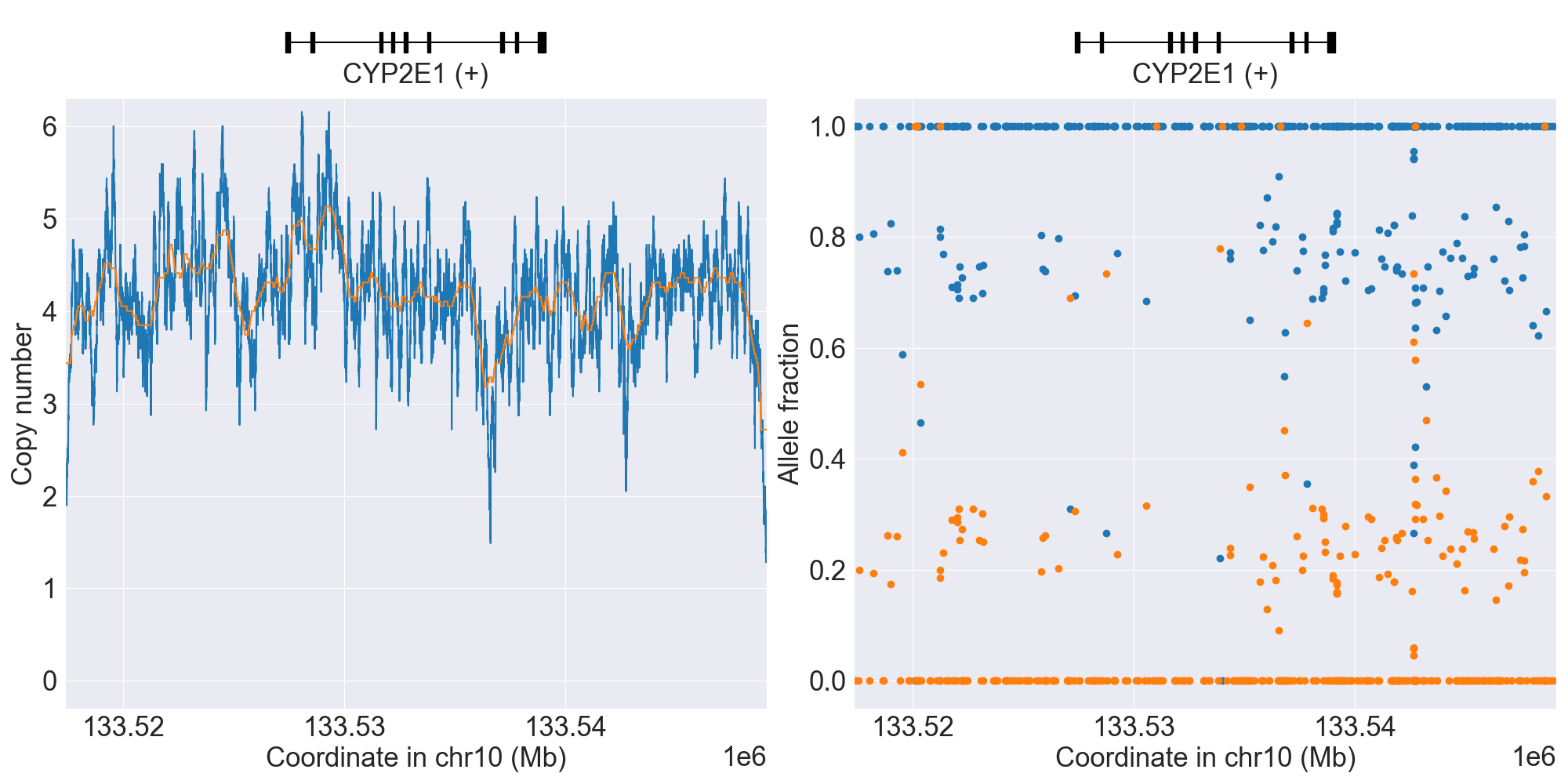
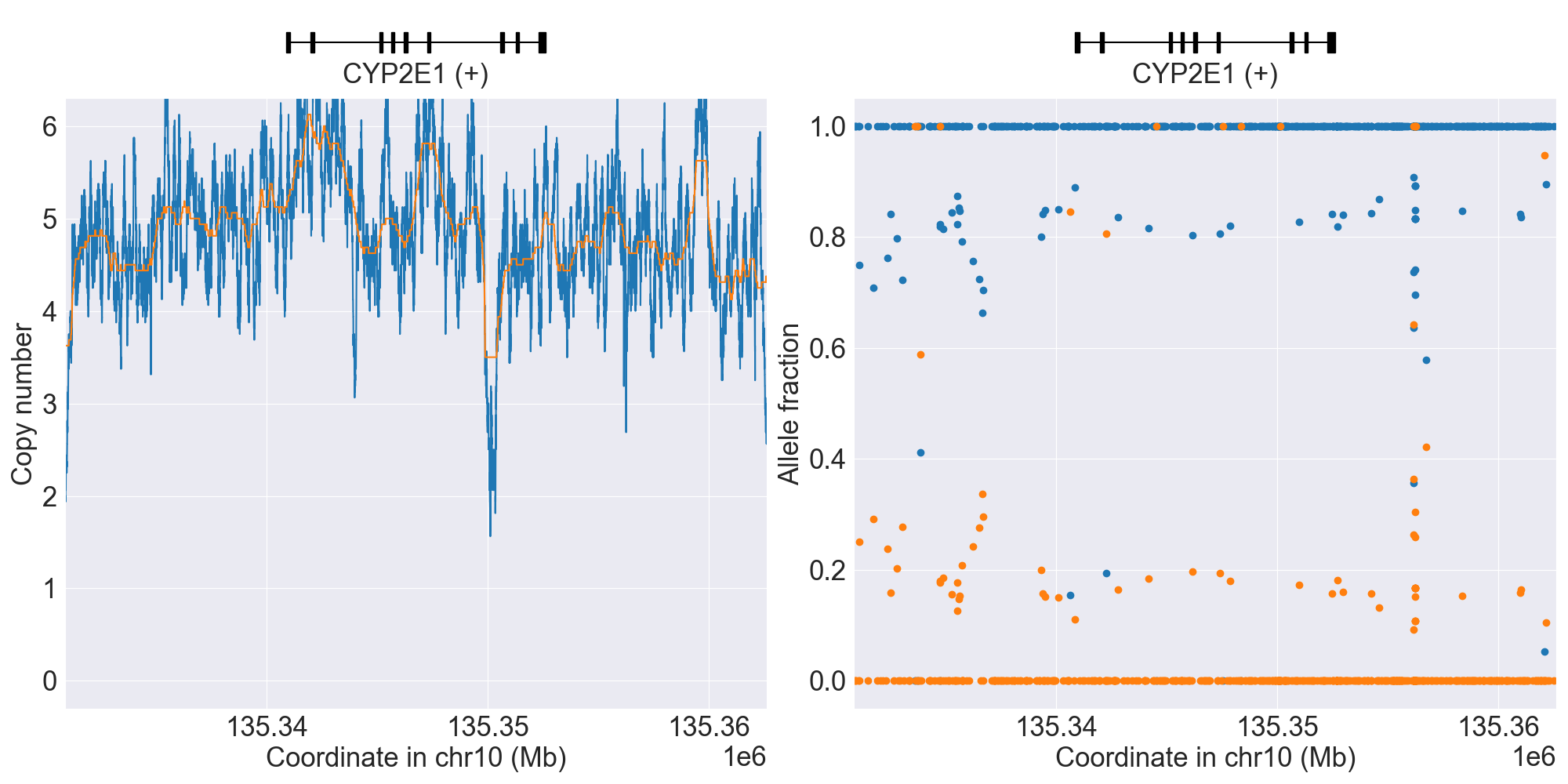
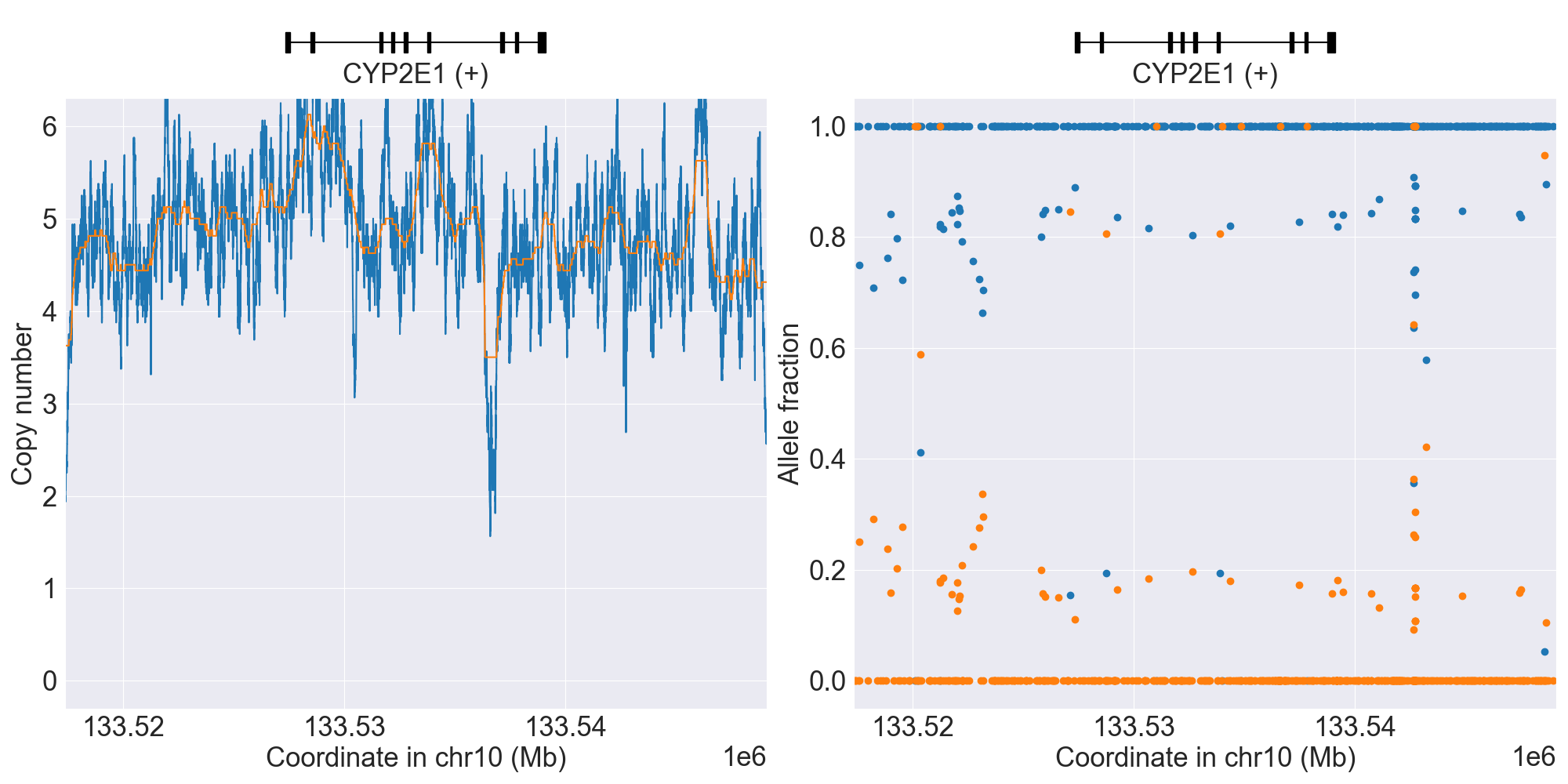
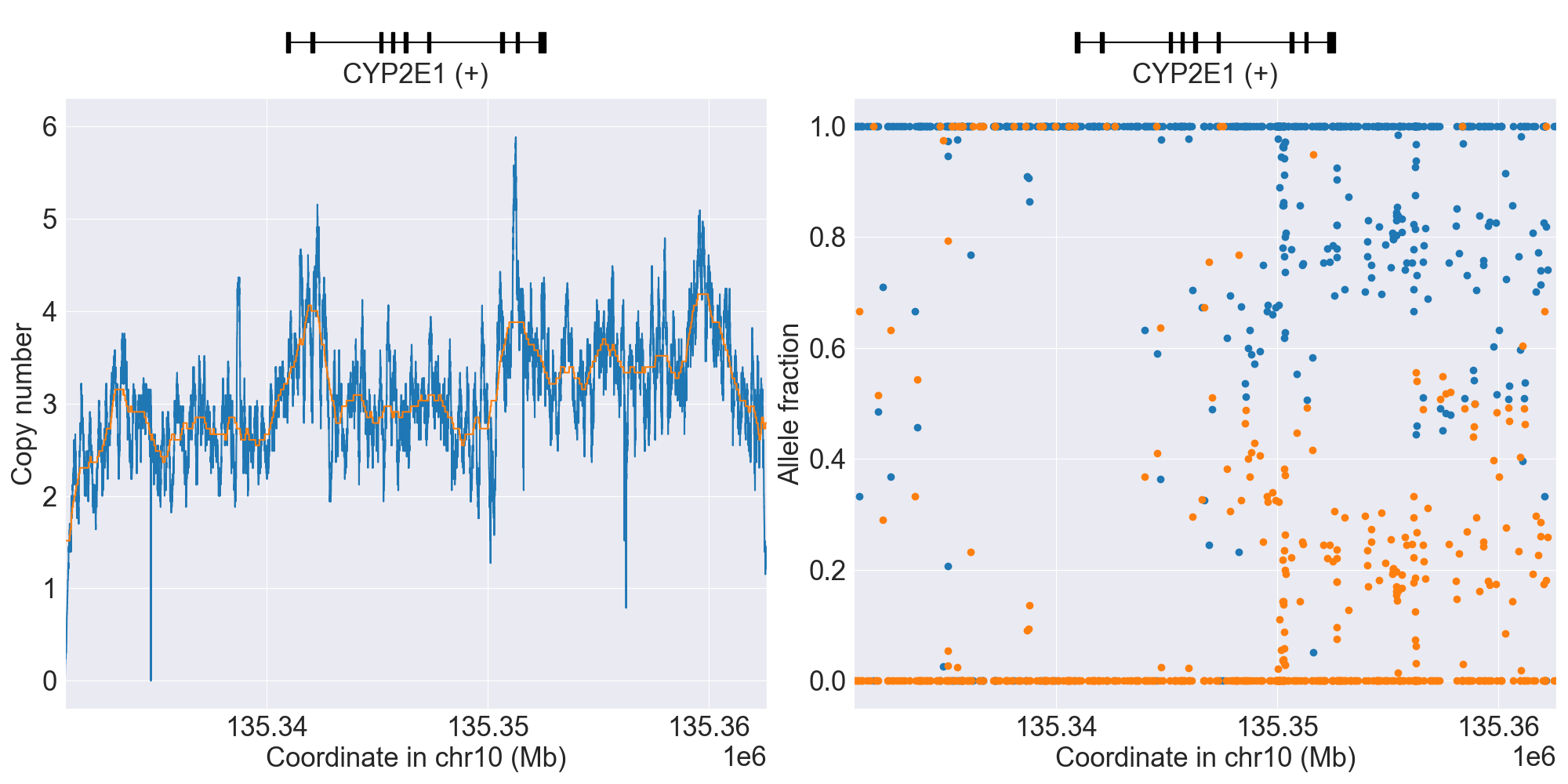
SV summary for CYP2E1
Below is comprehensive summary of SV described from real NGS studies:
SV Alleles |
SV Name |
Genotype |
Reference |
Gene Model |
GRCh37 |
GRCh38 |
Data Type |
Source |
Coriell ID |
Version |
Description |
|---|---|---|---|---|---|---|---|---|---|---|---|
Normal |
*1/*7 |
WGS |
NA10831 |
0.4.1 |
|||||||
WholeDel1 |
Indeterminate |
WGS |
HG03445 |
0.16.0 |
|||||||
*1x2 |
WholeDup1 |
*1/*1x2 |
WGS |
0.4.1 |
|||||||
*7x2 |
WholeDup1 |
*1/*7x2 |
WGS |
NA19095 |
0.4.1 |
||||||
*1x2 |
WholeDup2 |
*1x2/*7 |
WGS |
NA19225 |
0.12.0 |
||||||
*S1 |
PartialDup1 |
*1/*S1 |
WGS |
NA19920 |
0.4.1 |
*S1 is linked to *7. |
|||||
*S1 |
PartialDup1Hom |
*S1/*S1 |
WGS |
NA19309 |
0.13.0 |
||||||
*7x3 |
WholeMultip1 |
*7/*7x3 |
WGS |
NA19908 |
0.4.1 |
||||||
WholeMultip2 |
Indeterminate |
WGS |
NA20291 |
0.14.0 |
|||||||
WholeDup1+PartialDup1 |
Indeterminate |
WGS |
HG03401 |
0.16.0 |
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
PyPGx was recently applied to the entire high-coverage WGS dataset from 1KGP (N=2,504). Click here to see individual SV calls for CYP2E1, and corresponding copy number profiles and allele fraction profiles.
Resources for CYP2E1
CYP2F1
Resources for CYP2F1
CYP2J2
Resources for CYP2J2
CYP2R1
Resources for CYP2R1
CYP2S1
Resources for CYP2S1
CYP2W1
Resources for CYP2W1
CYP3A4
Resources for CYP3A4
CYP3A5
Phenotype summary for CYP3A5
Diplotype-phenotype mapping is used for phenotype prediction.
Phenotype |
Example |
Priority |
|---|---|---|
Normal Metabolizer |
*1/*1 |
Abnormal/Priority/High Risk |
Intermediate Metabolizer |
*1/*3 |
Abnormal/Priority/High Risk |
Possible Intermediate Metabolizer |
*1/*2 |
Abnormal/Priority/High Risk |
Poor Metabolizer |
*6/*6 |
Normal/Routine/Low Risk |
Indeterminate |
*2/*2 |
None |
Recommendations for CYP3A5
Tacrolimus
“The CPIC dosing guideline for tacrolimus recommends increasing the starting dose by 1.5 to 2 times the recommended starting dose in patients who are CYP3A5 intermediate or extensive metabolizers, though total starting dose should not exceed 0.3 mg/kg/day. Therapeutic drug monitoring should also be used to guide dose adjustments.” (Source: PharmGKB)
Resources for CYP3A5
CYP3A7
Resources for CYP3A7
CYP3A43
Resources for CYP3A43
CYP4A11
Resources for CYP4A11
CYP4A22
Resources for CYP4A22
CYP4B1
Resources for CYP4B1
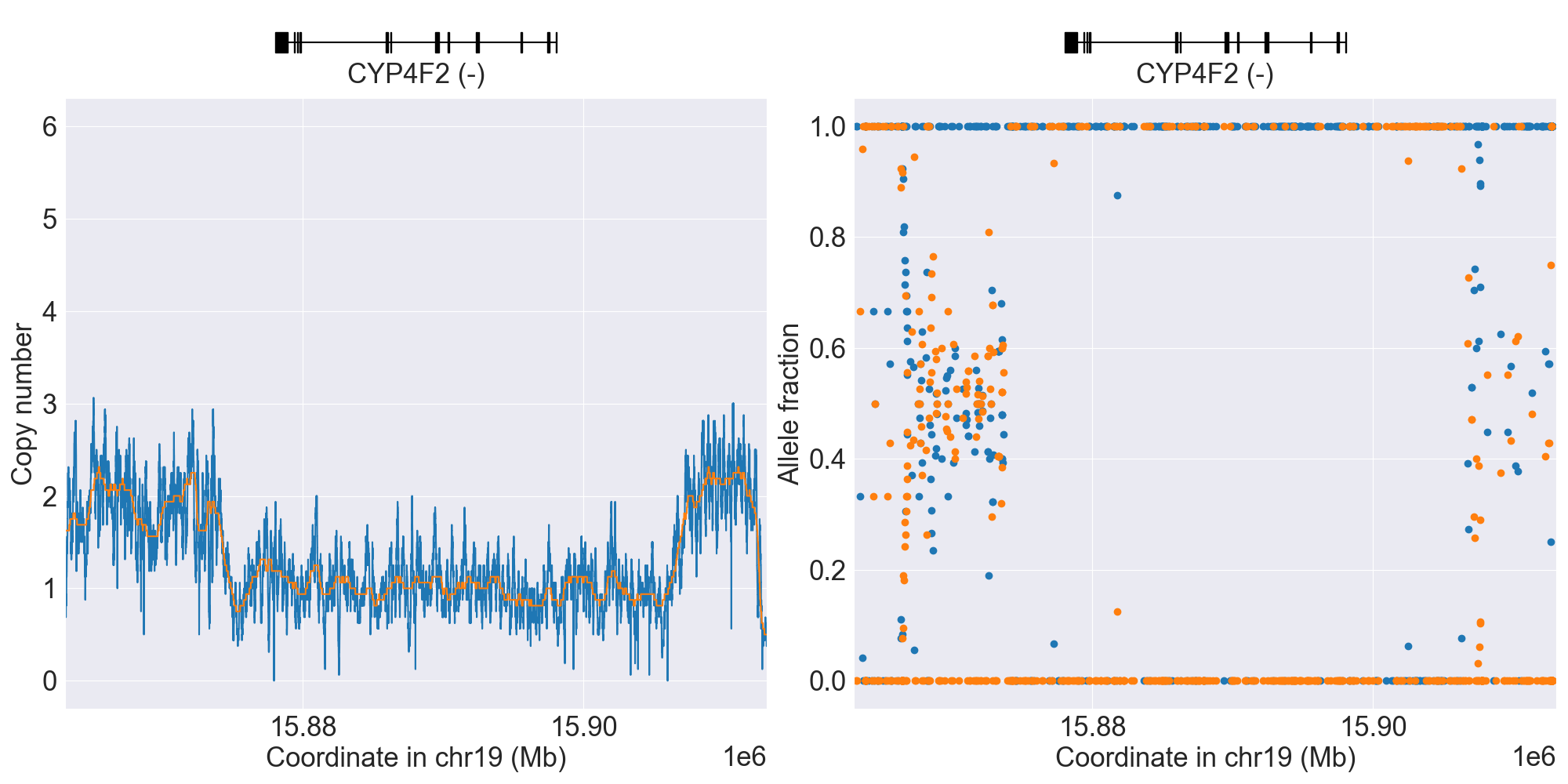
CYP4F2
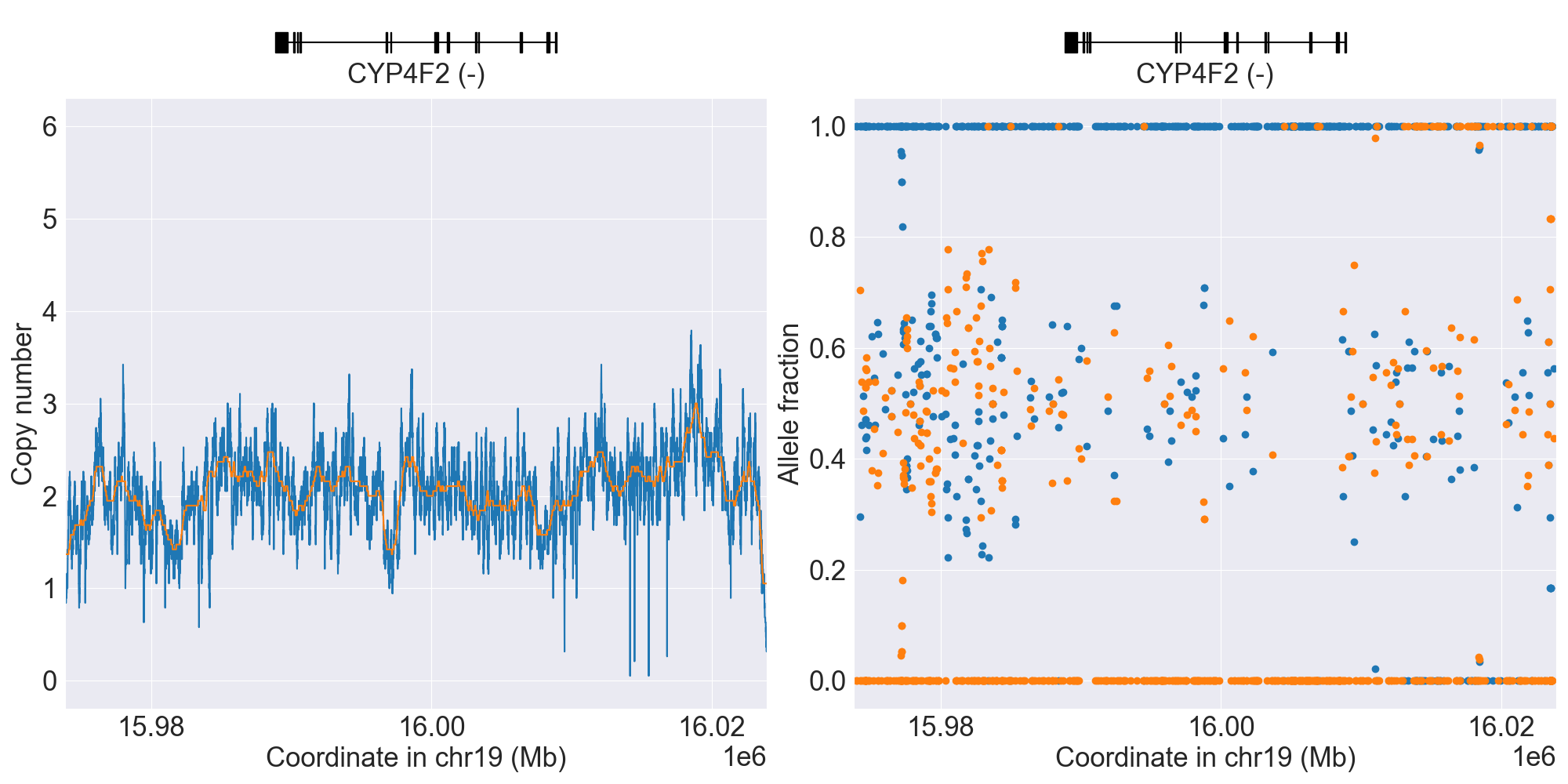
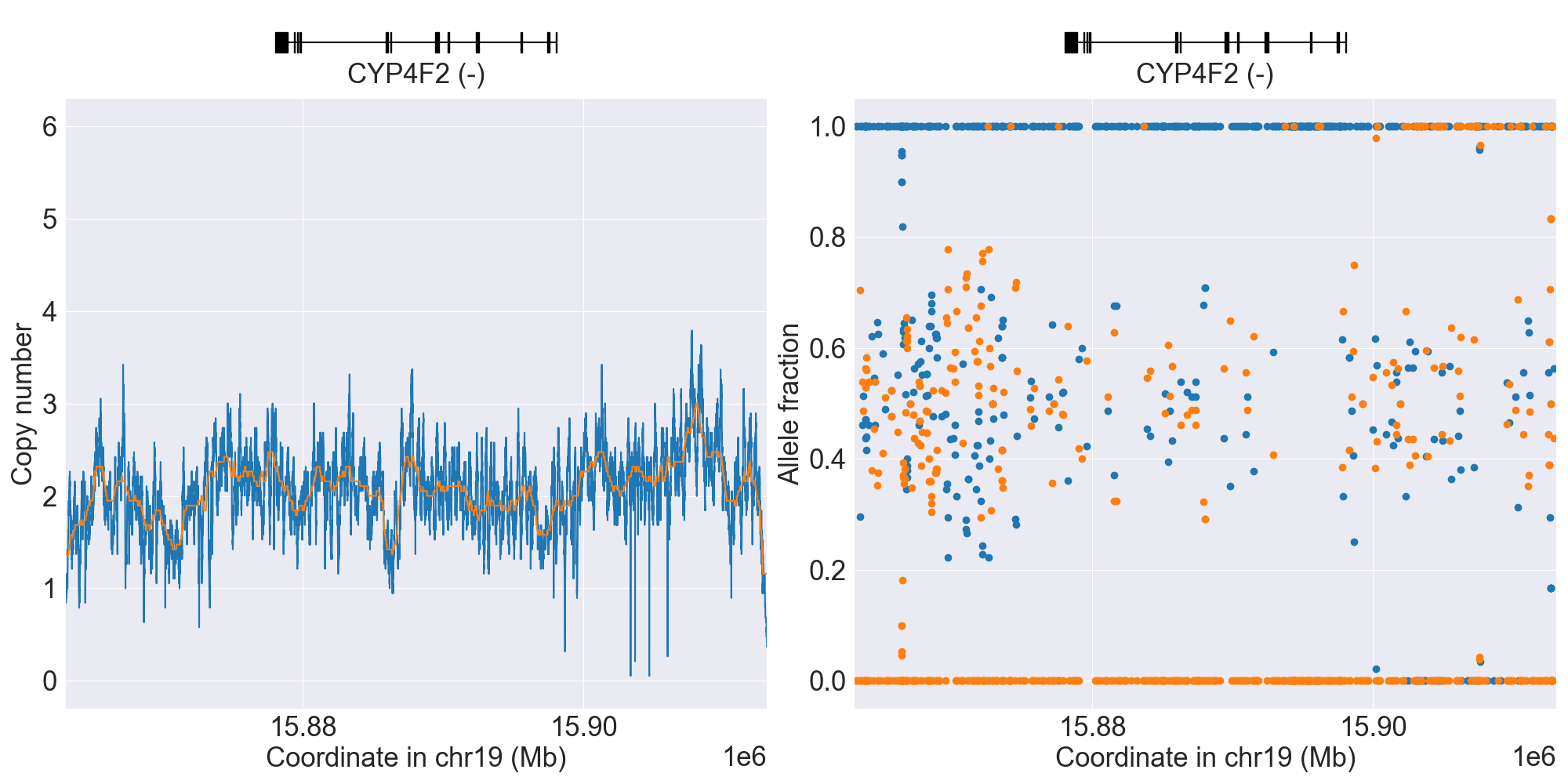
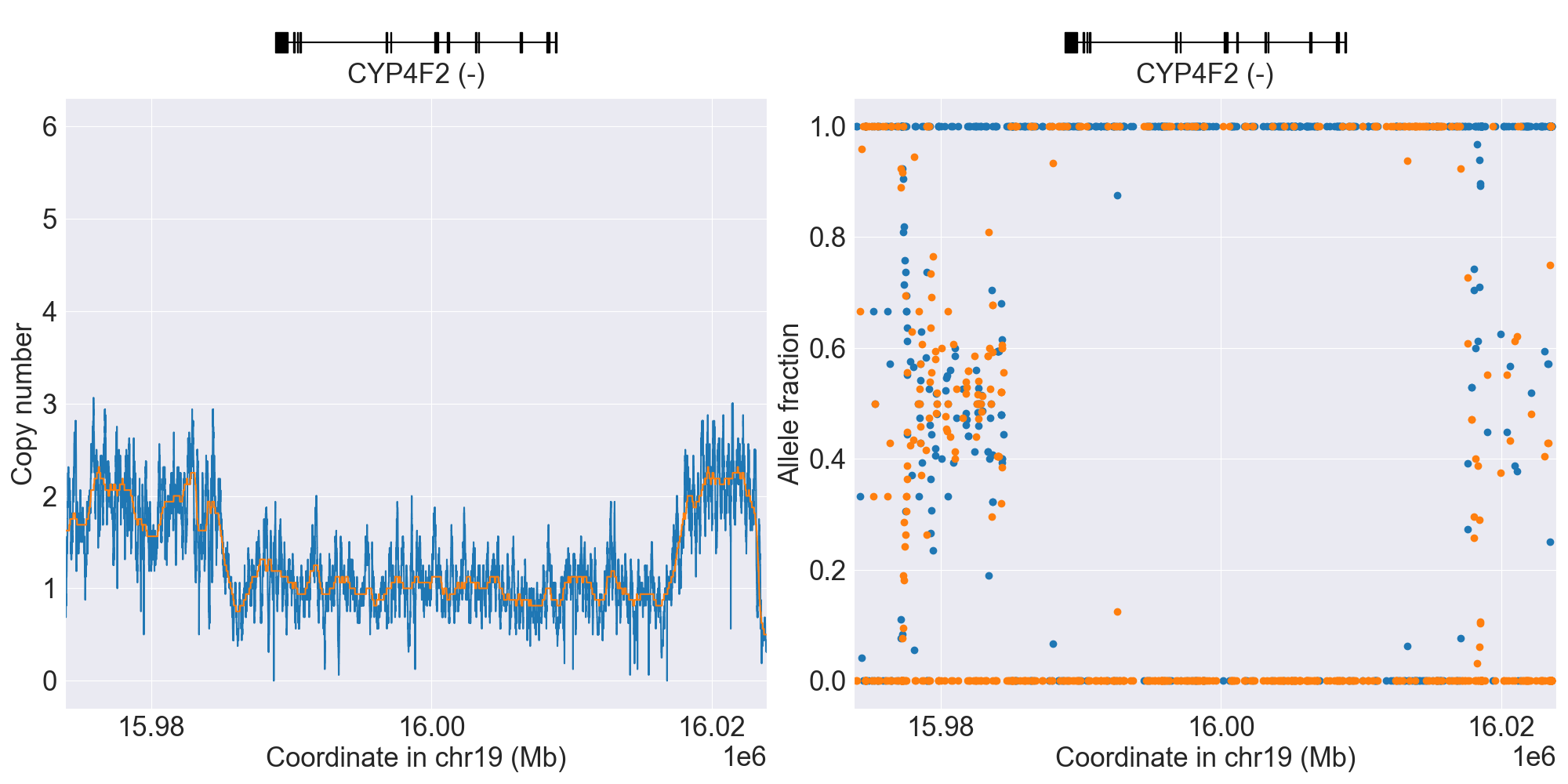
SV summary for CYP4F2
Below is comprehensive summary of SV described from real NGS studies:
SV Alleles |
SV Name |
Genotype |
Reference |
Gene Model |
GRCh37 |
GRCh38 |
Data Type |
Source |
Coriell ID |
Version |
Description |
|---|---|---|---|---|---|---|---|---|---|---|---|
Normal |
*1/*3 |
WGS |
HG01190 |
0.11.0 |
|||||||
*DEL |
WholeDel1 |
*1/*DEL |
WGS |
0.11.0 |
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
PyPGx was recently applied to the entire high-coverage WGS dataset from 1KGP (N=2,504). Click here to see individual SV calls for CYP4F2, and corresponding copy number profiles and allele fraction profiles.
Resources for CYP4F2
CYP17A1
Resources for CYP17A1
CYP19A1
Resources for CYP19A1
CYP26A1
Resources for CYP26A1
DPYD
Phenotype summary for DPYD
Activity score is used for phenotype prediction.
Phenotype |
Activity Score |
Example |
Priority |
|---|---|---|---|
Normal Metabolizer |
2 == score |
Reference/Reference |
Normal/Routine/Low Risk |
Intermediate Metabolizer |
1 <= score < 2 |
Reference/c.1905+1G>A (*2A) |
Abnormal/Priority/High Risk |
Poor Metabolizer |
0 <= score < 1 |
c.295_298delTCAT (*7)/c.703C>T (*8) |
Abnormal/Priority/High Risk |
Recommendations for DPYD
Capecitabine
“The CPIC Dosing Guideline for 5-fluorouracil and capecitabine recommends an alternative drug for patients who are DPYD poor metabolizers with an activity score of 0. In those who are poor metabolizers with an activity score of 0.5, an alternative drug is also recommended, but if this is not considered a suitable therapeutic option, 5-fluorouracil or capecitabine should be administered at a strongly reduced dose with early therapeutic drug monitoring. Patients who are intermediate metabolizers with an activity score of 1 or 1.5 should receive a dose reduction of 50%. Patients with the c.[2846A>T];[2846A>T] genotype may require a >50% dose reduction.” (Source: PharmGKB)
Fluorouracil
“The CPIC Dosing Guideline for 5-fluorouracil and capecitabine recommends an alternative drug for patients who are DPYD poor metabolizers with an activity score of 0. In those who are poor metabolizers with an activity score of 0.5, an alternative drug is also recommended, but if this is not considered a suitable therapeutic option, 5-fluorouracil or capecitabine should be administered at a strongly reduced dose with early therapeutic drug monitoring. Patients who are intermediate metabolizers with an activity score of 1 or 1.5 should receive a dose reduction of 50%. Patients with the c.[2846A>T];[2846A>T] genotype may require a >50% dose reduction.” (Source: PharmGKB)
Resources for DPYD
F5
Phenotype summary for F5
Diplotype-phenotype mapping is used for phenotype prediction.
Phenotype
Example
Priority
Favorable Response
Reference/Reference
None
Unfavorable Response
Reference/Leiden
None
Recommendations for F5
Hormonal contraceptives
“In individuals who carry the Factor V Leiden allele (rs6025 T) and have a family history of thrombotic events, estrogen-containing oral contraceptives should be avoided and alternative forms of contraception used.” (Source: PharmGKB)
Resources for F5
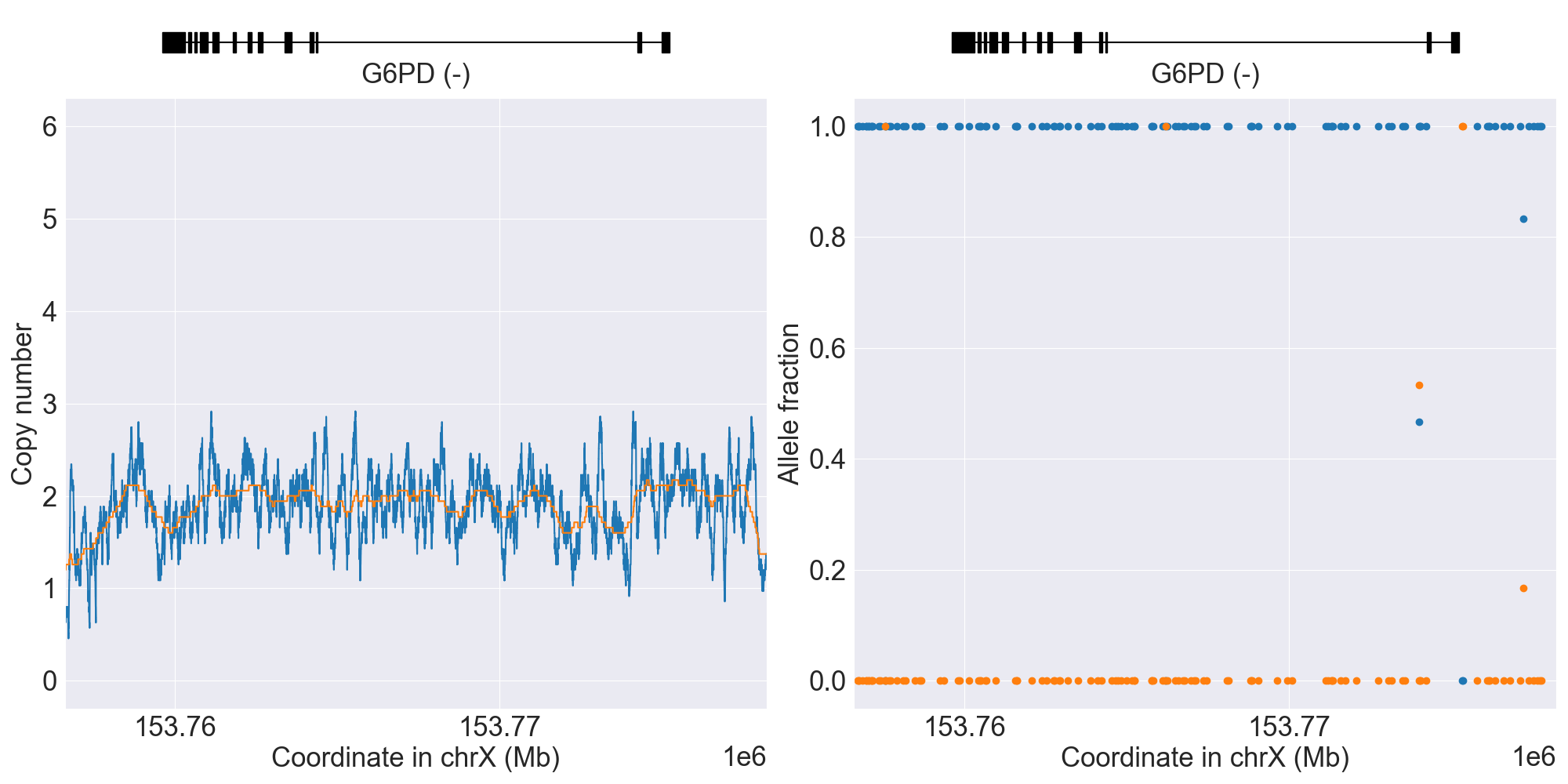
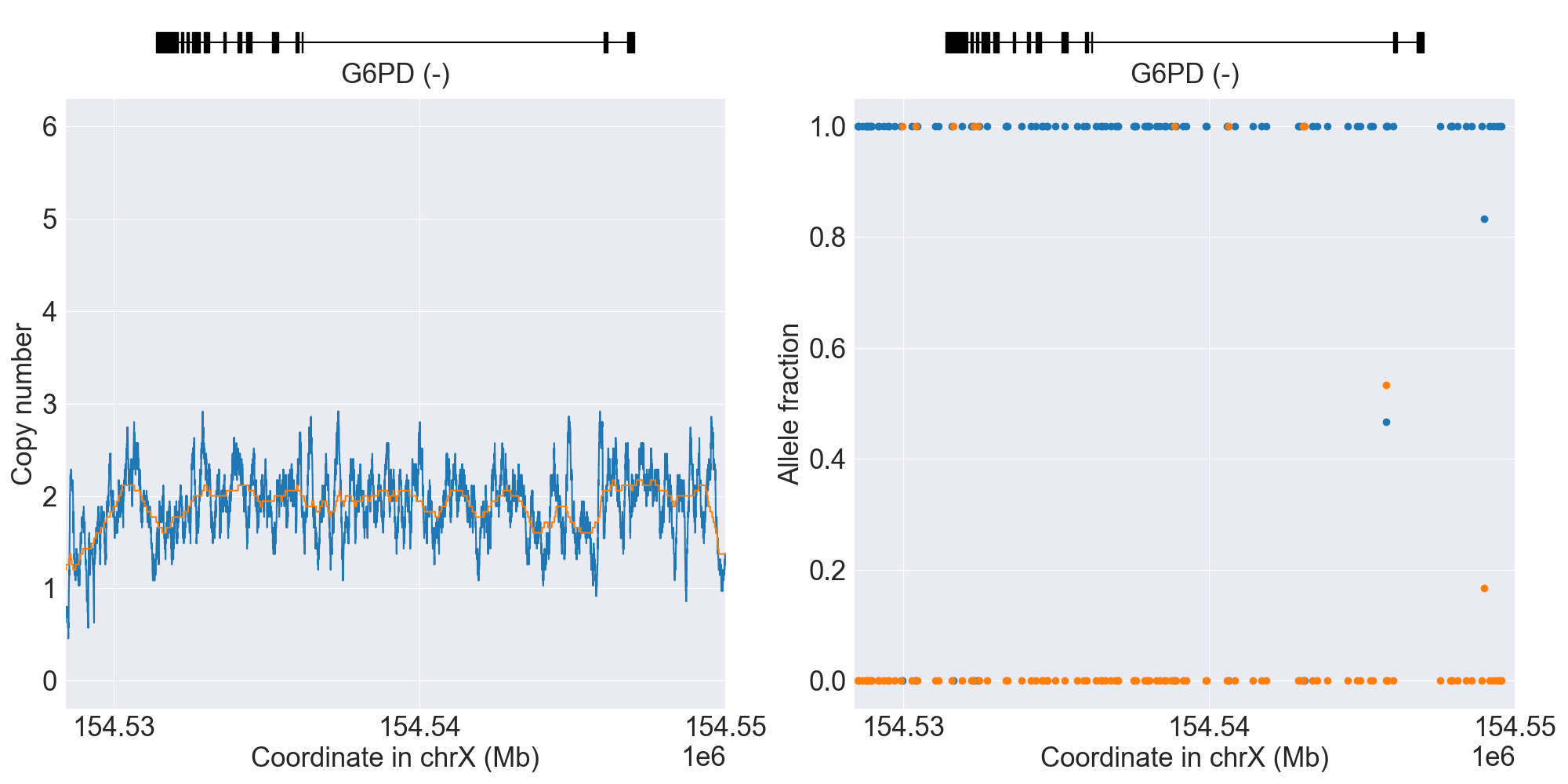
G6PD
SV summary for G6PD
Since the gene is located on X chromosome, its copy number differs between females (N=2) and males (N=1). Technically speaking, this difference is not a SV event, but it is treated as such by PyPGx for genotyping purposes (i.e. sex determination).
Below is comprehensive summary of SV described from real NGS studies:
SV Alleles |
SV Name |
Genotype |
Reference |
Gene Model |
GRCh37 |
GRCh38 |
Data Type |
Source |
Coriell ID |
Version |
Description |
|---|---|---|---|---|---|---|---|---|---|---|---|
Female |
B (reference)/B (reference) |
WGS |
HG00276 |
0.12.0 |
|||||||
MALE |
Male |
MALE/B (reference) |
WGS |
HG00436 |
0.12.0 |
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
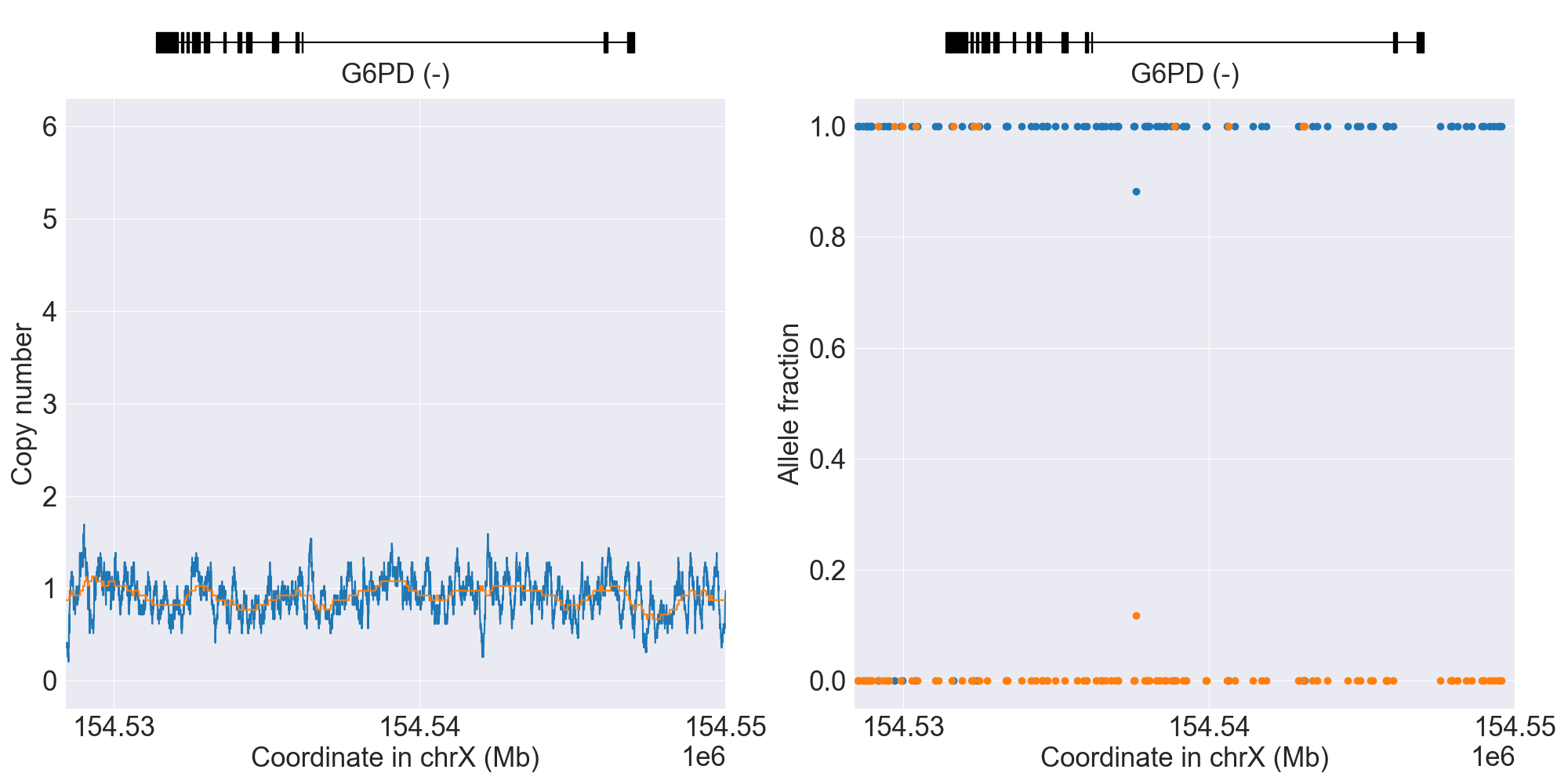
PyPGx was recently applied to the entire high-coverage WGS dataset from 1KGP (N=2,504). Click here to see individual SV calls for G6PD, and corresponding copy number profiles and allele fraction profiles.
Phenotype summary for G6PD
Diplotype-phenotype mapping is used for phenotype prediction.
Phenotype
Example
Priority
G6PD Normal
A/B (reference)
Normal Risk
G6PD Deficient with CNSHA
Alhambra/Bari
Abnormal/Priority/High Risk
G6PD Variable
202G>A_376A>G_1264C>G/B (reference)
Abnormal/Priority/High Risk
G6PD Deficient
202G>A_376A>G_1264C>G/A- 680T_376G
Abnormal/Priority/High Risk
G6PD Indeterminate
A- 202A_376G/Dagua
Abnormal/Priority/High Risk
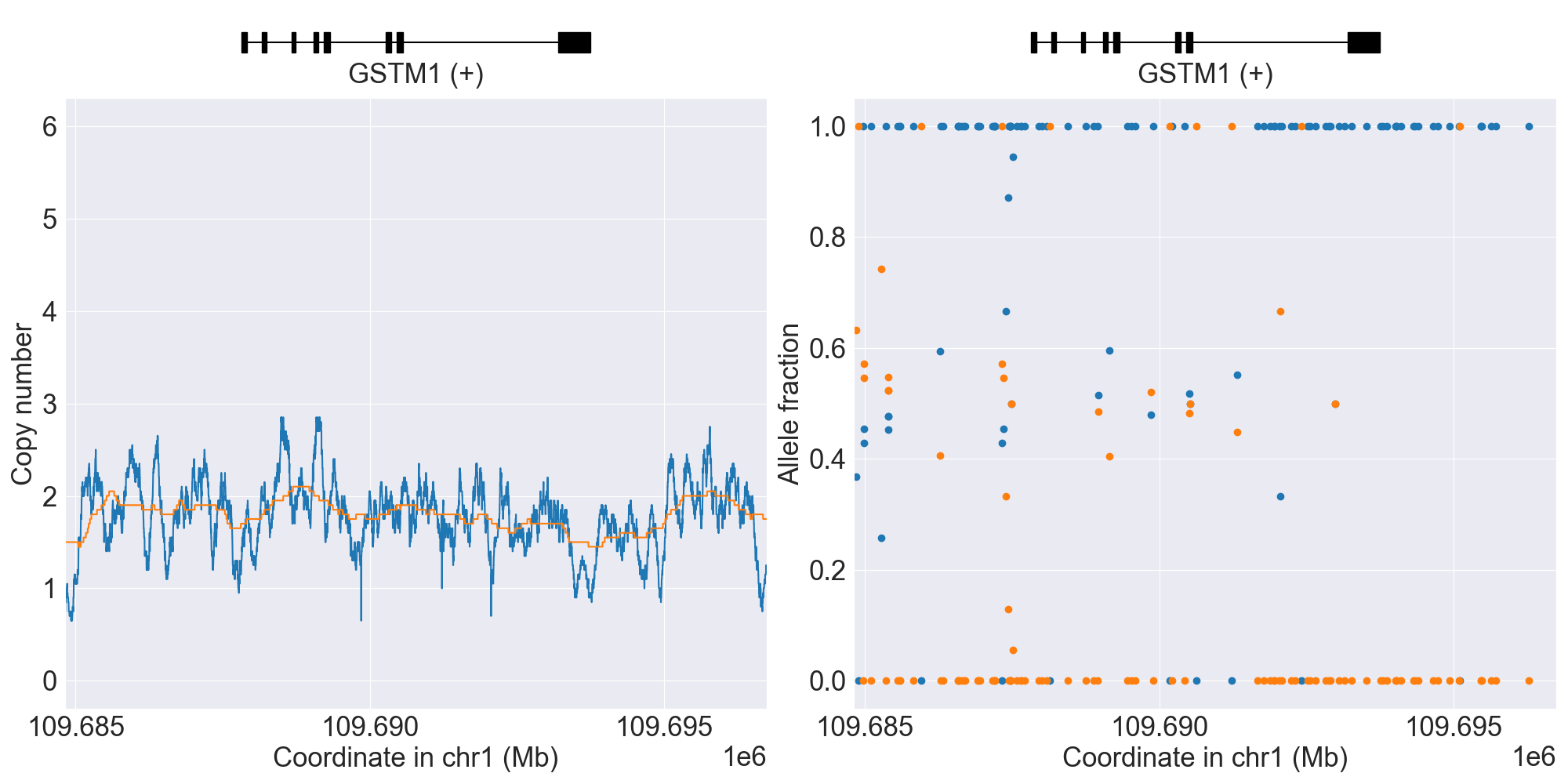
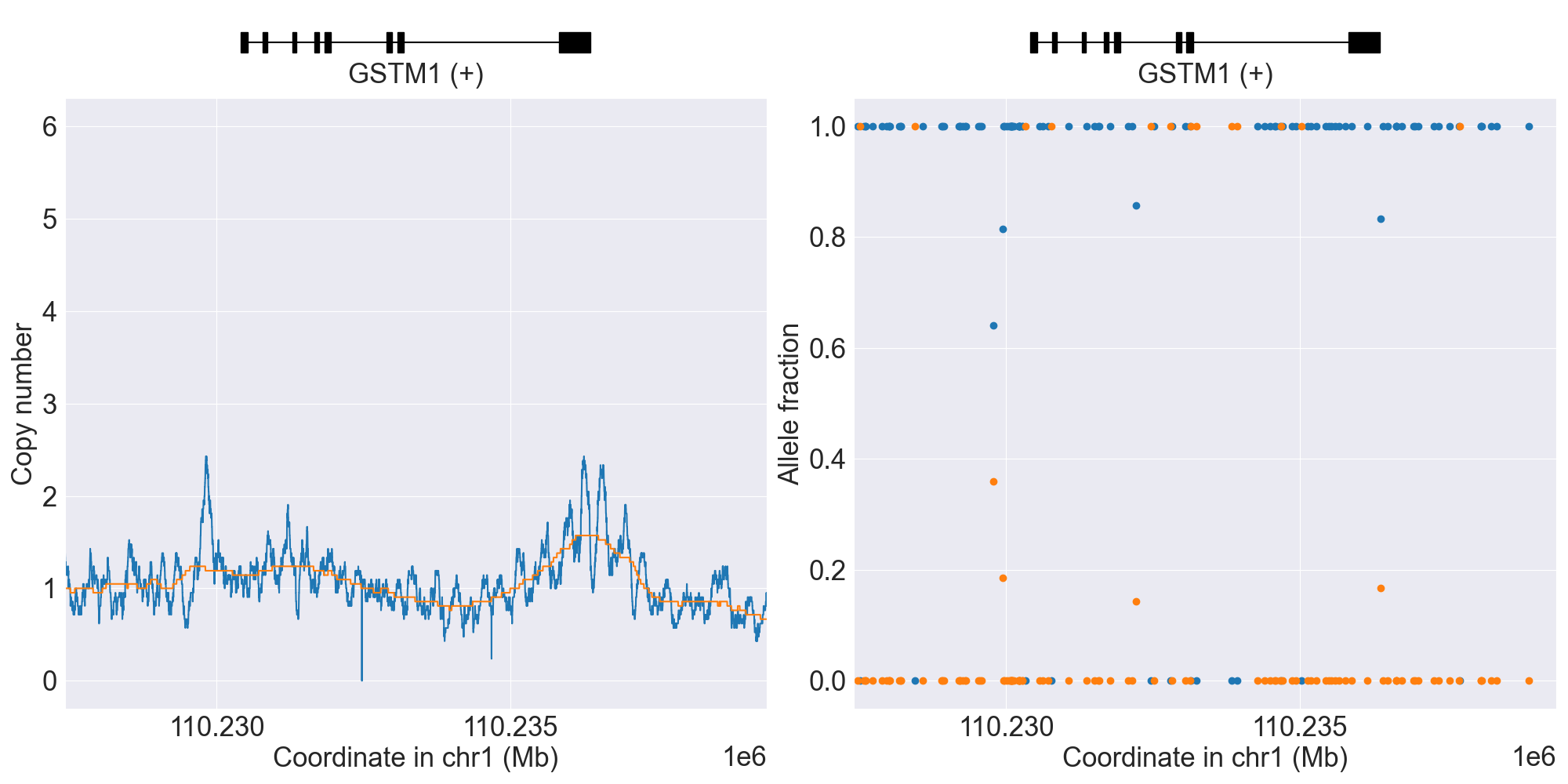
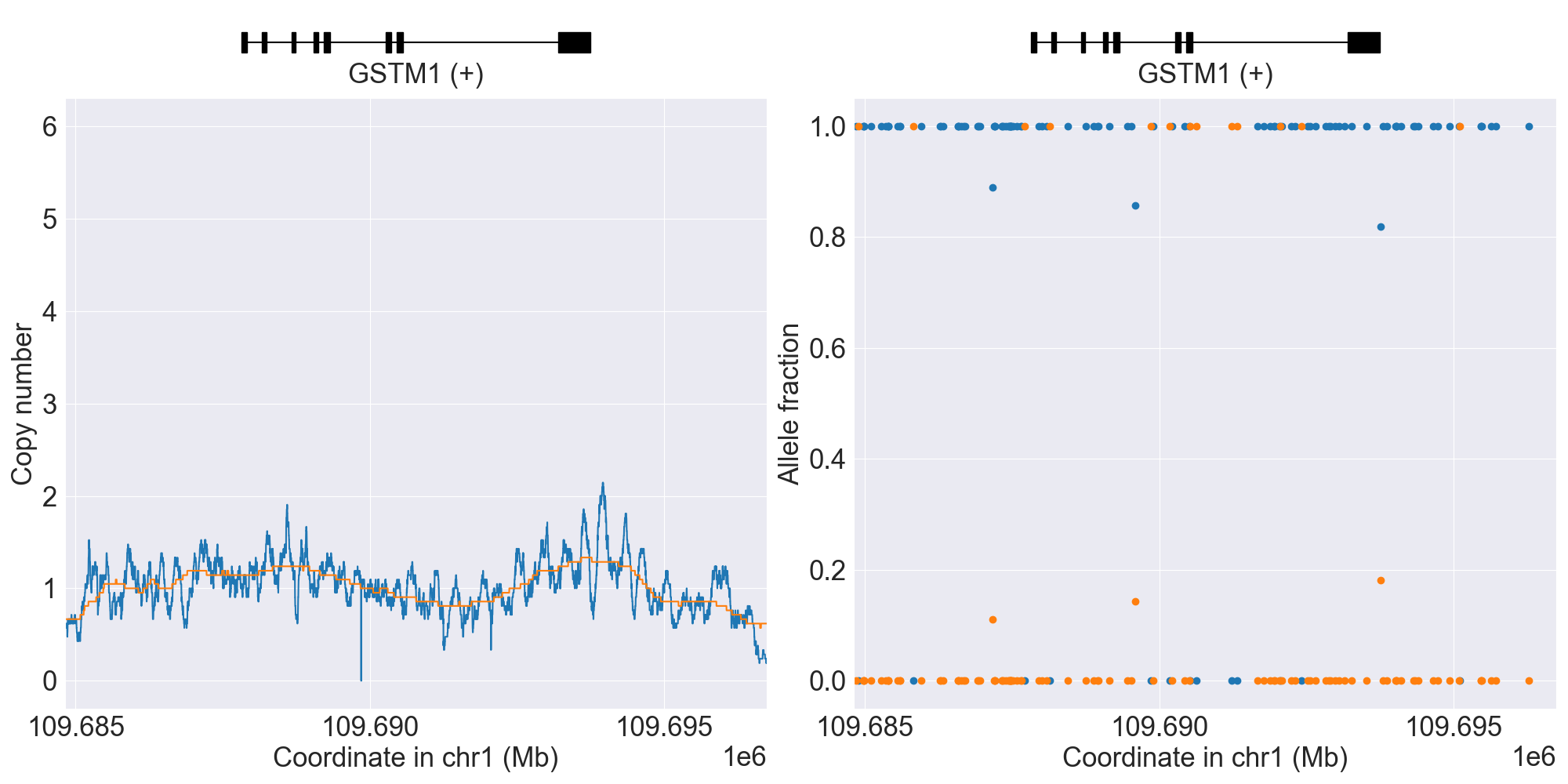
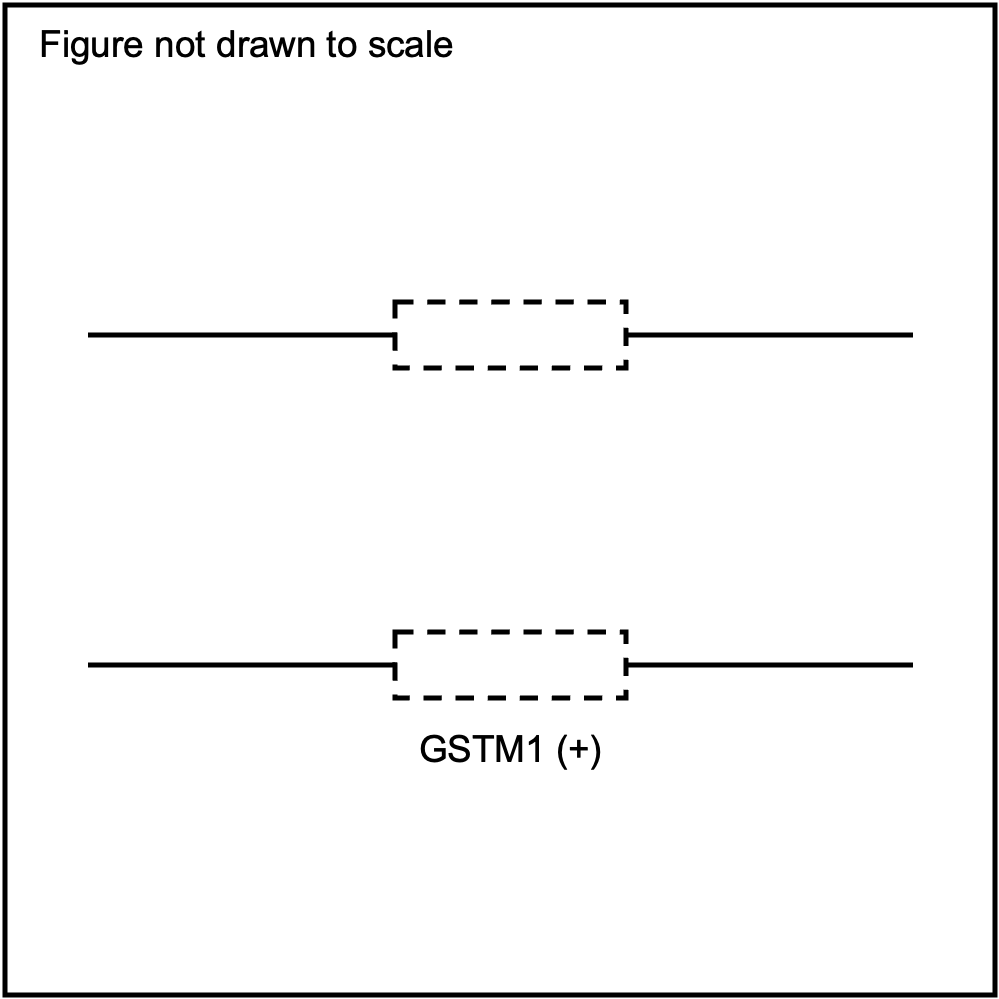
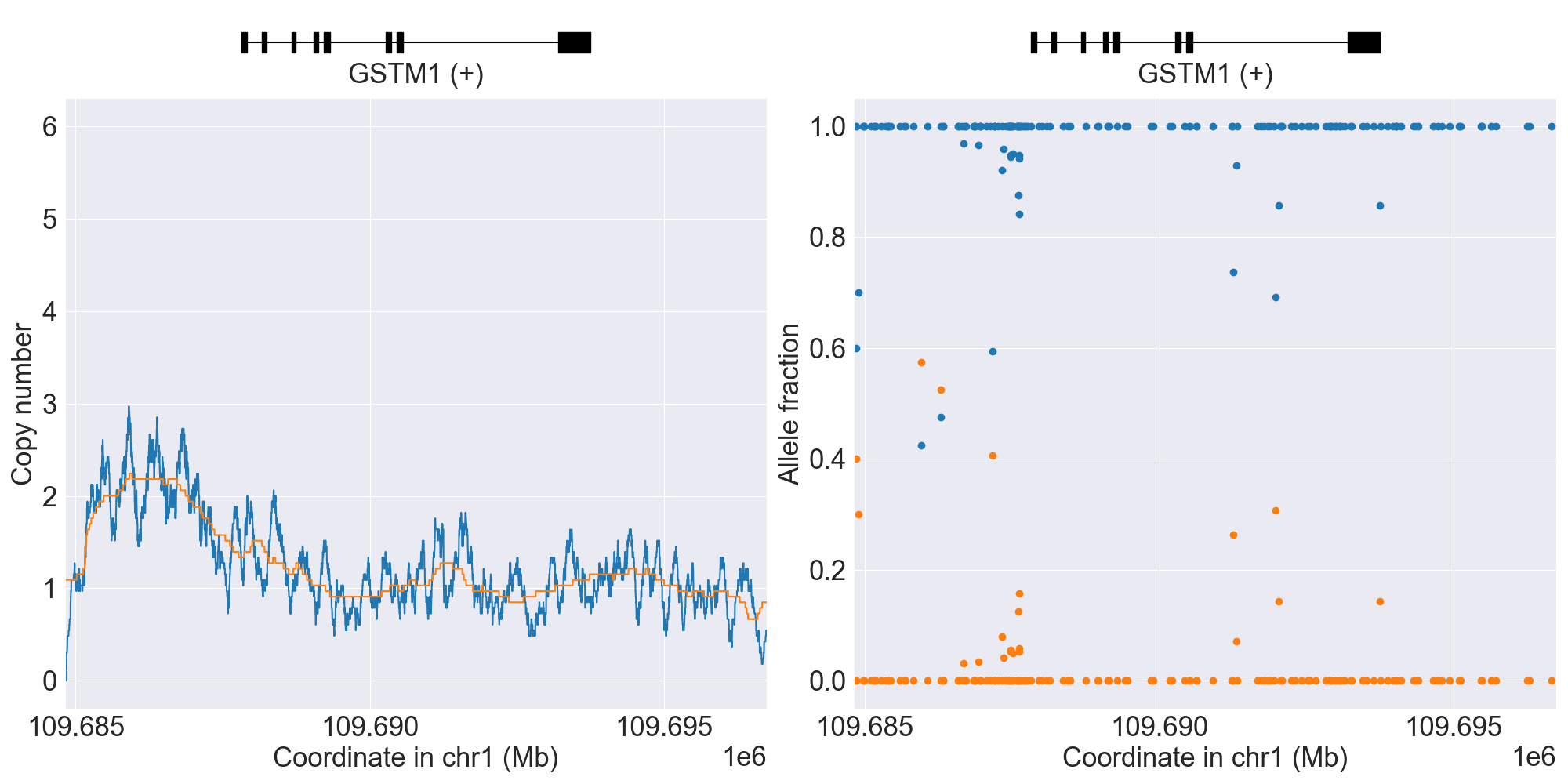
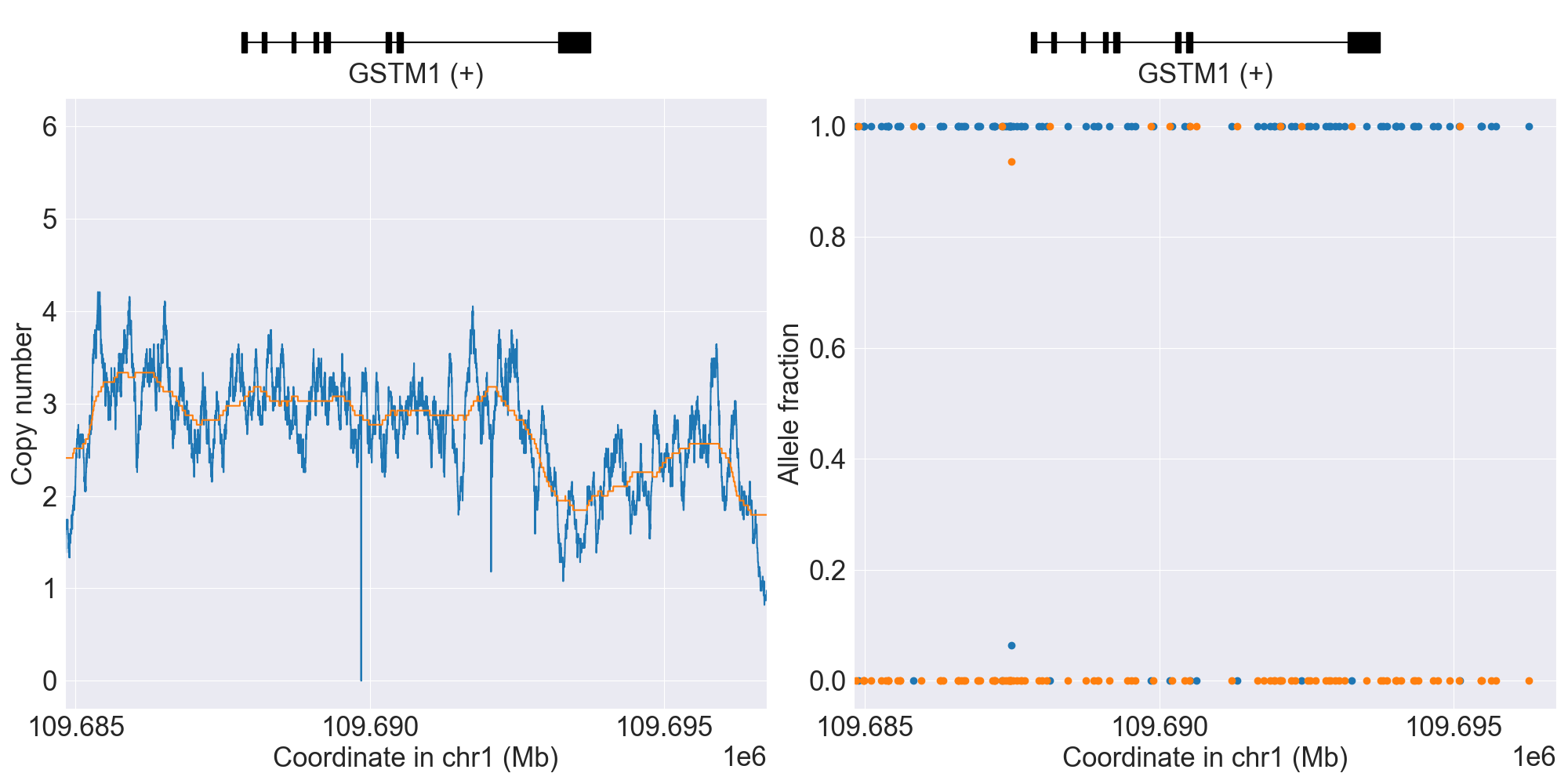
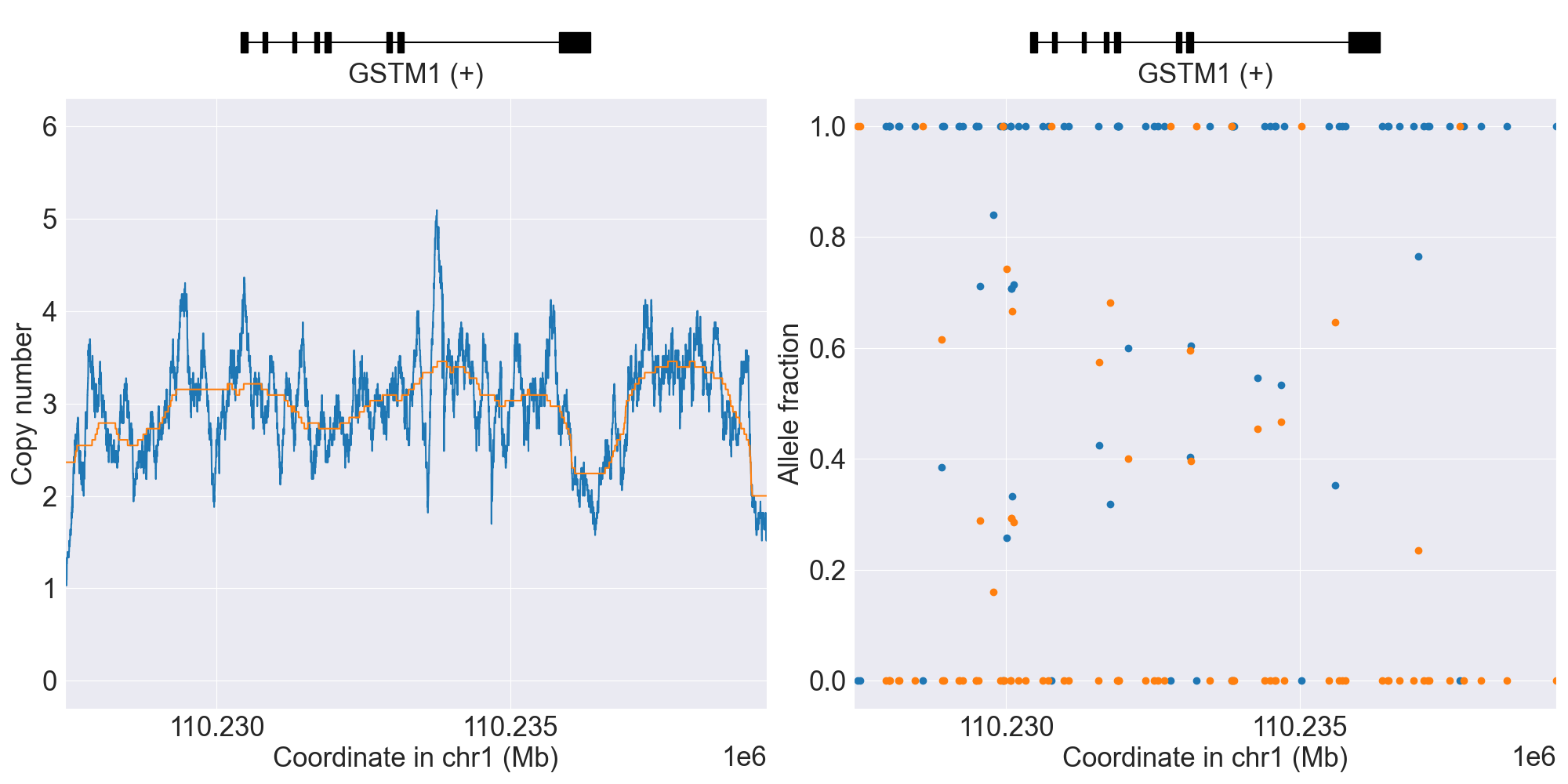
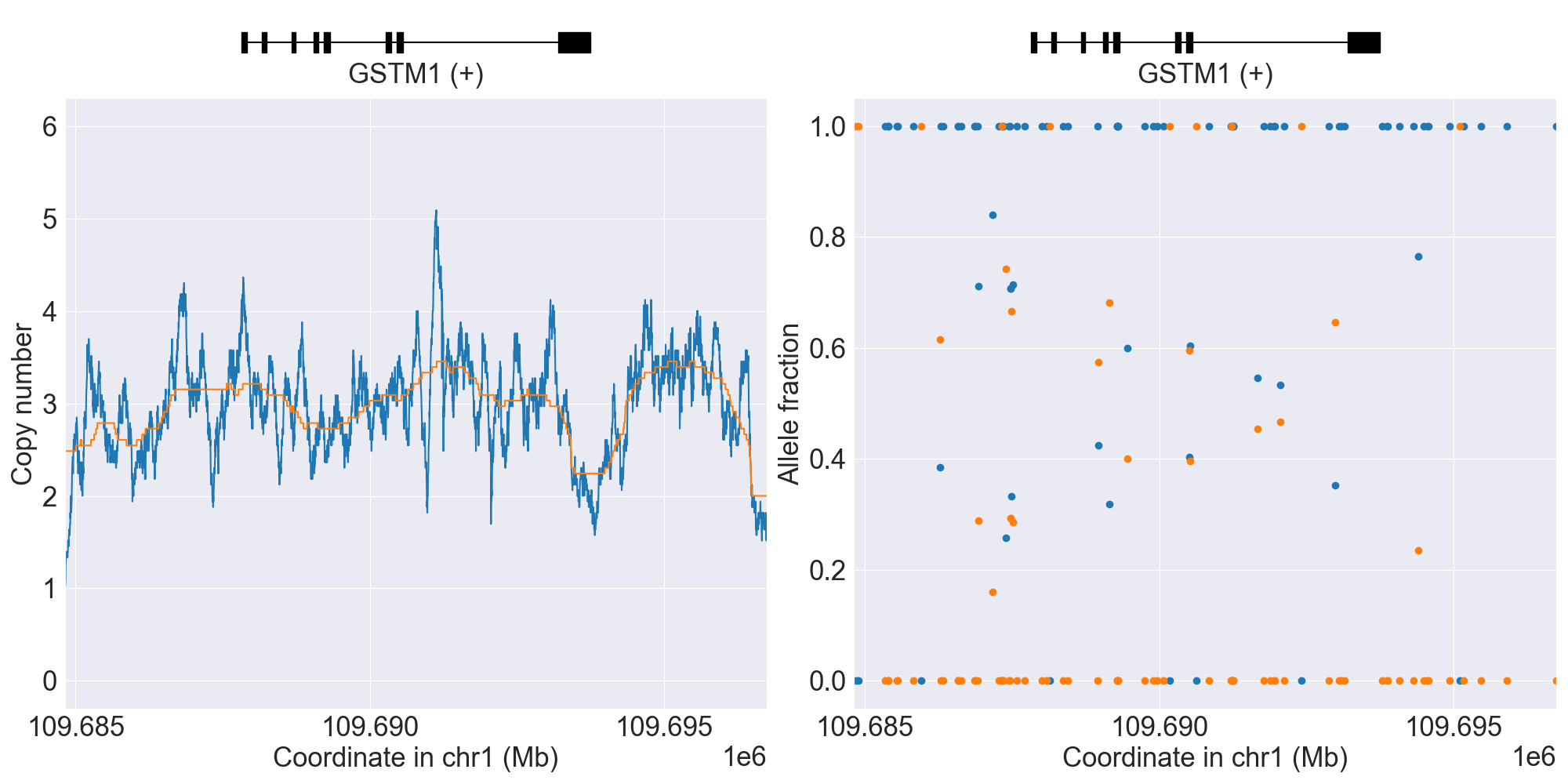
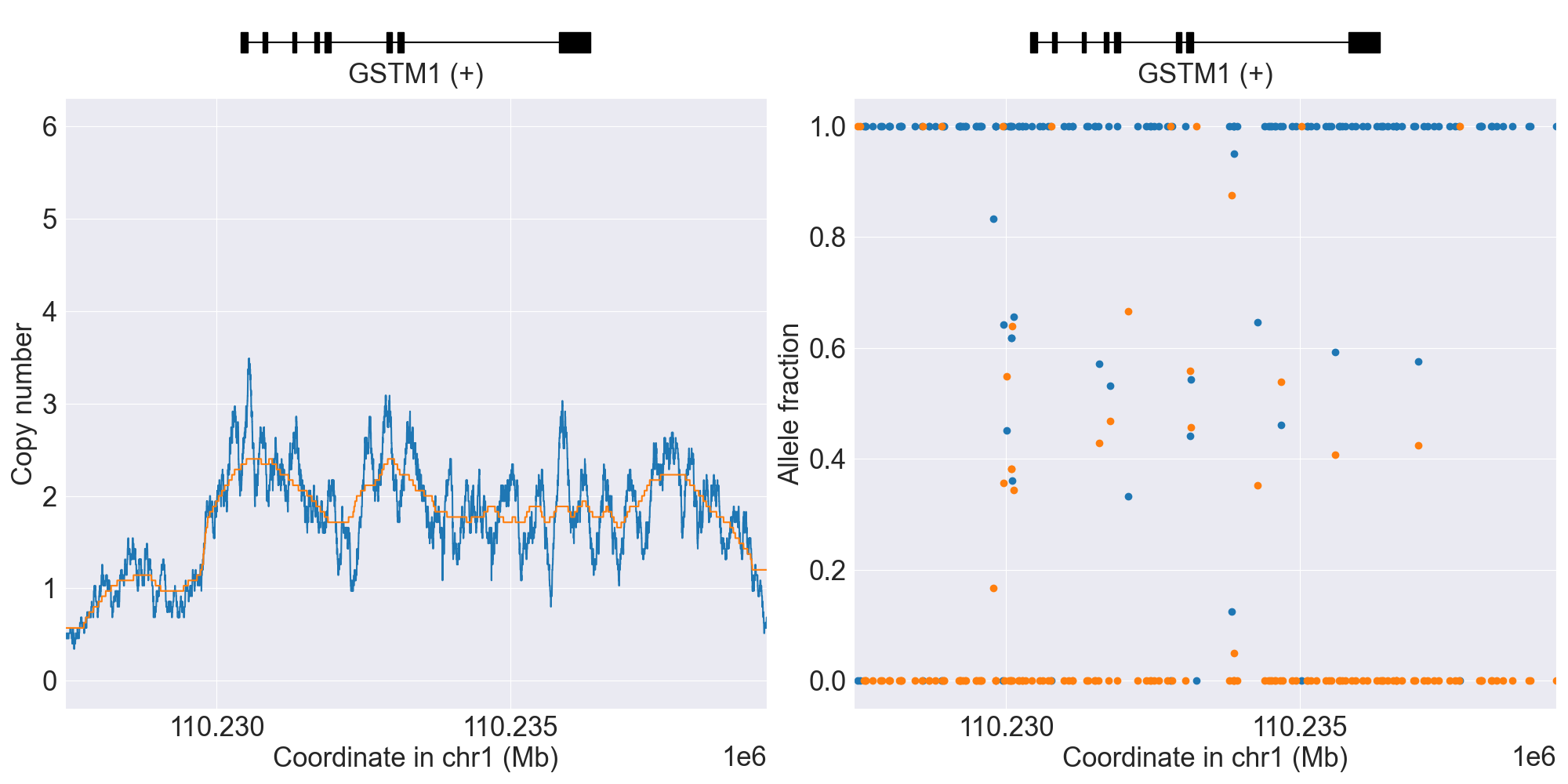
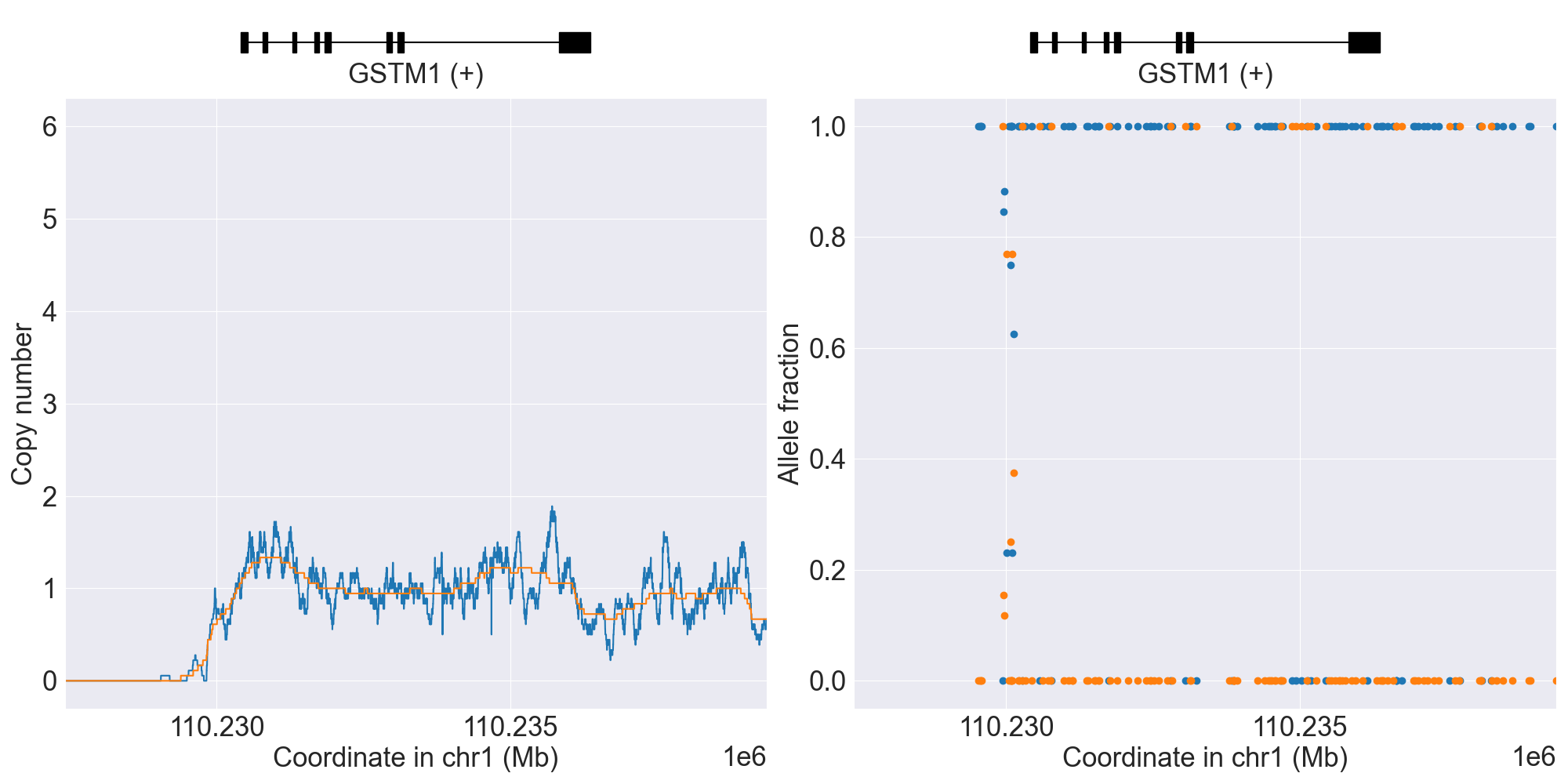
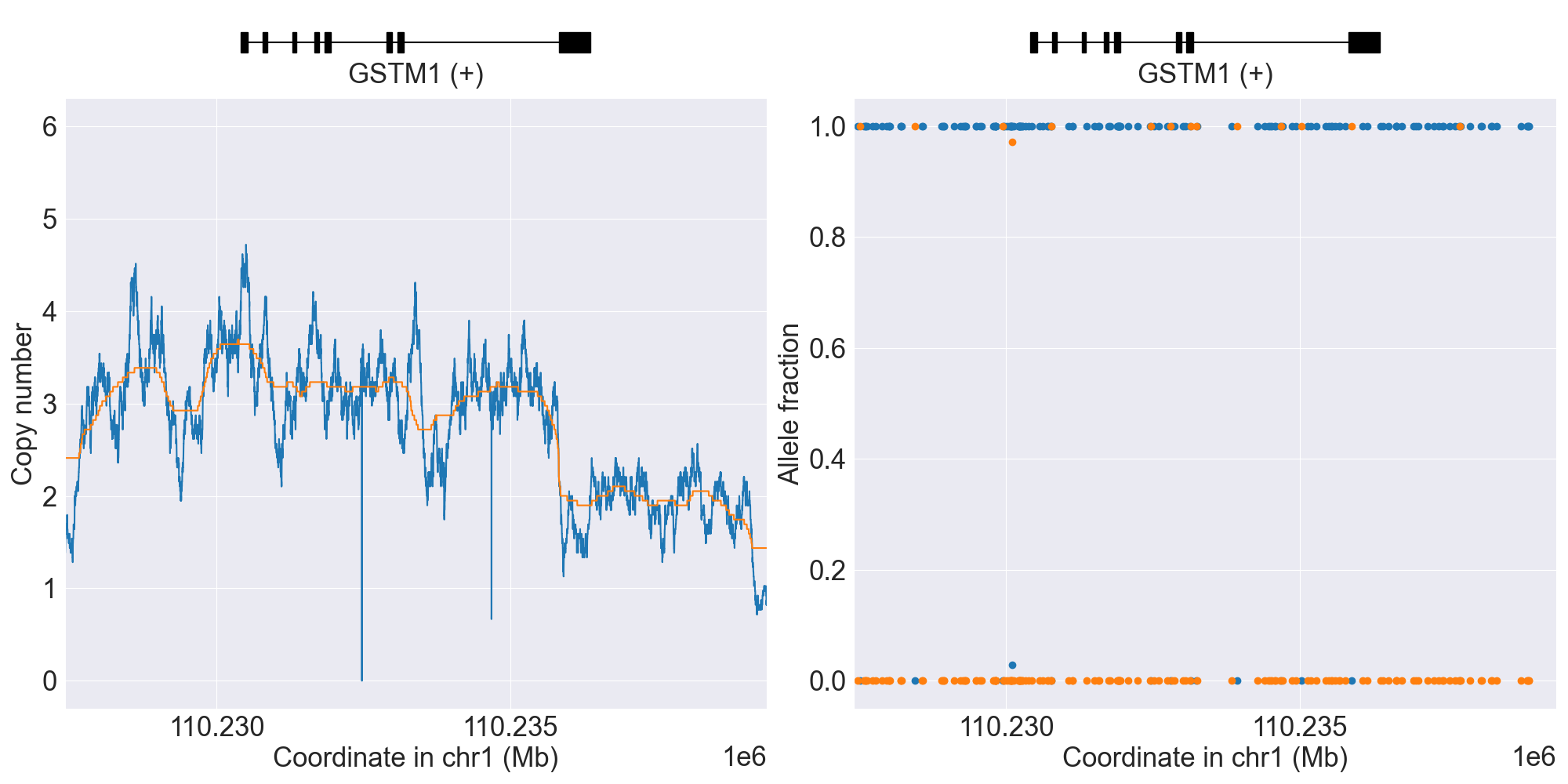
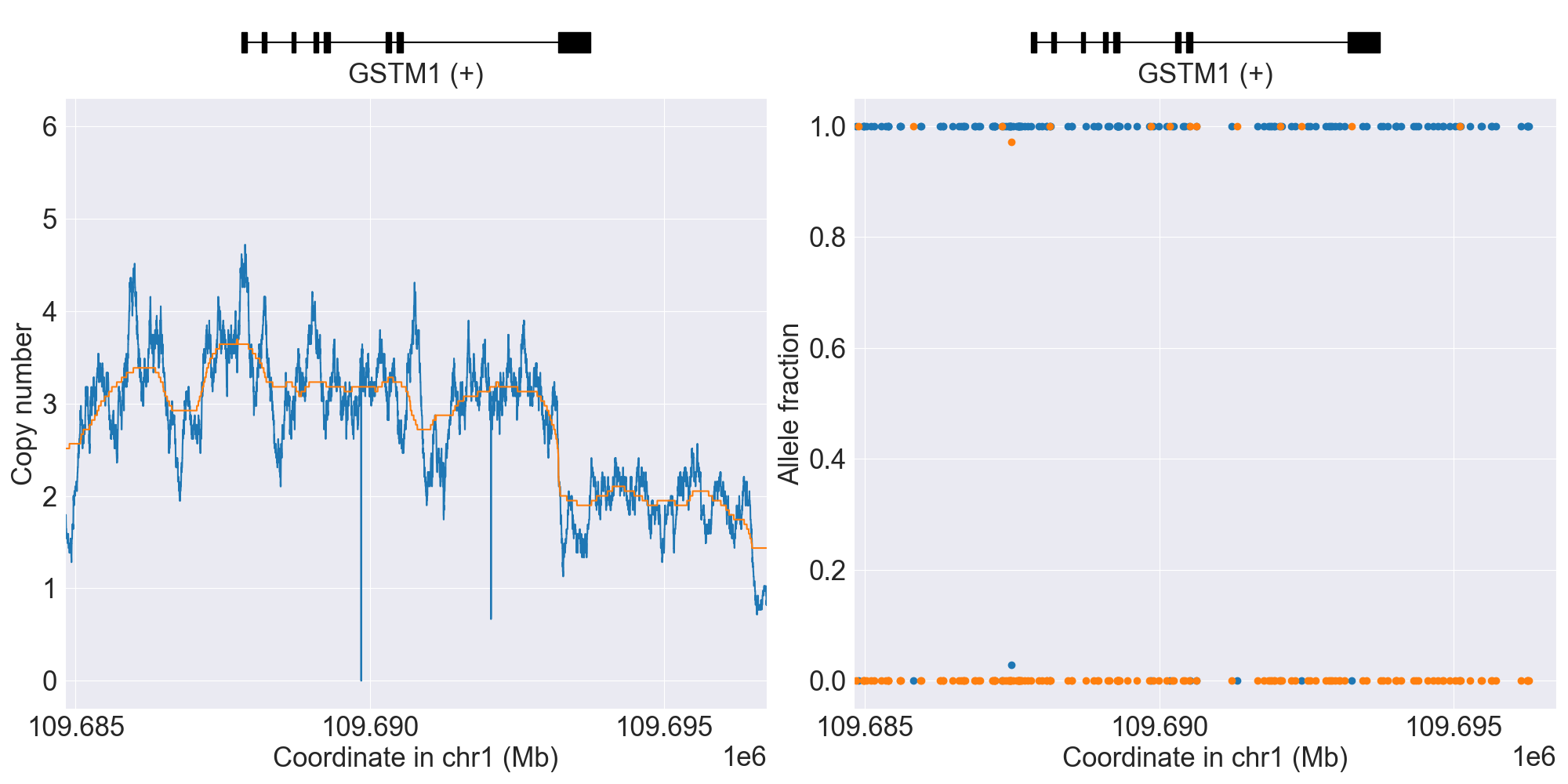
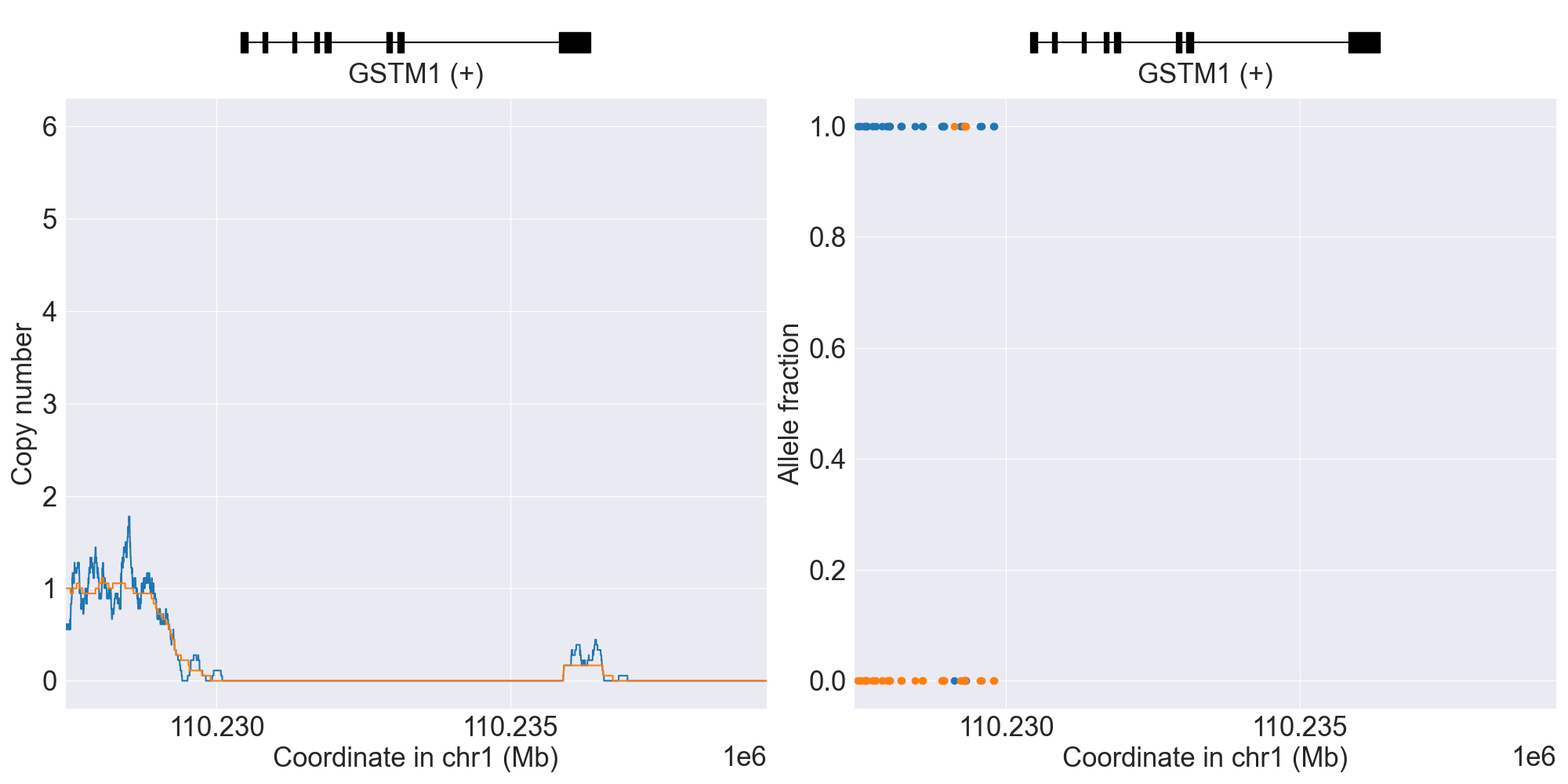
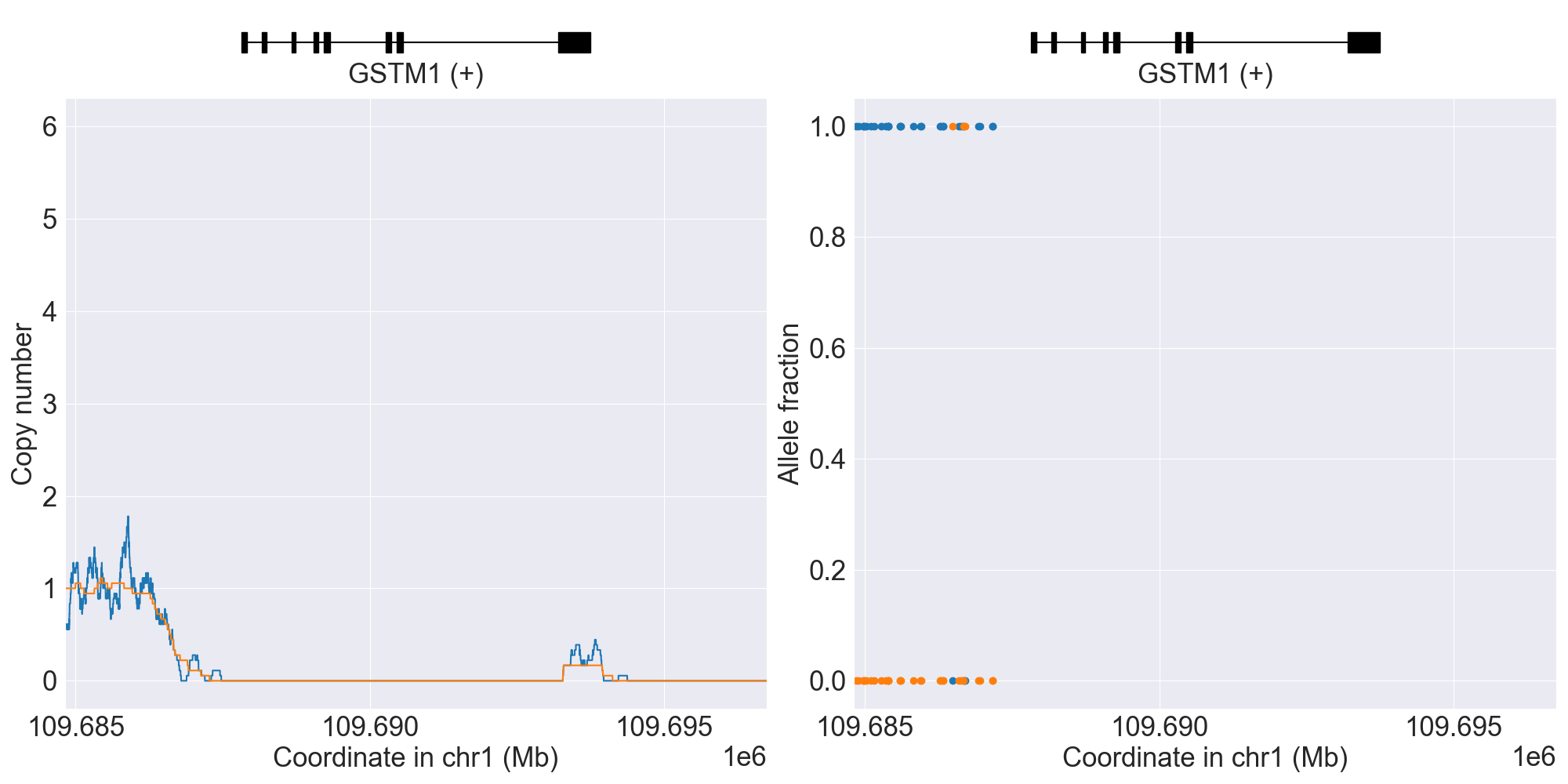
GSTM1
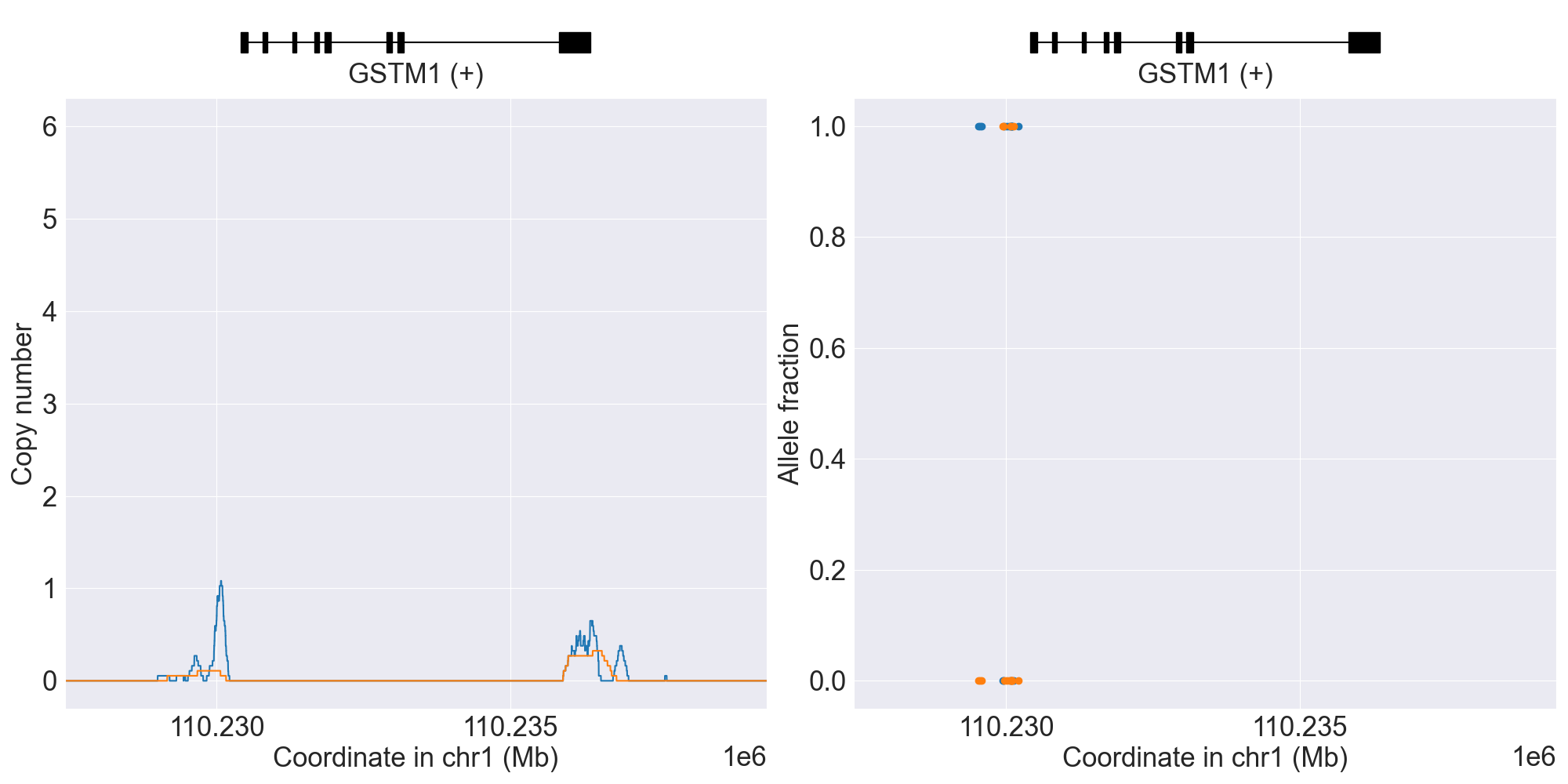
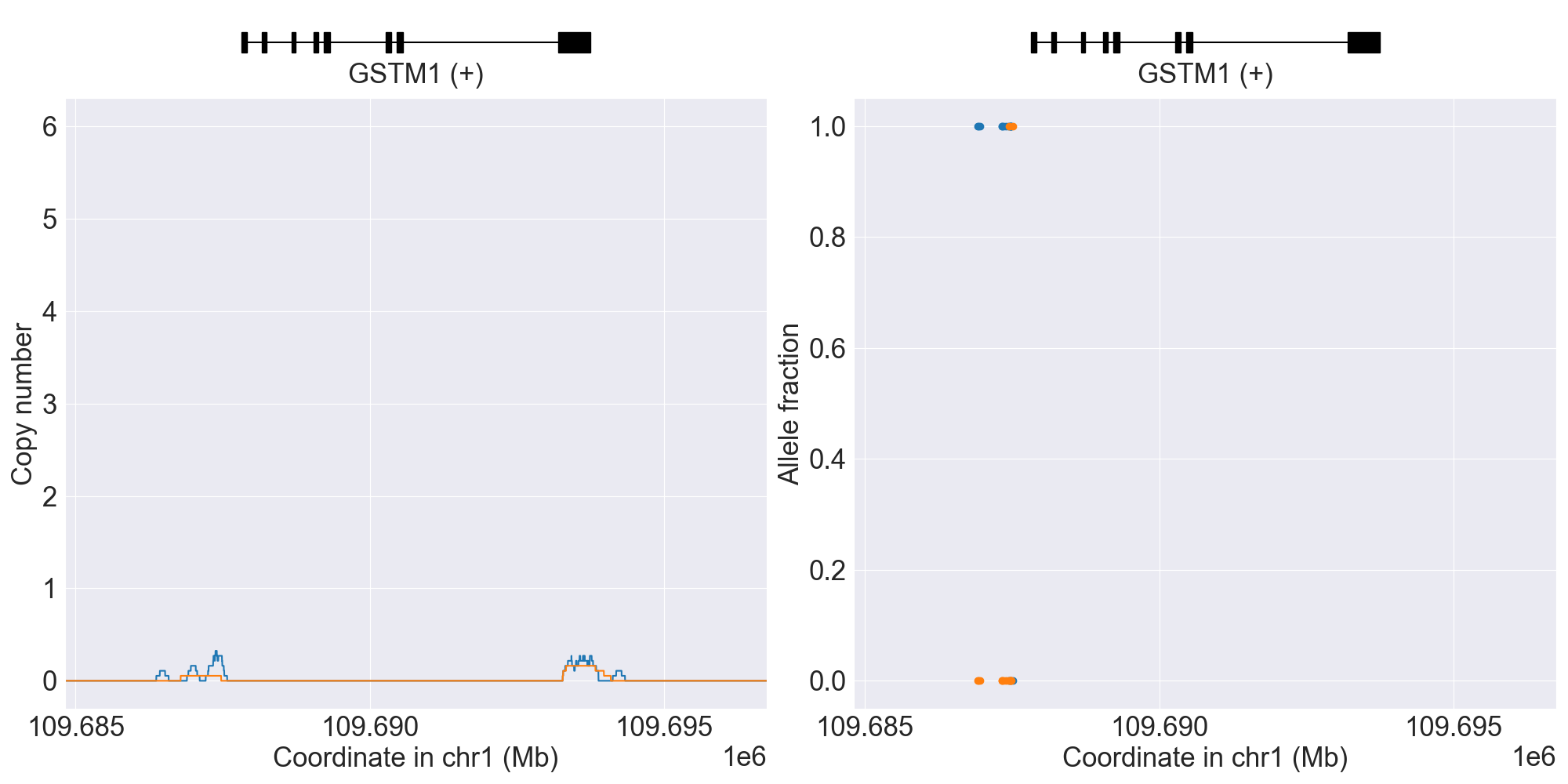
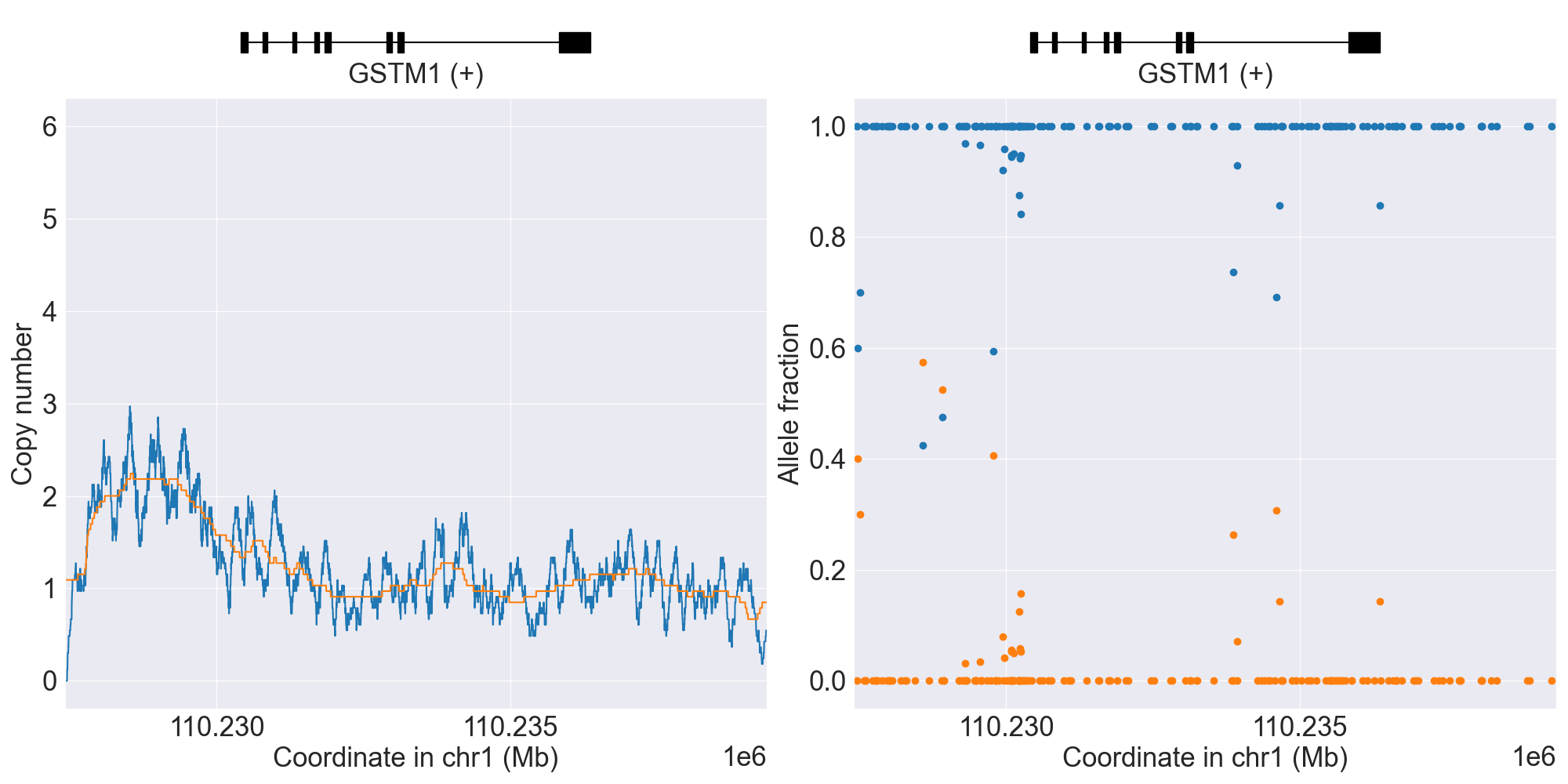
SV summary for GSTM1
This gene is known to have an extremely high rate of gene deletion polymorphism in the population and thus requires SV analysis.
Below is comprehensive summary of SV described from real NGS studies:
SV Alleles |
SV Name |
Genotype |
Reference |
Gene Model |
GRCh37 |
GRCh38 |
Data Type |
Source |
Coriell ID |
Version |
Description |
|---|---|---|---|---|---|---|---|---|---|---|---|
Normal |
*A/*B |
WGS |
NA06991 |
0.4.1 |
|||||||
*0 |
WholeDel1 |
*0/*A |
WGS |
NA18855 |
0.4.1 |
||||||
*0 |
WholeDel1Hom |
*0/*0 |
WGS |
NA10831 |
0.4.1 |
||||||
*0 |
WholeDel2 |
*0/*A |
WGS |
NA21097 |
0.15.0 |
||||||
*Ax2 |
WholeDup1 |
*A/*Ax2 |
WGS |
NA19908 |
0.4.1 |
||||||
*Bx2 |
WholeDup1 |
*A/*Bx2 |
WGS |
0.4.1 |
|||||||
NoncodingDel1 |
*A/*B |
WGS |
NA19005 |
0.12.0 |
|||||||
*0 |
WholeDel1+NoncodingDel1 |
*0/*A |
WGS |
NA06984 |
0.12.0 |
||||||
PartialDup1 |
Indeterminate |
WGS |
NA19908 |
0.14.0 |
|||||||
WholeDel1+WholeDel2 |
Indeterminate |
WGS |
NA20506 |
0.14.0 |
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
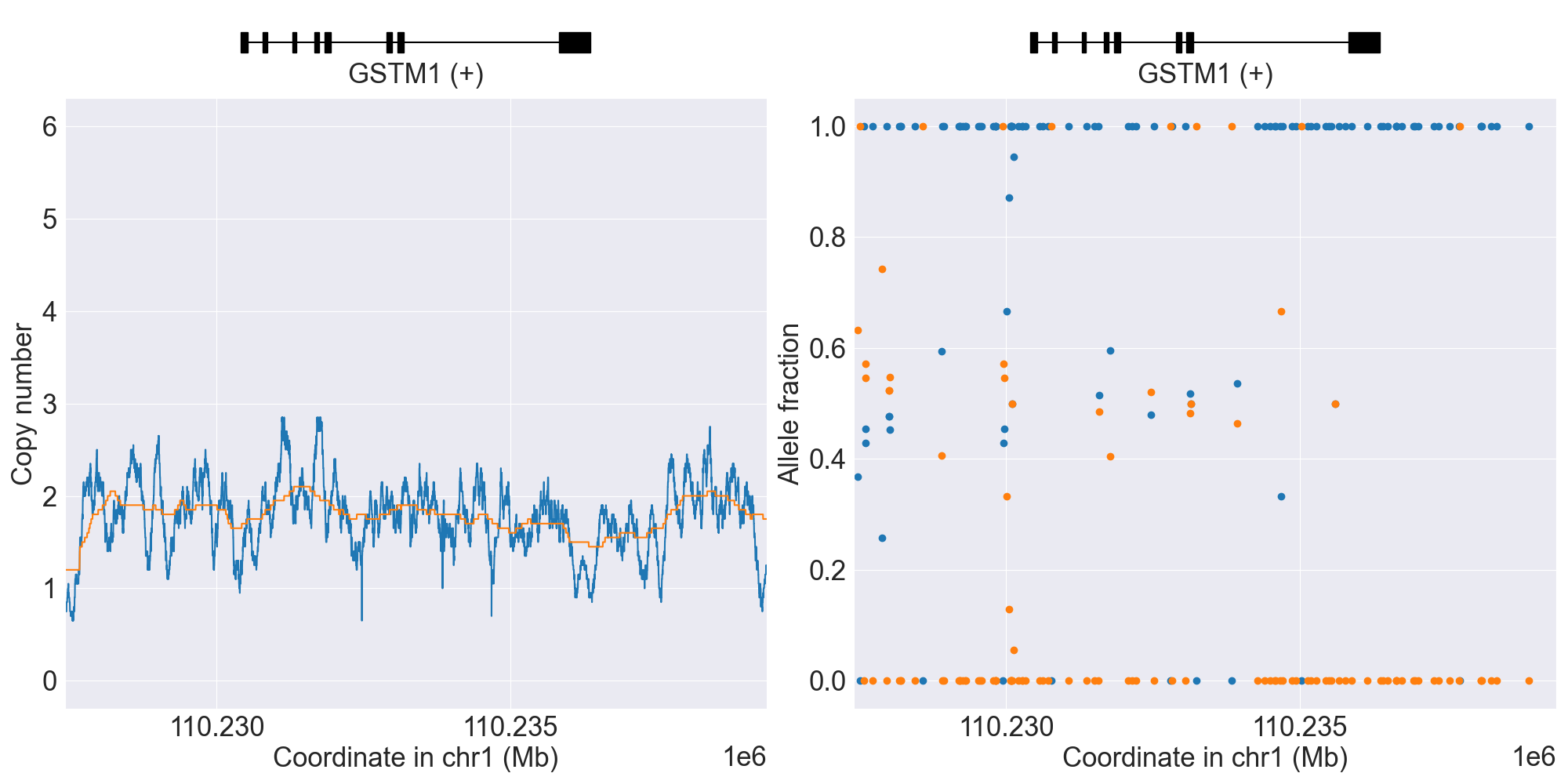
PyPGx was recently applied to the entire high-coverage WGS dataset from 1KGP (N=2,504). Click here to see individual SV calls for GSTM1, and corresponding copy number profiles and allele fraction profiles.
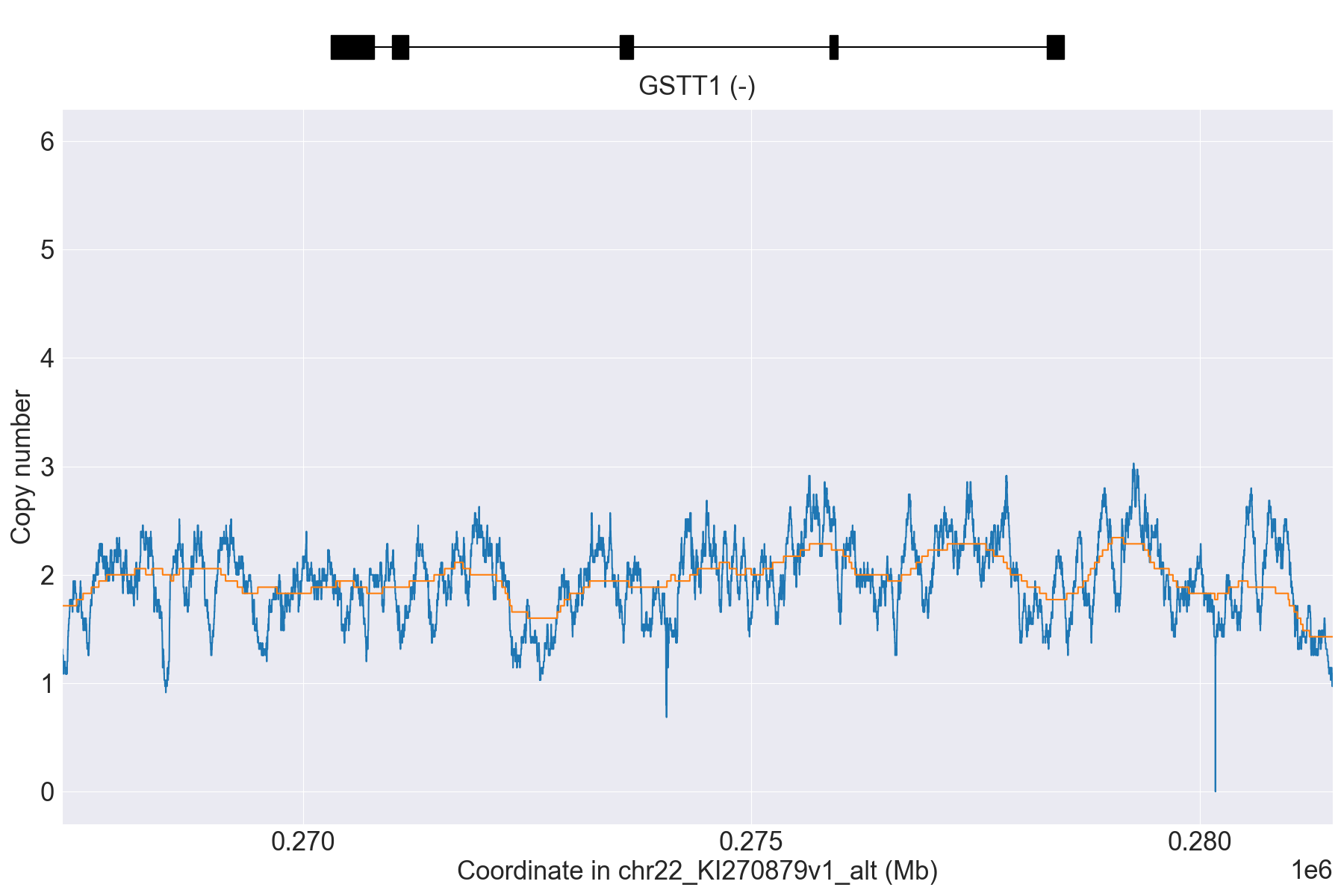
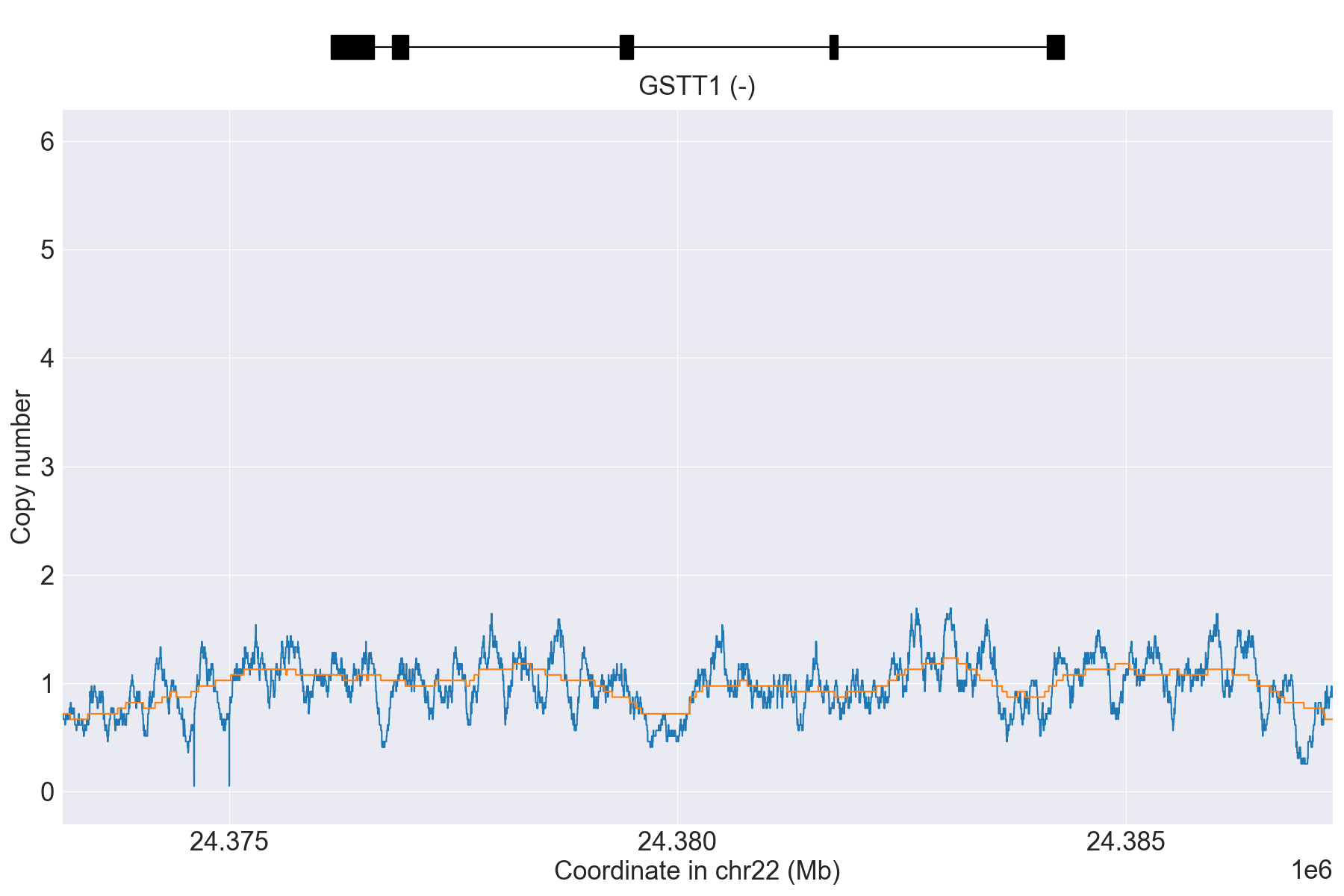
GSTT1
GRCh38 data for GSTT1
GSTT1 is located on chr22 for GRCh37 but on chr22_KI270879v1_alt
for GRCh38. Therefore, if you are interested in genotyping this gene with
GRCh38 data, then you must have sequence reads mapped to the ALT contig.
For more details, please read the GRCh37 vs. GRCh38 page.
SV summary for GSTT1
This gene is known to have an extremely high rate of gene deletion polymorphism in the population and thus requires SV analysis.
Below is comprehensive summary of SV described from real NGS studies:
SV Alleles |
SV Name |
Genotype |
Reference |
Gene Model |
GRCh37 |
GRCh38 |
Data Type |
Source |
Coriell ID |
Version |
Description |
|---|---|---|---|---|---|---|---|---|---|---|---|
Normal |
*A/*A |
WGS |
NA07055 |
0.4.1 |
|||||||
*0 |
WholeDel1 |
*0/*A |
WGS |
NA19908 |
0.4.1 |
||||||
*0 |
WholeDel1Hom |
*0/*0 |
WGS |
NA11832 |
0.4.1 |
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
IFNL3
Phenotype summary for IFNL3
Diplotype-phenotype mapping is used for phenotype prediction.
Phenotype |
Example |
Priority |
|---|---|---|
Favorable Response |
Reference/Reference |
None |
Unfavorable Response |
Reference/rs12979860 |
None |
Indeterminate |
Reference/rs8099917 |
None |
Recommendations for IFNL3
Peginterferon alfa-2a
“IFNL3 (IL28B) variation (rs12979860) is the strongest baseline predictor of response to PEG-interferon-alpha-containing regimens in HCV genotype 1 patients. Patients with the favorable response genotype (rs12979860 CC) have increased likelihood of response (higher SVR rate) to PEG-interferon-alpha- containing regimens as compared to patients with unfavorable response genotype (rs12979860 CT or TT). Consider implications before initiating PEG-IFN alpha and RBV containing regimens.” (Source: PharmGKB)
Peginterferon alfa-2b
“IFNL3 (IL28B) variation (rs12979860) is the strongest baseline predictor of response to PEG-interferon-alpha-containing regimens in HCV genotype 1 patients. Patients with the favorable response genotype (rs12979860 CC) have increased likelihood of response (higher SVR rate) to PEG-interferon-alpha- containing regimens as compared to patients with unfavorable response genotype (rs12979860 CT or TT). Consider implications before initiating PEG-IFN alpha and RBV containing regimens.” (Source: PharmGKB)
Ribavirin
“IFNL3 (IL28B) variation (rs12979860) is the strongest baseline predictor of response to PEG-interferon-alpha-containing regimens in HCV genotype 1 patients. Patients with the favorable response genotype (rs12979860 CC) have increased likelihood of response (higher SVR rate) to PEG-interferon-alpha- containing regimens as compared to patients with unfavorable response genotype (rs12979860 CT or TT). Consider implications before initiating PEG-IFN alpha and RBV containing regimens.” (Source: PharmGKB)
Resources for IFNL3
MT-RNR1
Phenotype summary for MT-RNR1
Diplotype-phenotype mapping is used for phenotype prediction.
Phenotype |
Example |
Priority |
|---|---|---|
Normal Risk of Aminoglycoside-Induced Hearing Loss |
Reference/Reference |
None |
Increased Risk of Aminoglycoside-Induced Hearing Loss |
m.1494C>T/m.1494C>T |
None |
Uncertain Risk of Aminoglycoside-Induced Hearing Loss |
m.663A>G/m.663A>G |
None |
NUDT15
Phenotype summary for NUDT15
Diplotype-phenotype mapping is used for phenotype prediction.
Phenotype |
Example |
Priority |
|---|---|---|
Normal Metabolizer |
*1/*1 |
Normal/Routine/Low risk |
Intermediate Metabolizer |
*1/*2 |
Abnormal/Priority/High Risk |
Possible Intermediate Metabolizer |
*3/*4 |
Abnormal/Priority/High Risk |
Poor Metabolizer |
*2/*3 |
Abnormal/Priority/High Risk |
Indeterminate |
*1/*4 |
Abnormal/Priority/High Risk |
Recommendations for NUDT15
Azathioprine
“Consider an alternate agent or extreme dose reduction of azathioprine for patients who are TPMT or NUDT15 poor metabolizers. Start at 30-80% of target dose for patients who are TPMT or NUDT15 intermediate metabolizers.” (Source: PharmGKB)
Mercaptopurine
“Consider an alternate agent or extreme dose reduction of mercaptopurine for patients who are TPMT or NUDT15 poor metabolizers. Start at 30-80% of target dose for patients who are TPMT or NUDT15 intermediate metabolizers.” (Source: PharmGKB)
Thioguanine
“Consider an alternate agent or extreme dose reduction of thioguanine for patients who are TPMT or NUDT15 poor metabolizers. Start at 50-80% of target dose for patients who are TPMT or NUDT15 intermediate metabolizers.” (Source: PharmGKB)
Resources for NUDT15
POR
Resources for POR
PTGIS
Resources for PTGIS
RYR1
Phenotype summary for RYR1
Diplotype-phenotype mapping is used for phenotype prediction.
Phenotype |
Example |
Priority |
|---|---|---|
Uncertain Susceptibility |
Reference/Reference |
Normal Risk |
Malignant Hyperthermia Susceptibility |
Reference/c.103T>C |
Abnormal/Priority/High Risk |
Recommendations for RYR1
Desflurane
“The CPIC Dosing Guideline recommends that halogenated volatile anesthetics uch as desflurane, enflurane, halothane, isoflurane, methoxyflurane, sevoflurane and the depolarizing muscle relaxants succinylcholine are relatively contraindicated in persons with malignant hyperthermia susceptibility (MHS). See full guideline for disclaimers, further details and supporting evidence.” (Source: PharmGKB)
Enflurane
“The CPIC Dosing Guideline recommends that halogenated volatile anesthetics such as desflurane, enflurane, halothane, isoflurane, methoxyflurane, sevoflurane and the depolarizing muscle relaxants succinylcholine are relatively contraindicated in persons with malignant hyperthermia susceptibility (MHS). See full guideline for disclaimers, further details and supporting evidence.” (Source: PharmGKB)
Halothane
“The CPIC Dosing Guideline recommends that halogenated volatile anesthetics such as desflurane, enflurane, halothane, isoflurane, methoxyflurane, sevoflurane and the depolarizing muscle relaxants succinylcholine are relatively contraindicated in persons with malignant hyperthermia susceptibility (MHS). See full guideline for disclaimers, further details and supporting evidence.” (Source: PharmGKB)
Isoflurane
“The CPIC Dosing Guideline recommends that halogenated volatile anesthetics such as desflurane, enflurane, halothane, isoflurane, methoxyflurane, sevoflurane and the depolarizing muscle relaxants succinylcholine are relatively contraindicated in persons with malignant hyperthermia susceptibility (MHS). See full guideline for disclaimers, further details and supporting evidence.” (Source: PharmGKB)
Methoxyflurane
“The CPIC Dosing Guideline recommends that halogenated volatile anesthetics such as desflurane, enflurane, halothane, isoflurane, methoxyflurane, sevoflurane and the depolarizing muscle relaxants succinylcholine are relatively contraindicated in persons with malignant hyperthermia susceptibility (MHS). See full guideline for disclaimers, further details and supporting evidence.” (Source: PharmGKB)
Sevoflurane
“The CPIC Dosing Guideline recommends that halogenated volatile anesthetics such as desflurane, enflurane, halothane, isoflurane, methoxyflurane, sevoflurane and the depolarizing muscle relaxants succinylcholine are relatively contraindicated in persons with malignant hyperthermia susceptibility (MHS). See full guideline for disclaimers, further details and supporting evidence.” (Source: PharmGKB)
Succinylcholine
“The CPIC Dosing Guideline recommends that halogenated volatile anesthetics such as desflurane, enflurane, halothane, isoflurane, methoxyflurane, sevoflurane and the depolarizing muscle relaxants succinylcholine are relatively contraindicated in persons with malignant hyperthermia susceptibility (MHS). See full guideline for disclaimers, further details and supporting evidence.” (Source: PharmGKB)
Resources for RYR1
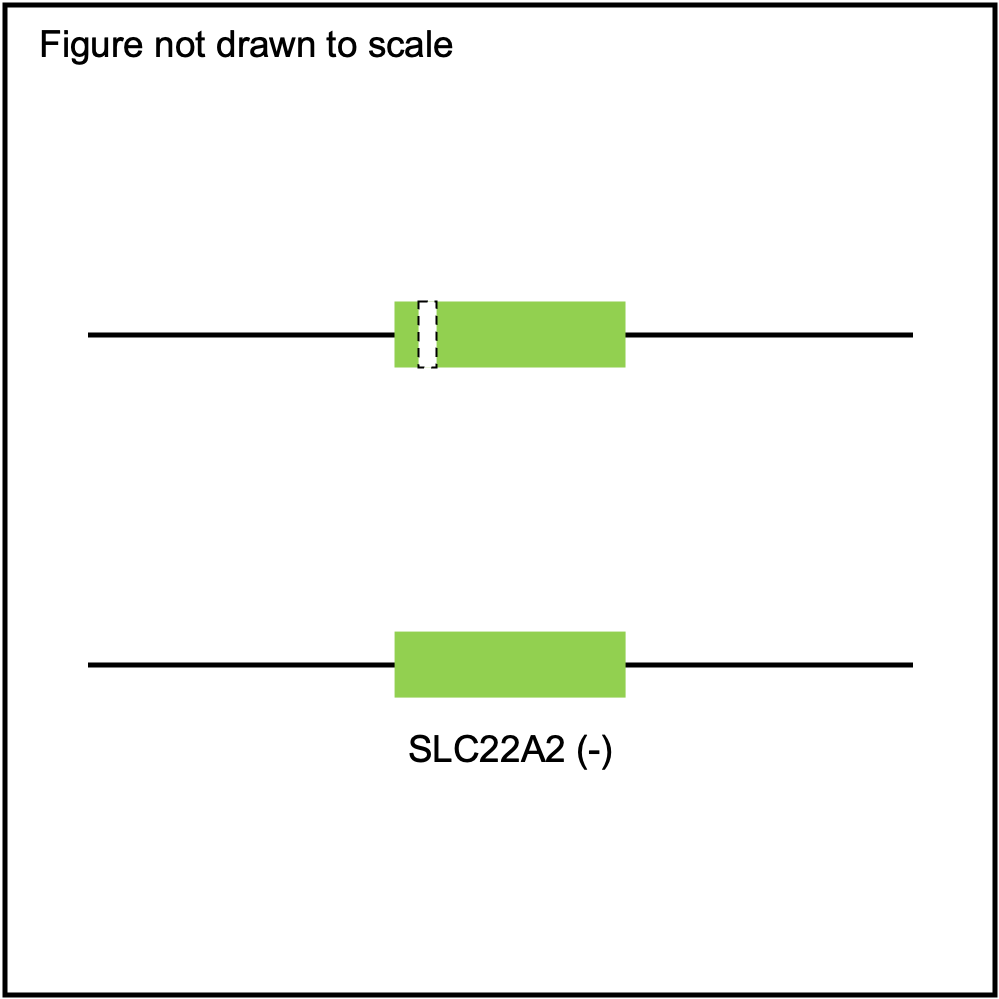
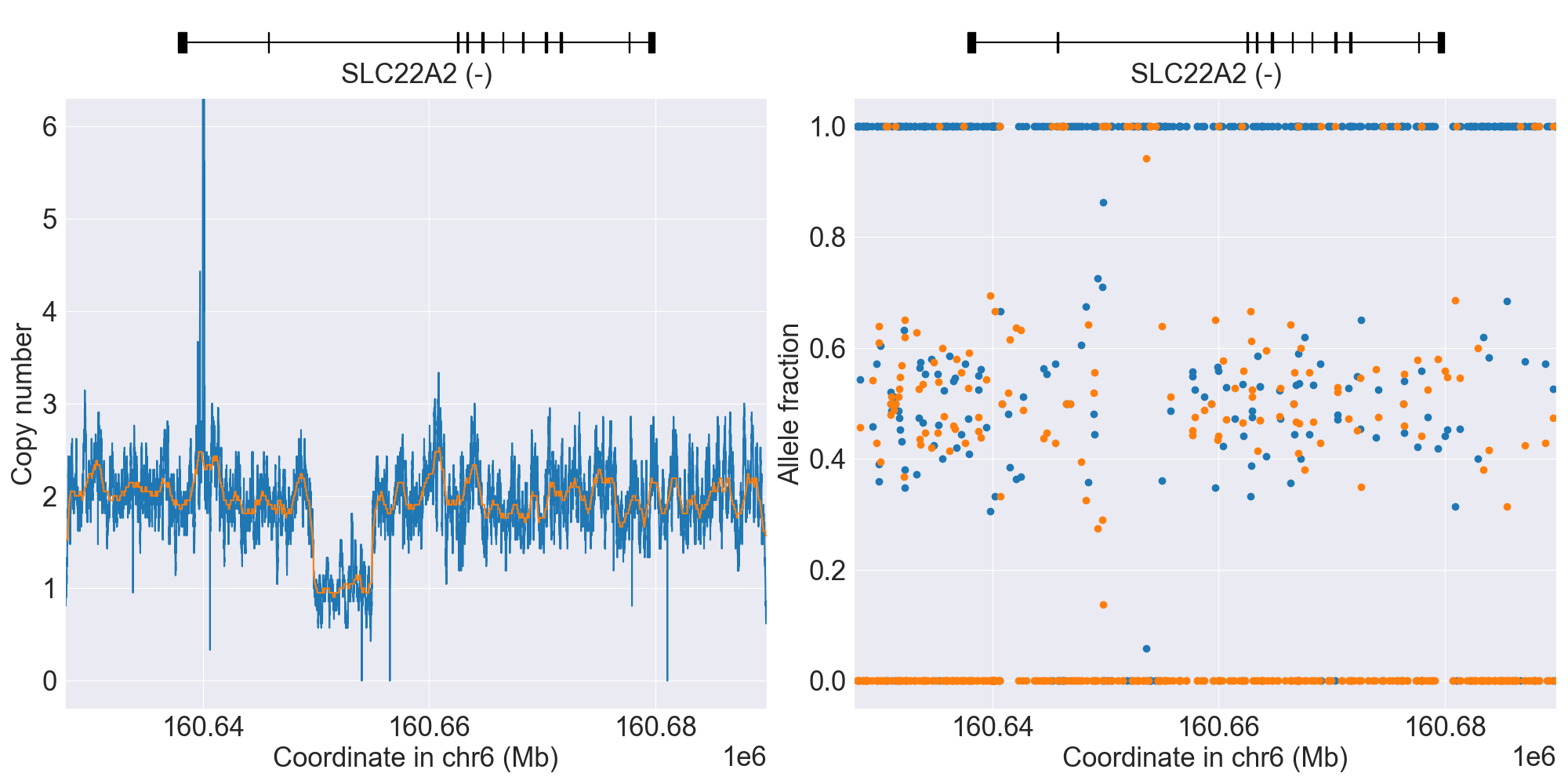
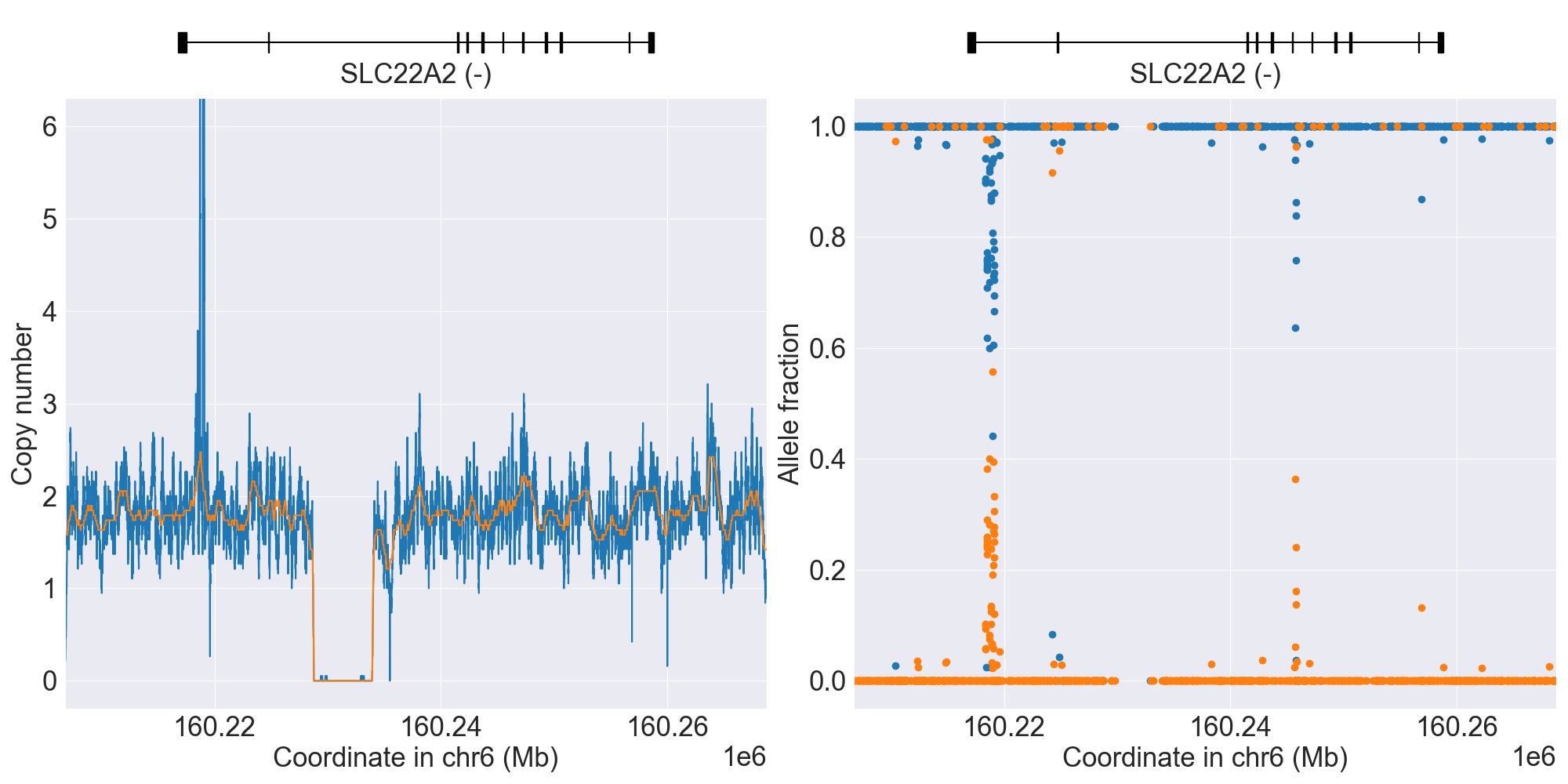
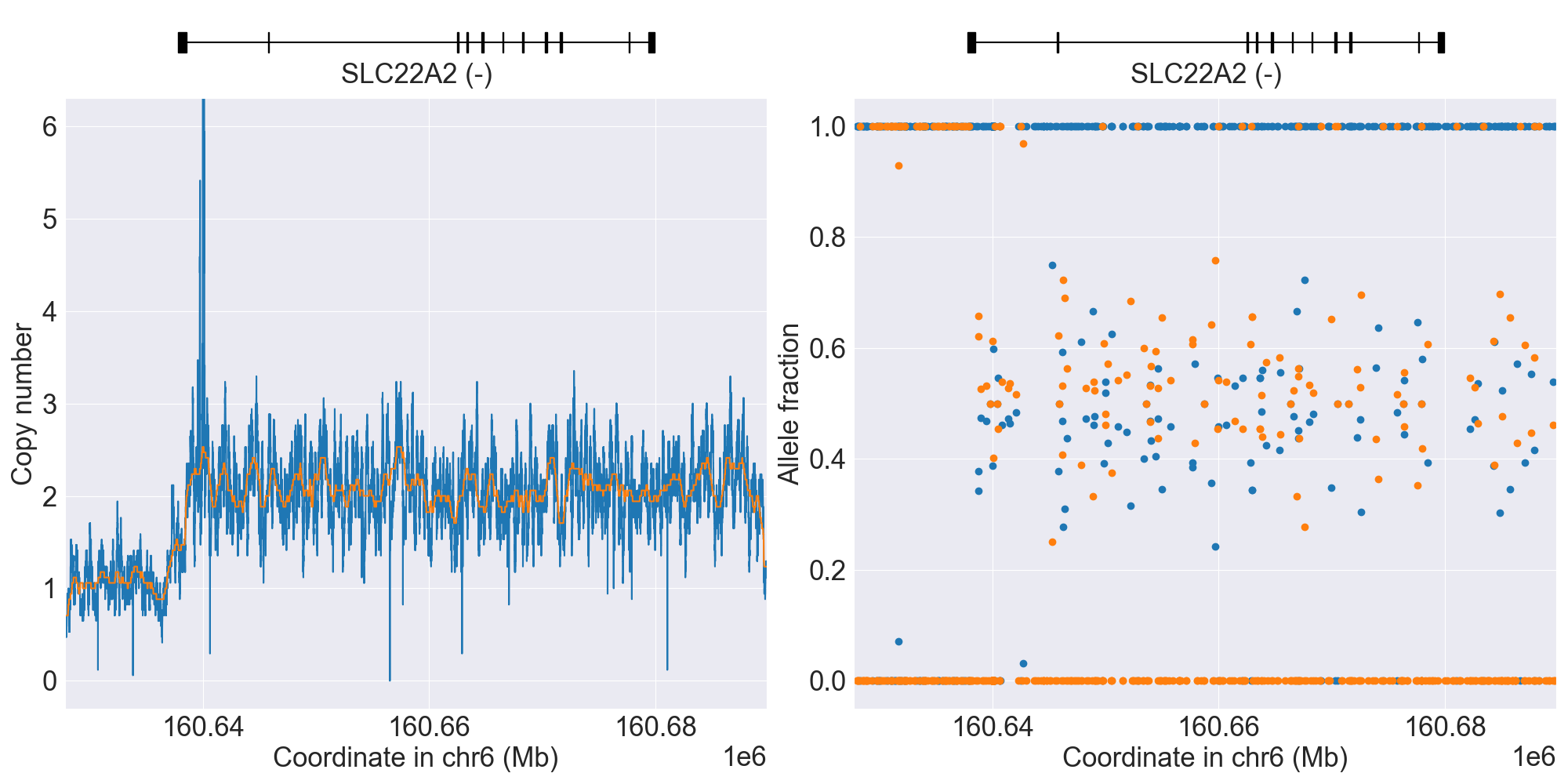
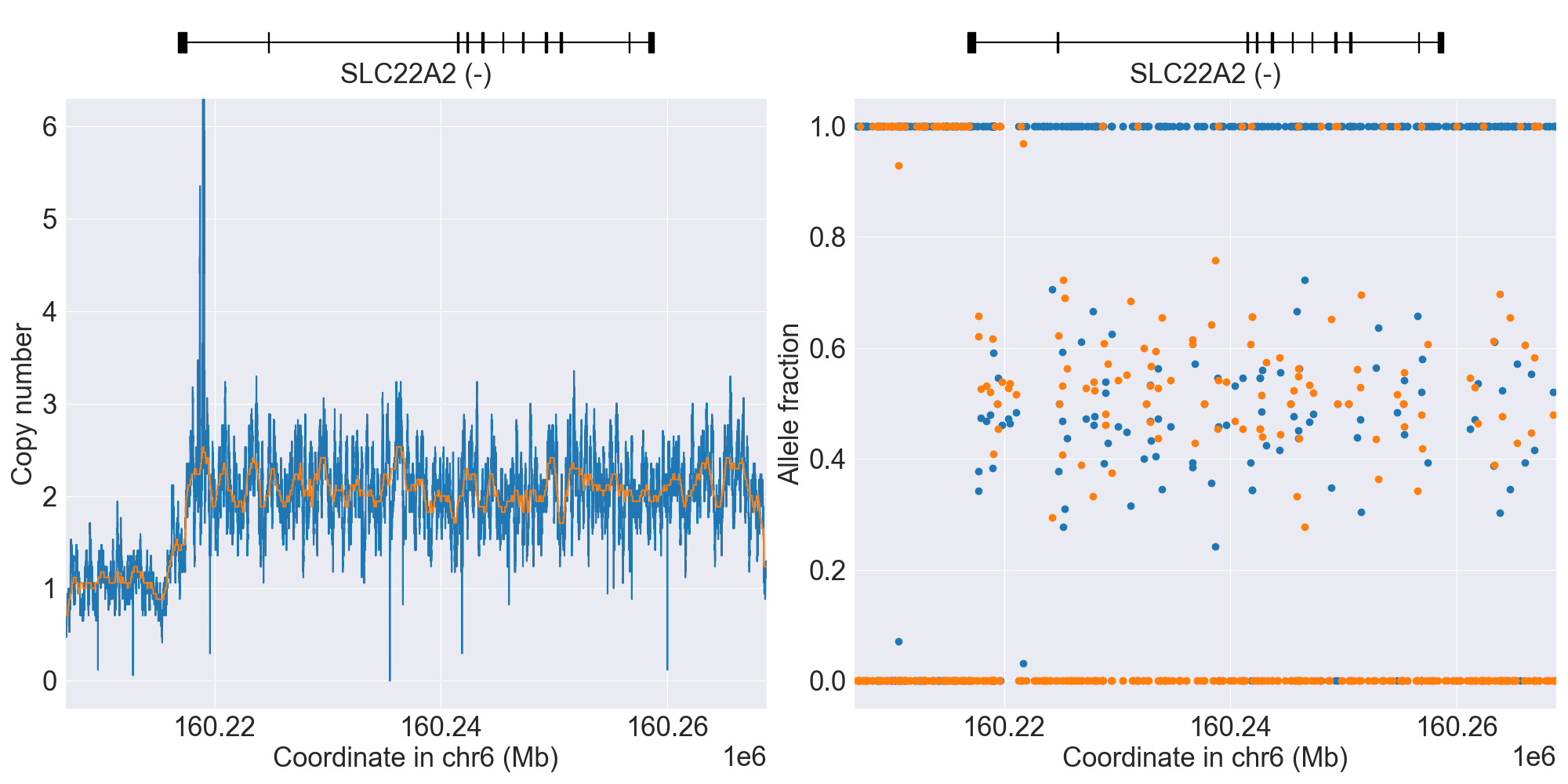
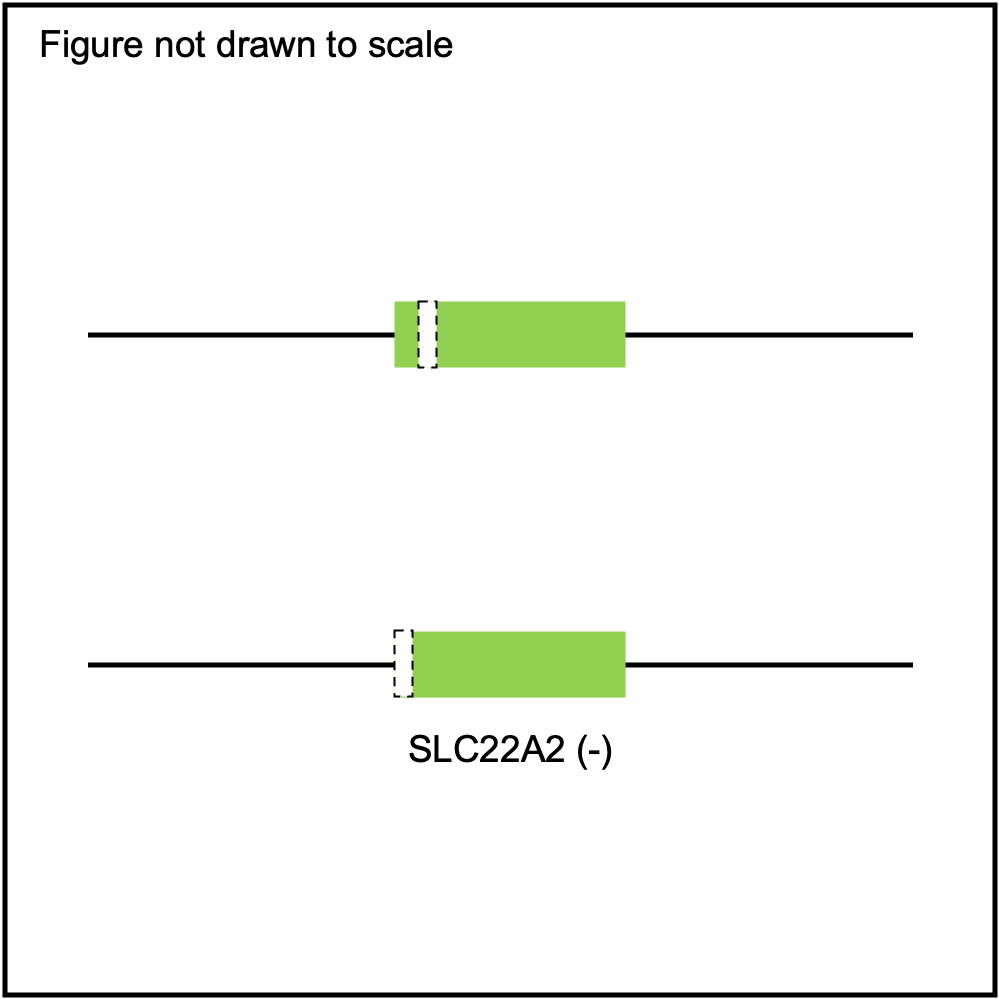
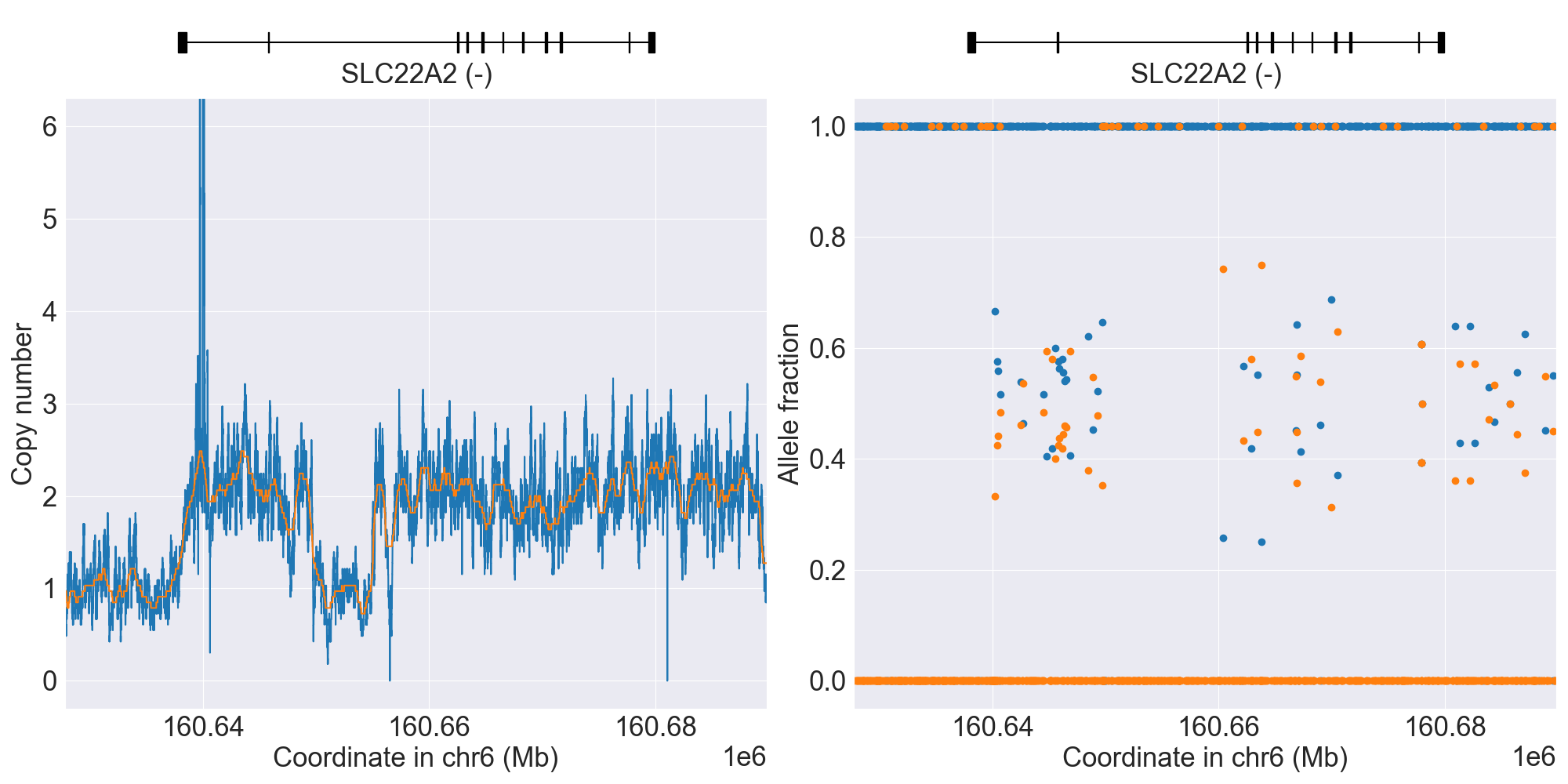
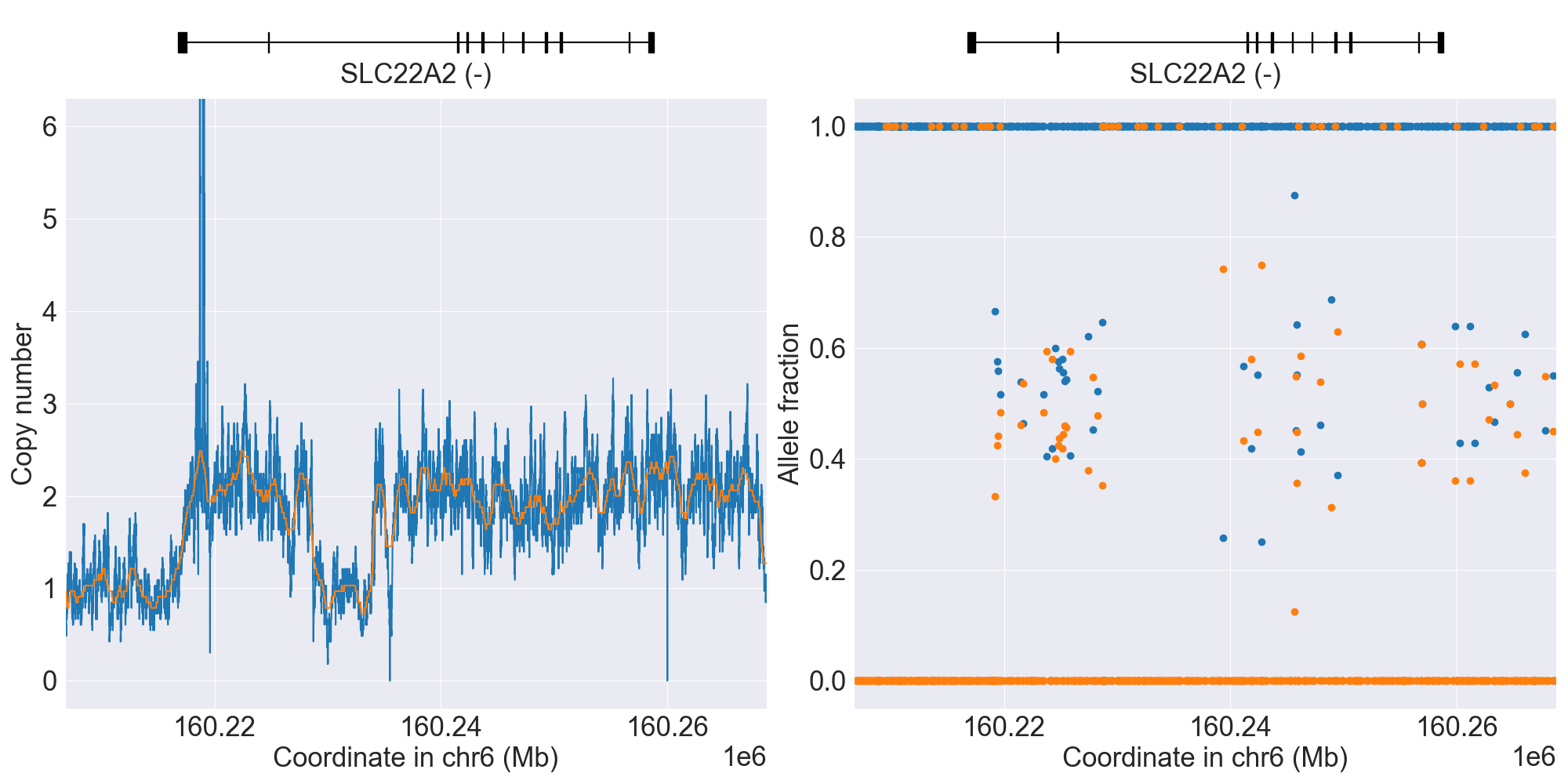
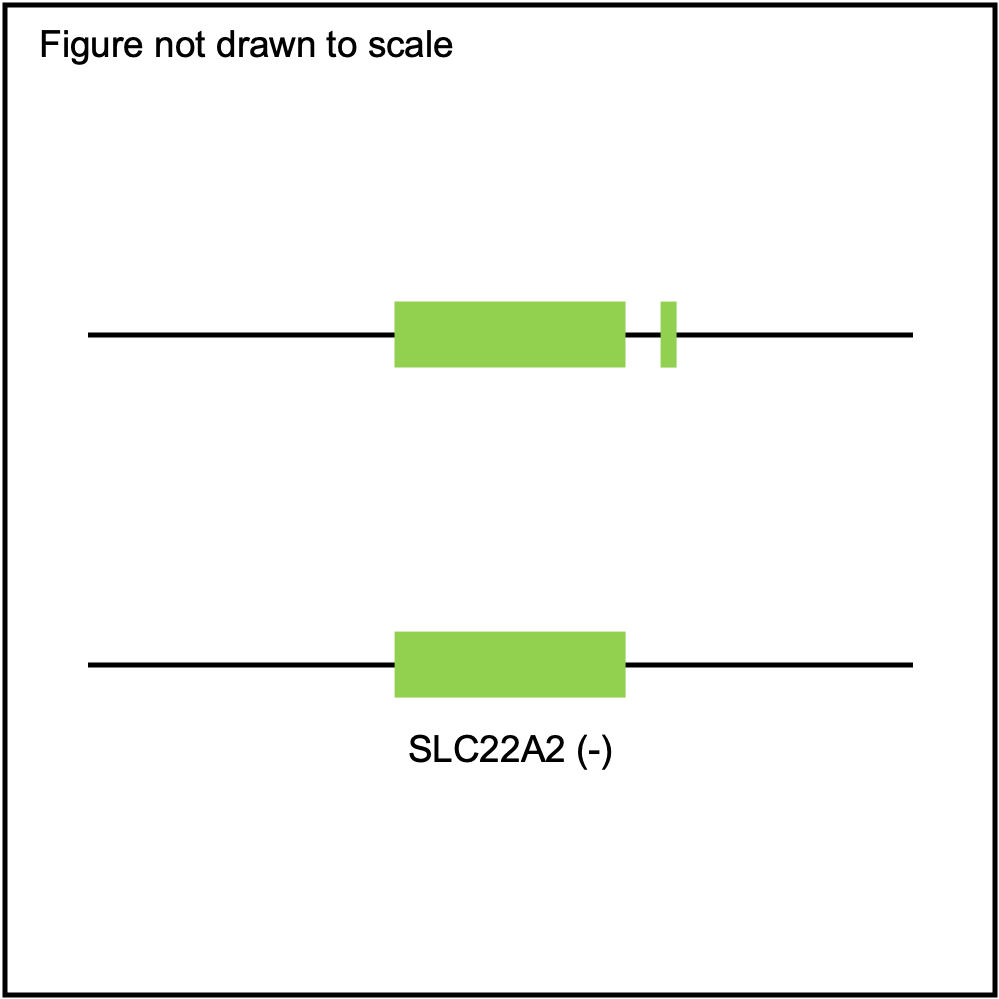
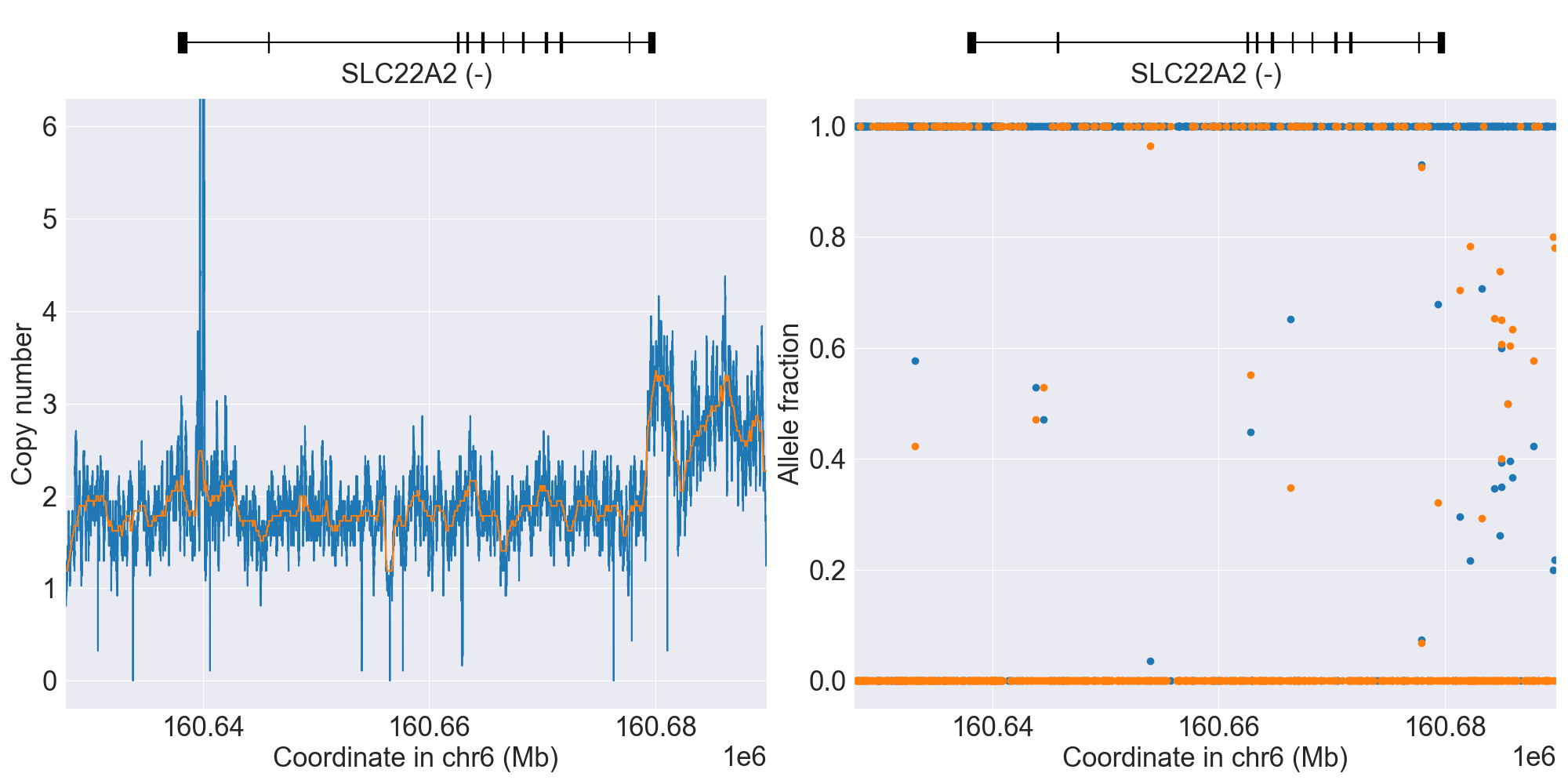
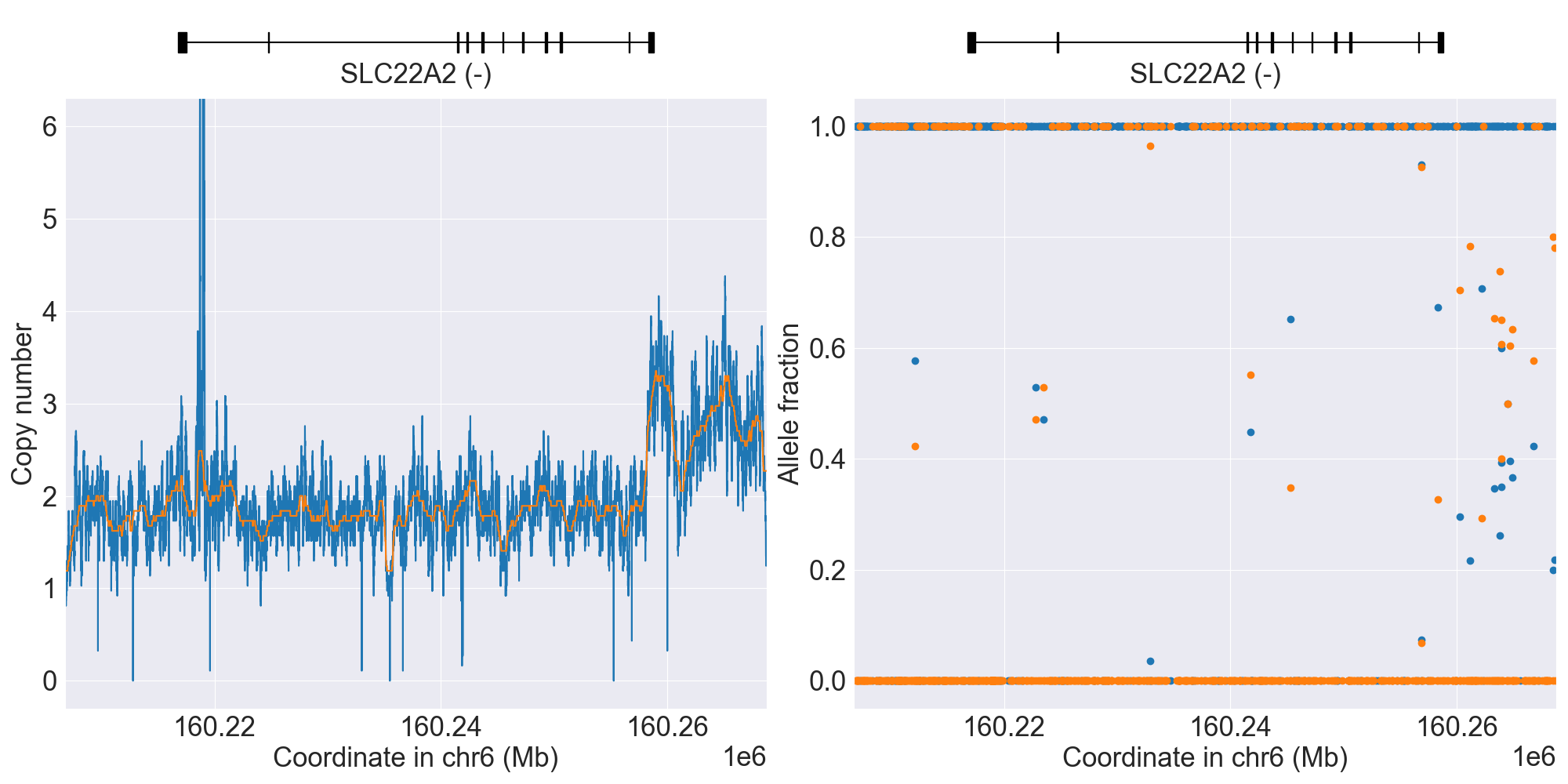
SLC22A2
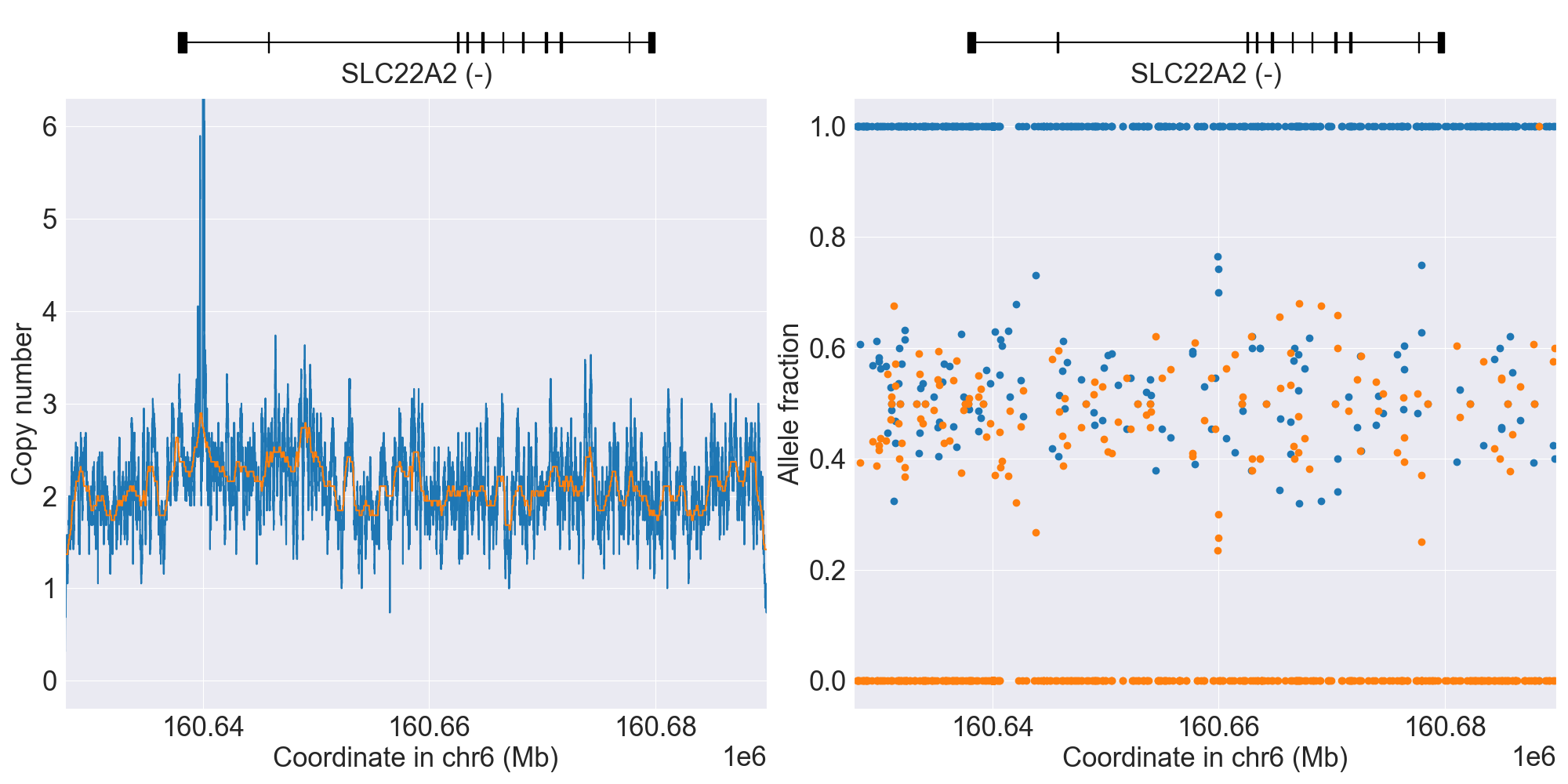
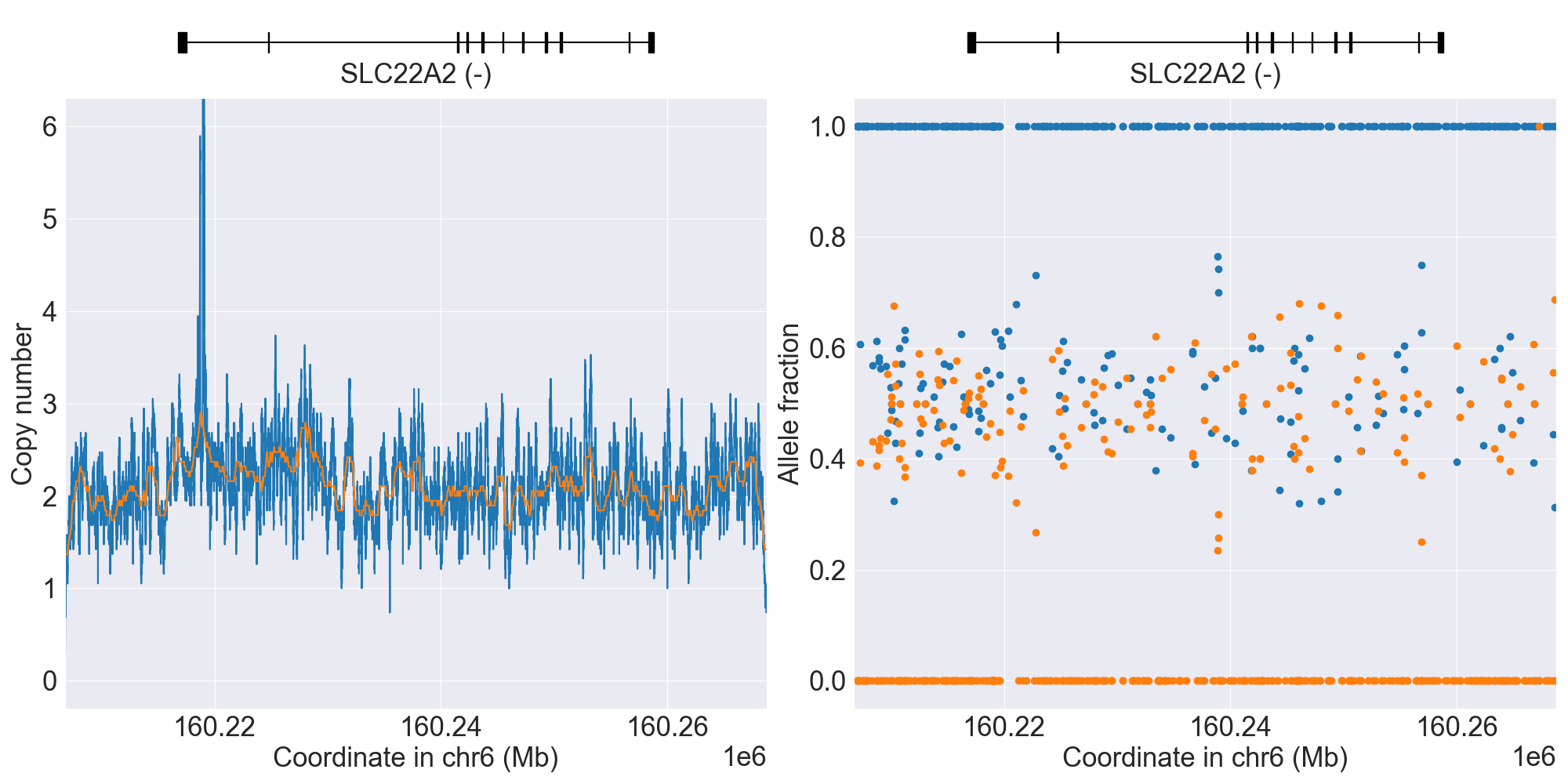
SV summary for SLC22A2
Below is comprehensive summary of SV described from real NGS studies:
SV Alleles |
SV Name |
Genotype |
Reference |
Gene Model |
GRCh37 |
GRCh38 |
Data Type |
Source |
Coriell ID |
Version |
Description |
|---|---|---|---|---|---|---|---|---|---|---|---|
Normal |
*1/*3 |
WGS |
HG01190 |
0.4.1 |
|||||||
*S1 |
NoncodingDel1 |
*1/*S1 |
WGS |
NA18855 |
0.4.1 |
||||||
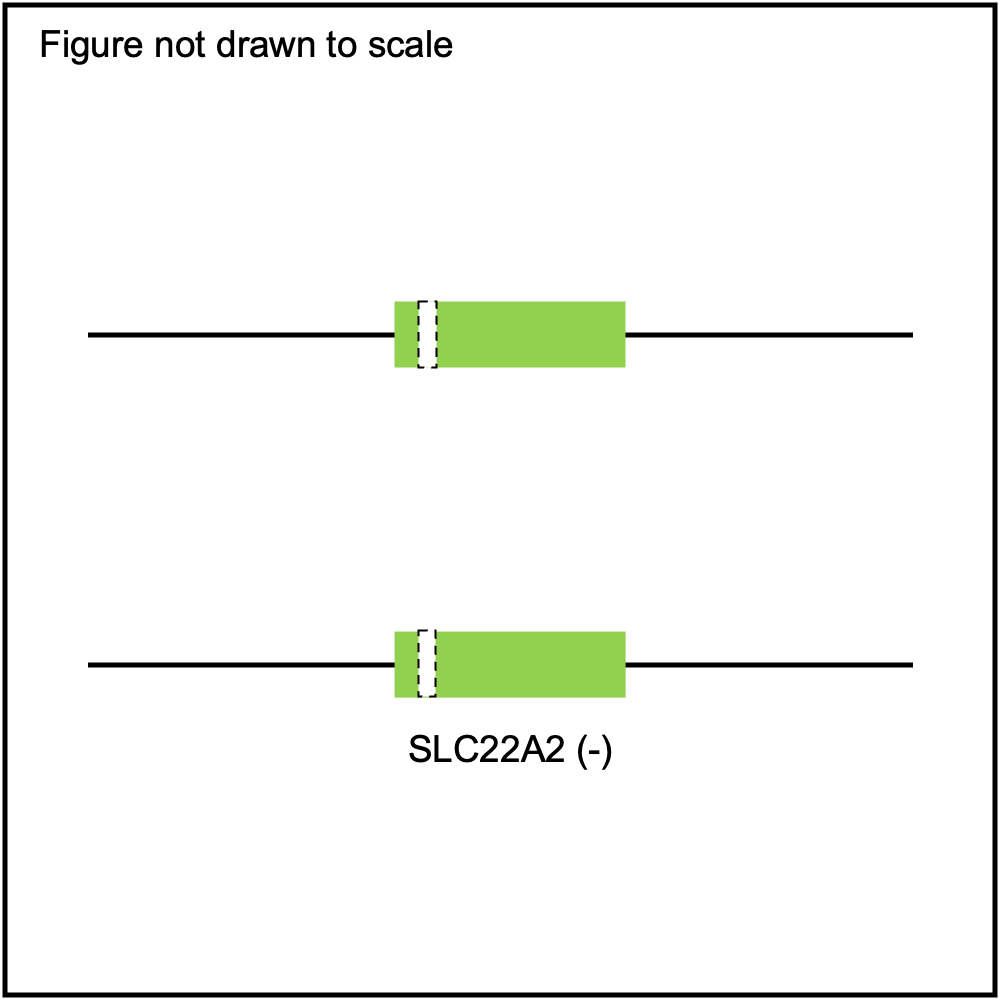
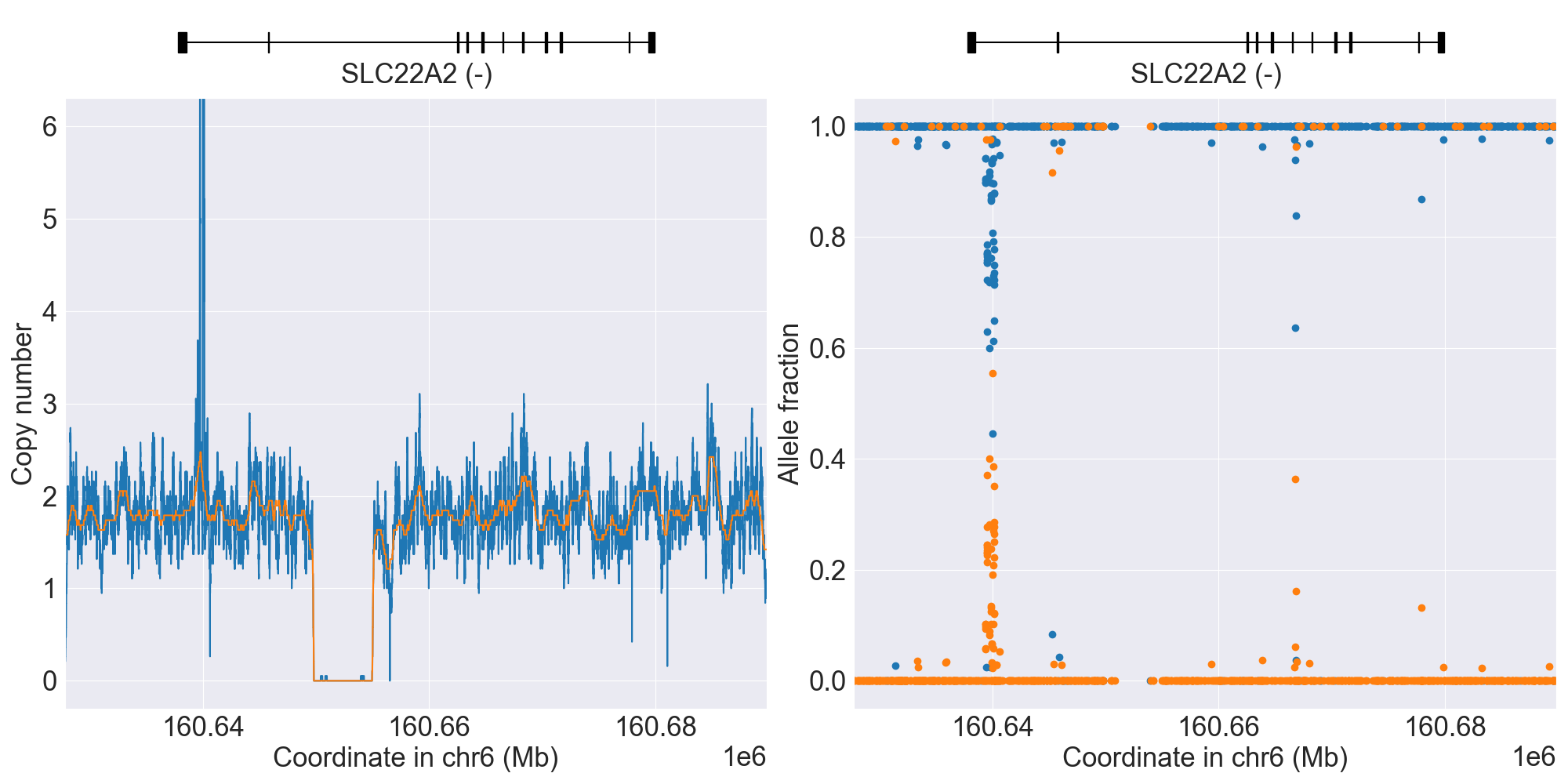
*S1 |
NoncodingDel1Hom |
*S1/*S1 |
WGS |
HG02337 |
0.16.0 |
||||||
*S2 |
PartialDel1 |
*1/*S2 |
WGS |
NA19819 |
0.4.1 |
||||||
*S1, *S2 |
NoncodingDel1+PartialDel1 |
*S1/*S2 |
WGS |
NA19030 |
0.13.0 |
||||||
PartialDup1 |
Indeterminate |
WGS |
NA20813 |
0.14.0 |
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
PyPGx was recently applied to the entire high-coverage WGS dataset from 1KGP (N=2,504). Click here to see individual SV calls for SLC22A2, and corresponding copy number profiles and allele fraction profiles.
SLCO1B1
Phenotype summary for SLCO1B1
Diplotype-phenotype mapping is used for phenotype prediction.
Phenotype |
Example |
Priority |
|---|---|---|
Increased Function |
*14/*14 |
None |
Normal Function |
*1/*1 |
Normal/Routine/Low Risk |
Possible Decreased Function |
*2/*15 |
Abnormal/Priority/High Risk |
Decreased Function |
*1/*5 |
Abnormal/Priority/High Risk |
Poor Function |
*5/*5 |
Abnormal/Priority/High Risk |
Indeterminate |
*2/*38 |
None |
Recommendations for SLCO1B1
Atorvastatin
“Prescribe ≤20mg for patients with SLCO1B1 poor function phenotype and ≤40mg for patients with SLCO1B1 decreased or possible decreased phenotype as a starting dose. Adjust doses of atorvastatin based on disease-specific guidelines. Prescriber should be aware of possible increased risk for myopathy especially for 40mg dose.” (Source: PharmGKB)
Fluvastatin
“CYP2C9 IMs should avoid fluvastatin doses greater than 40mg while CYP2C9 PMs should avoid doses greater than 20mg. If higher doses are required for desired efficacy, an alternative statin should be considered. Patients with SLCO1B1 poor function should also avoid fluvastatin doses greater than 40mg and and adjust doses of fluvastatin based on disease-specific guidelines. Patients with both SLCO1B1 poor function and CYP2C9 IM/PM should be prescribed an alternative statin depending on the desired potency.” (Source: PharmGKB)
Lovastatin
“Prescribe an alternative statin depending on the desired potency for patients with SLCO1B1 decreased function, possible decreased function or poor function phenotype. If lovastatin therapy is warranted in patients with SLCO1B1 decreased or possible decreased phenotype, limit dose to <20mg/day.” (Source: PharmGKB)
Pitavastatin
“Prescribe ≤1mg as a starting dose for patients with SLCO1B1 poor function phenotype. Prescribe ≤2mg as a starting dose for patients with SLCO1B1 decreased or possible decreased phenotype. Adjust doses of pitavastatin based on disease-specific guidelines. Consider an alternative statin or combination therapy if higher doses are needed.” (Source: PharmGKB)
Pravastatin
“Prescribe ≤40mg as a starting dose and adjust doses of pravastatin based on disease-specific guidelines for patients with SLCO1B1 poor function phenotype. Prescribe desired starting dose and adjust doses of pravastatin based on disease-specific guidelines for patients with SLCO1B1 decreased or possible decreased phenotype. Prescriber should be aware of possible increased risk for myopathy with pravastatin especially with doses >40mg per day.” (Source: PharmGKB)
Rosuvastatin
“Prescribe ≤20mg as a starting dose and adjust doses of rosuvastatin based on disease-specific and specific population guidelines for patients who are SLCO1B1 or ABCG2 poor function phenotype. If dose >20mg needed for desired efficacy, consider combination therapy (i.e. rosuvastatin plus non-statin guideline directed medical therapy). Patients with both ABCG2 poor function and SLCO1B1 poor/decreased function should be prescribed ≤10mg as a starting dose.” (Source: PharmGKB)
Simvastatin
“Prescribe an alternative statin depending on the desired potency for patients with SLCO1B1 decreased function, possible decreased function or poor function phenotype. If simvastatin therapy is warranted in patients with SLCO1B1 decreased or possible decreased phenotype, limit dose to <20mg/day.” (Source: PharmGKB)
Resources for SLCO1B1
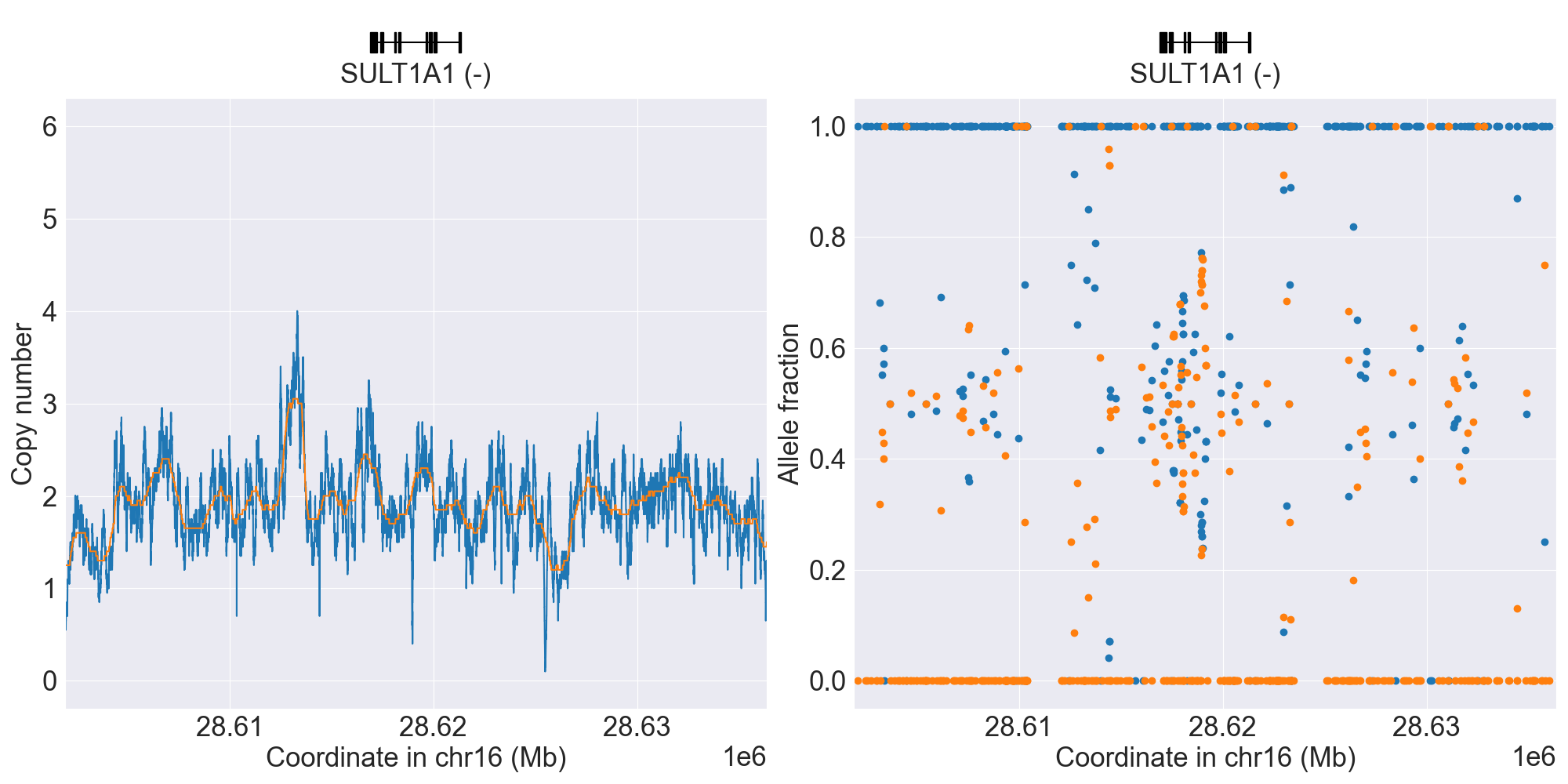
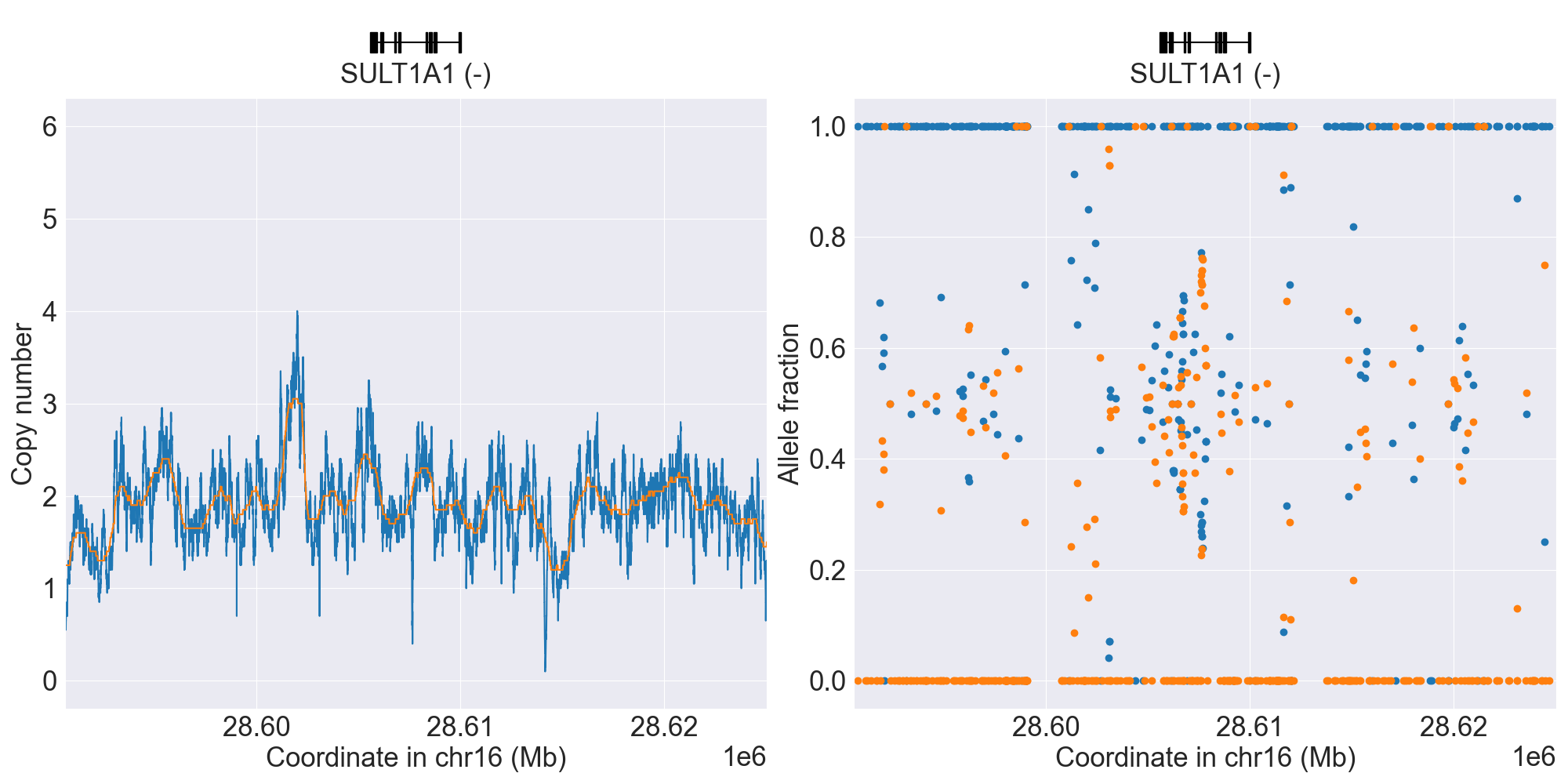
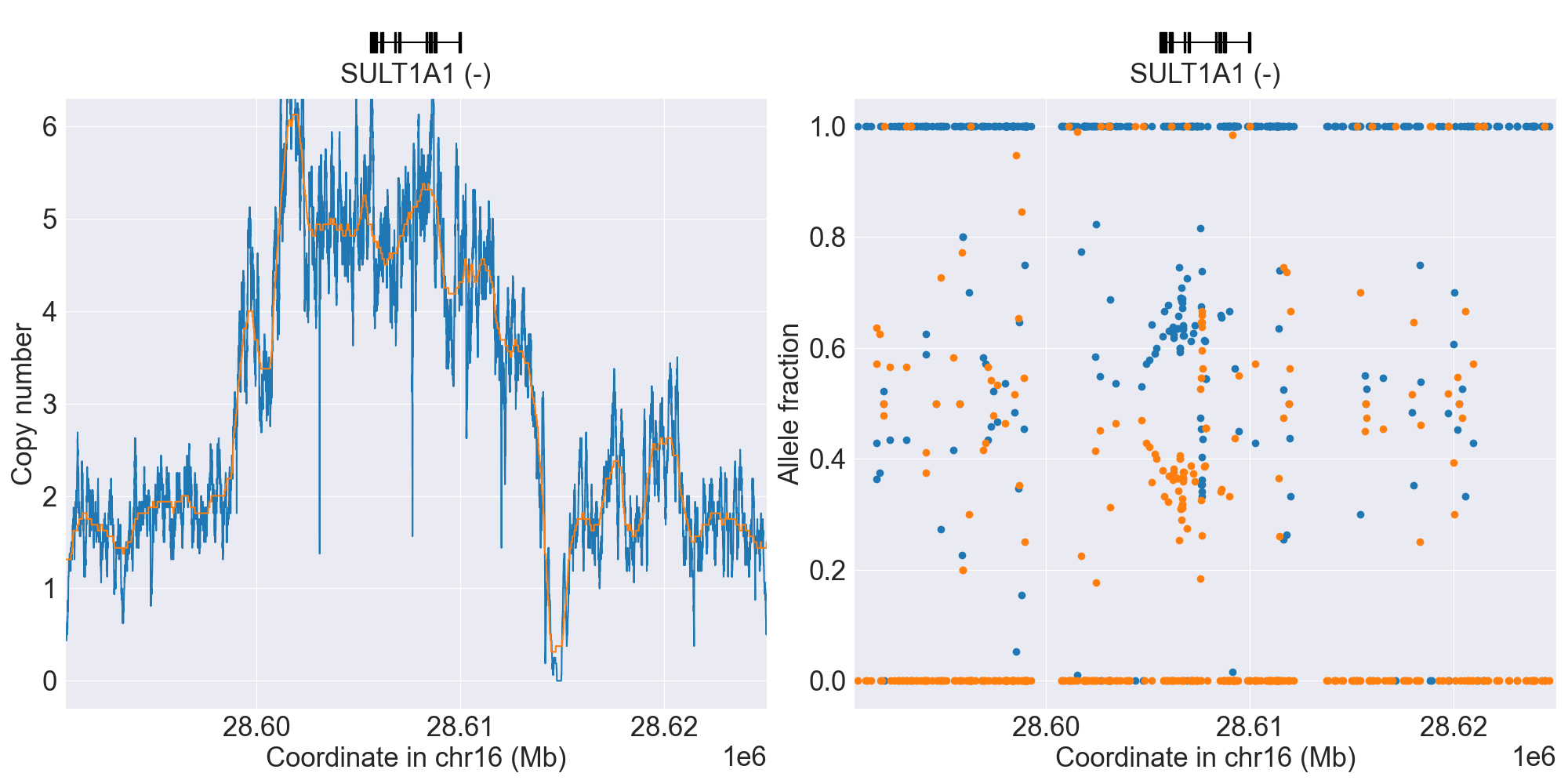
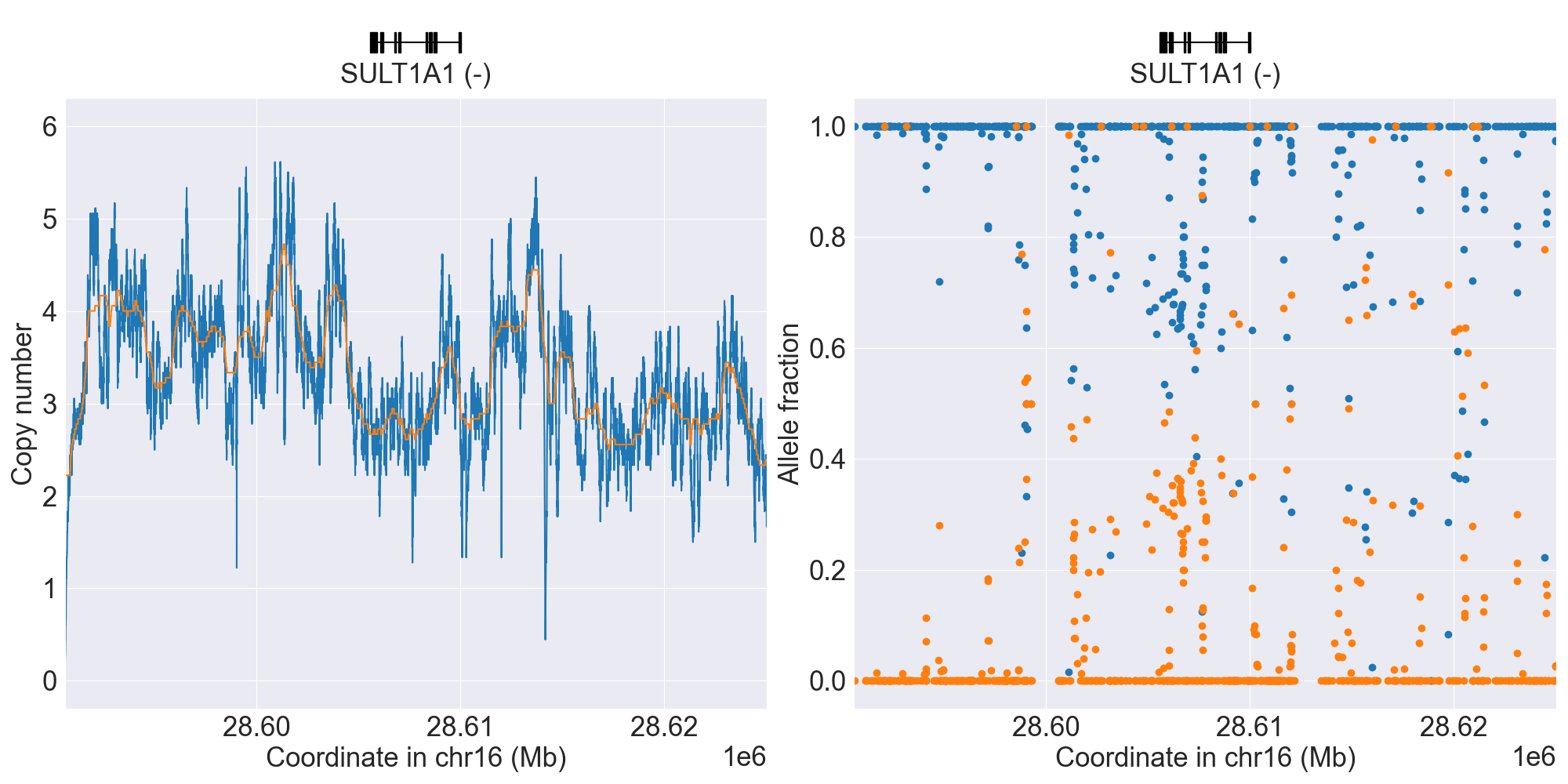
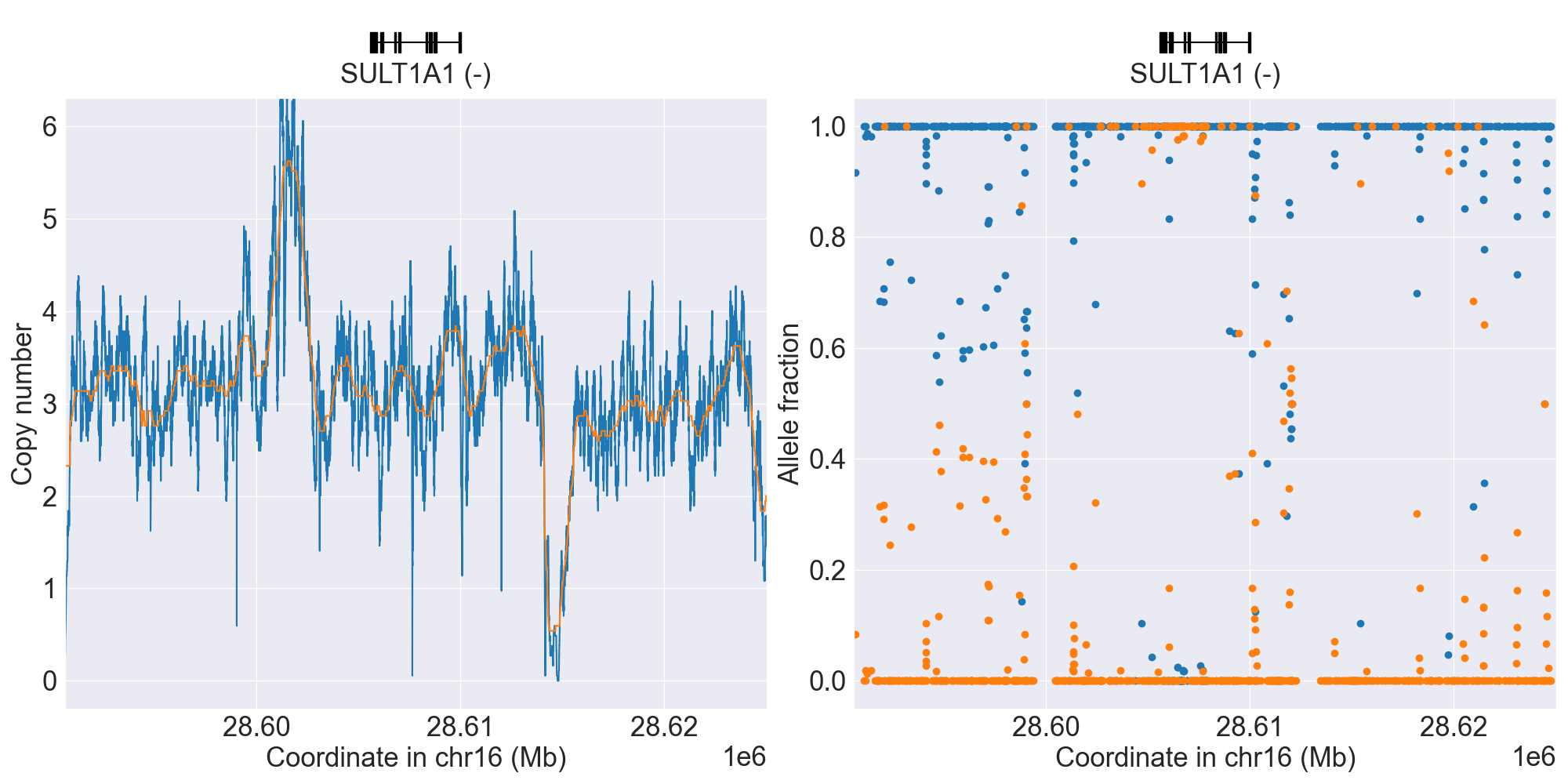
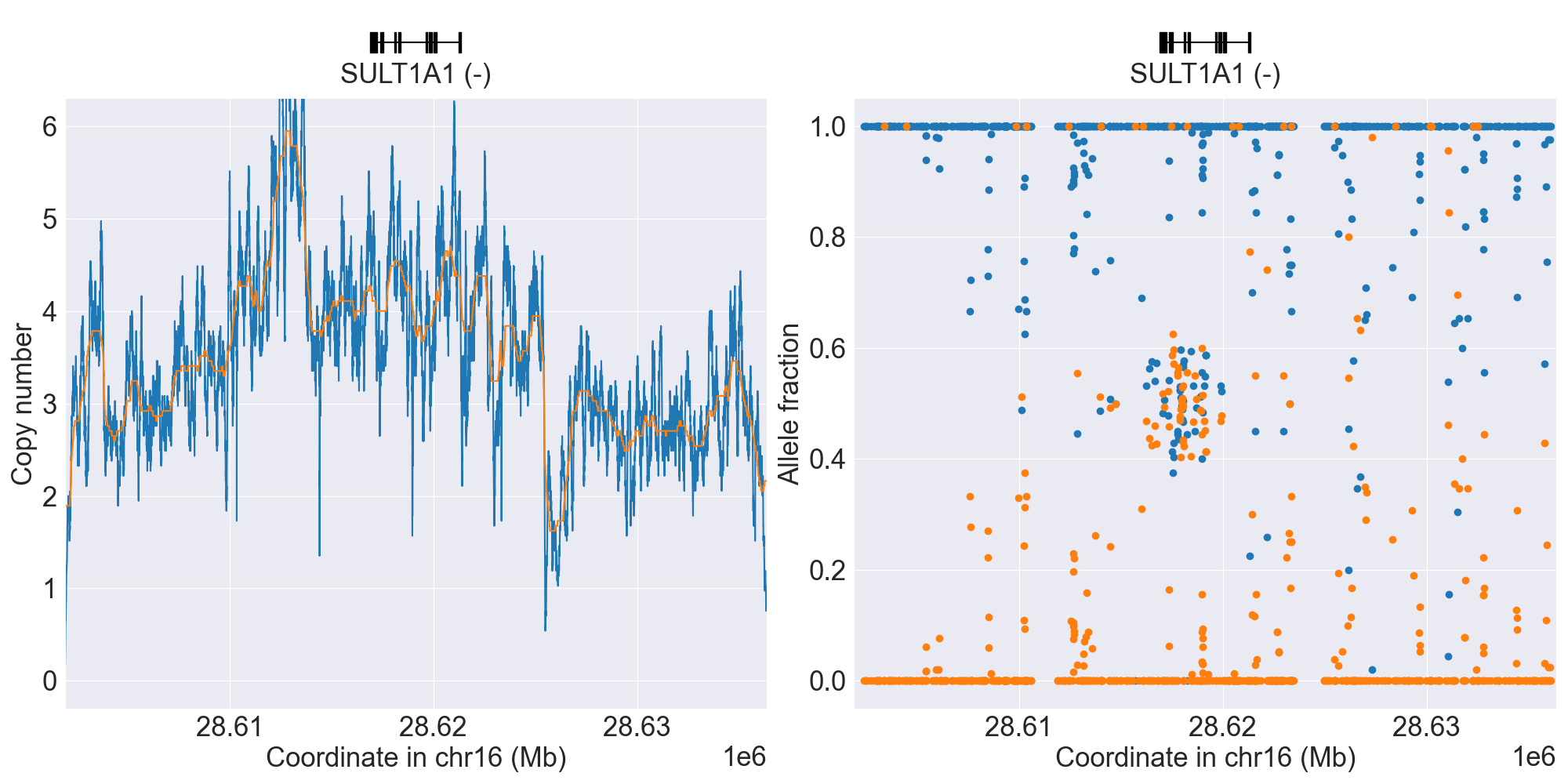
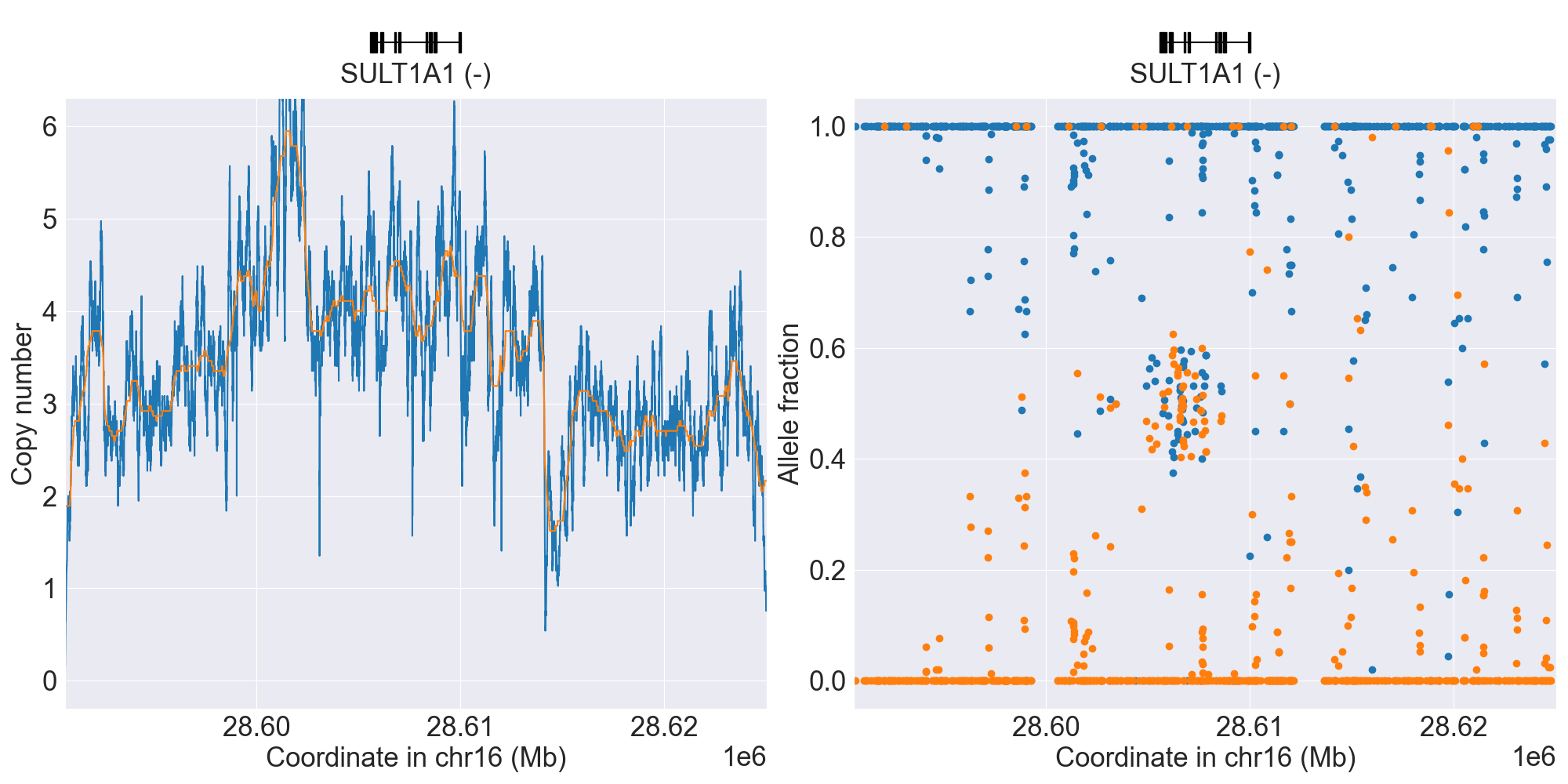
SULT1A1
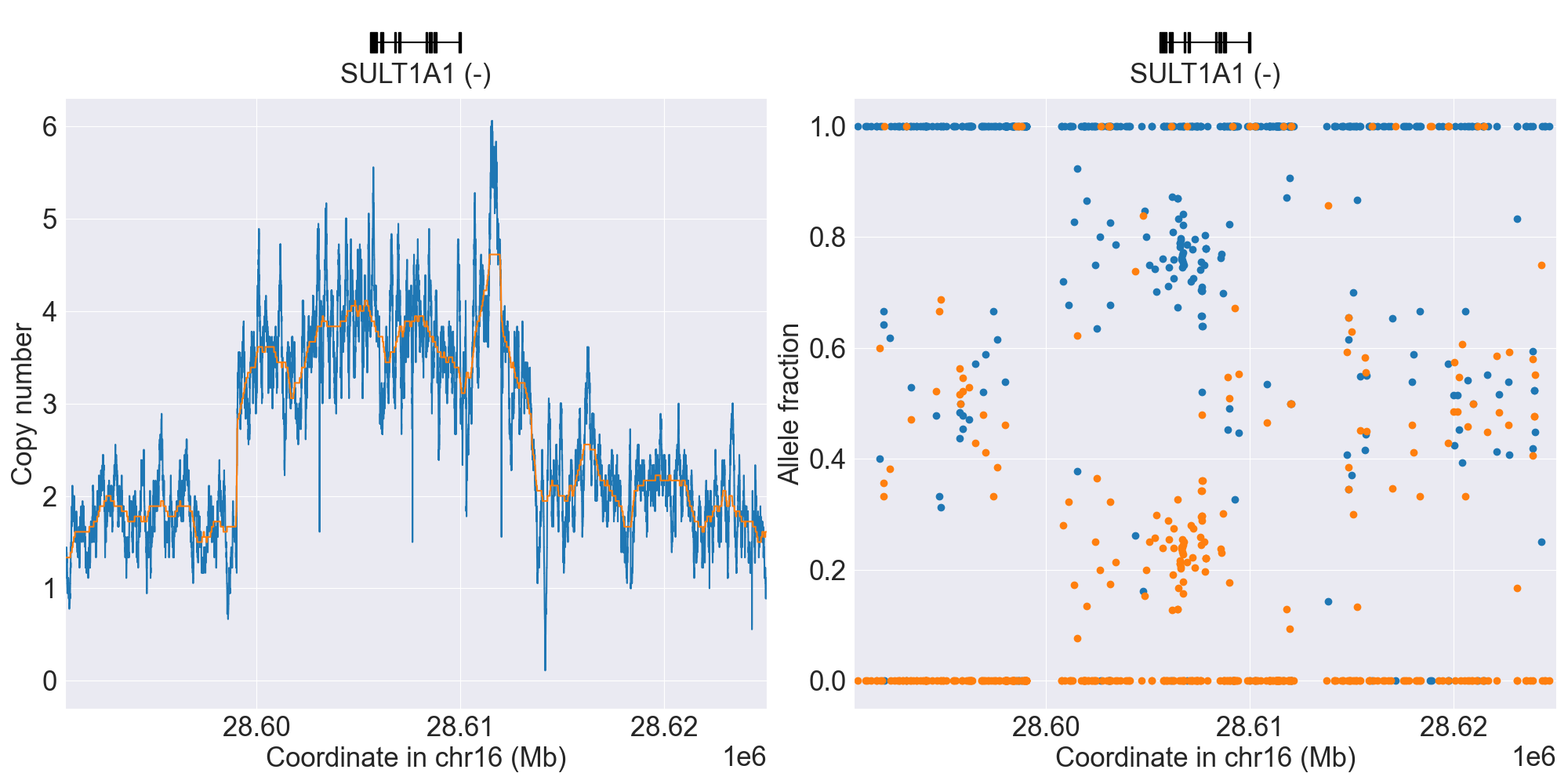
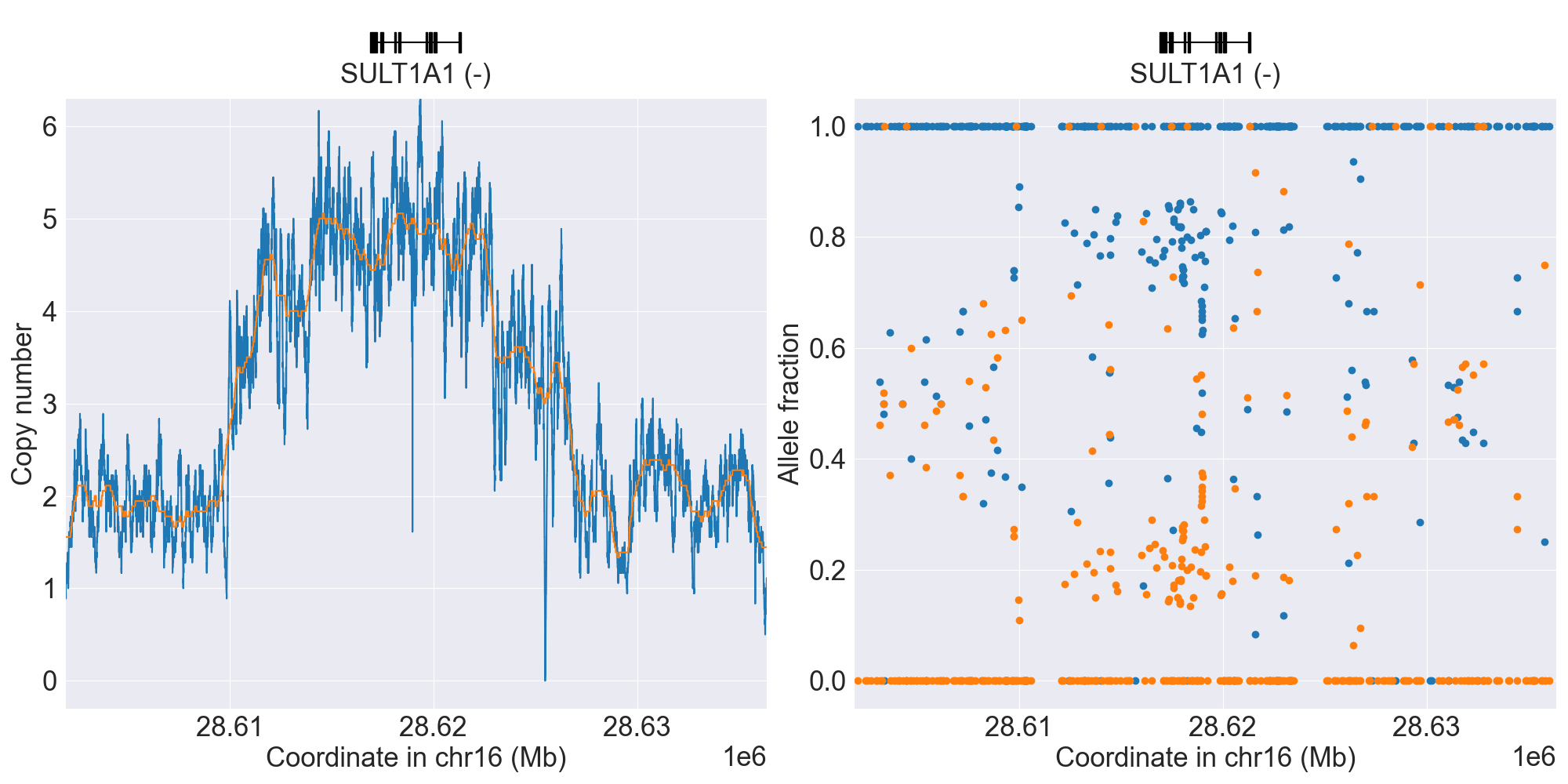
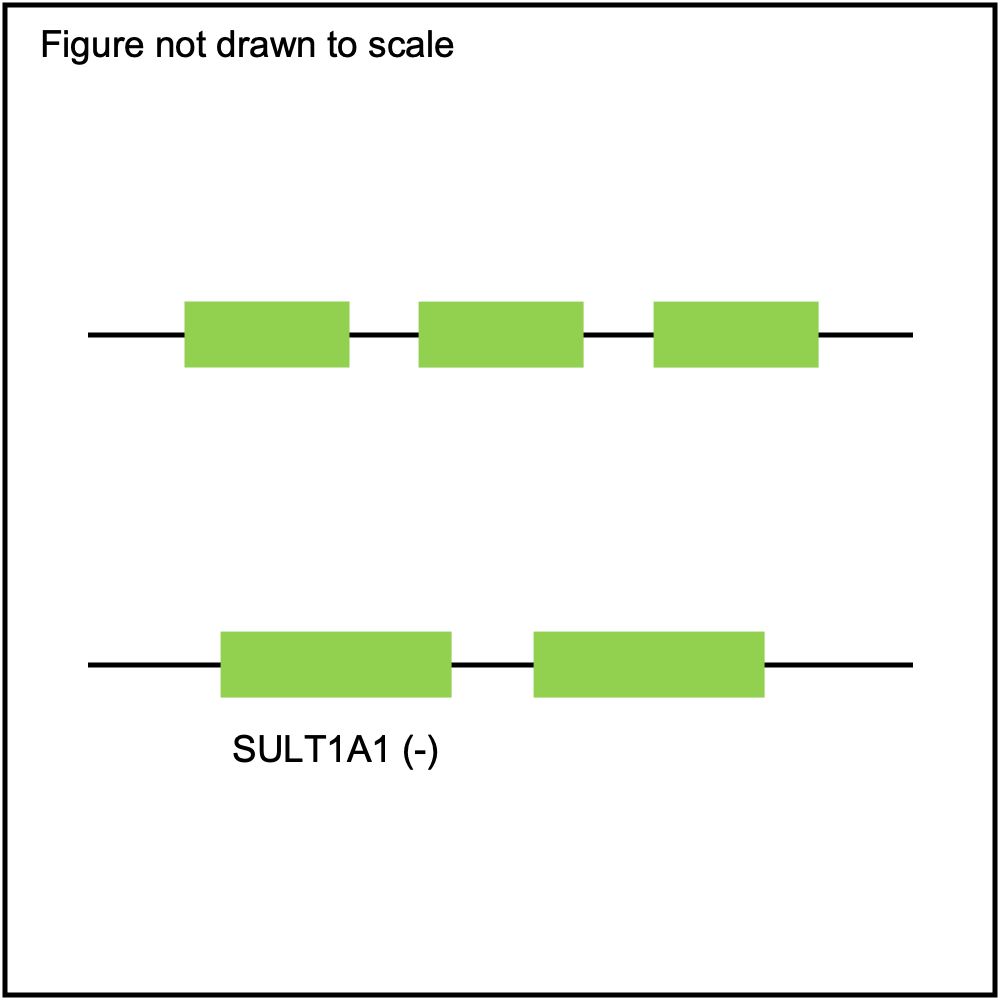
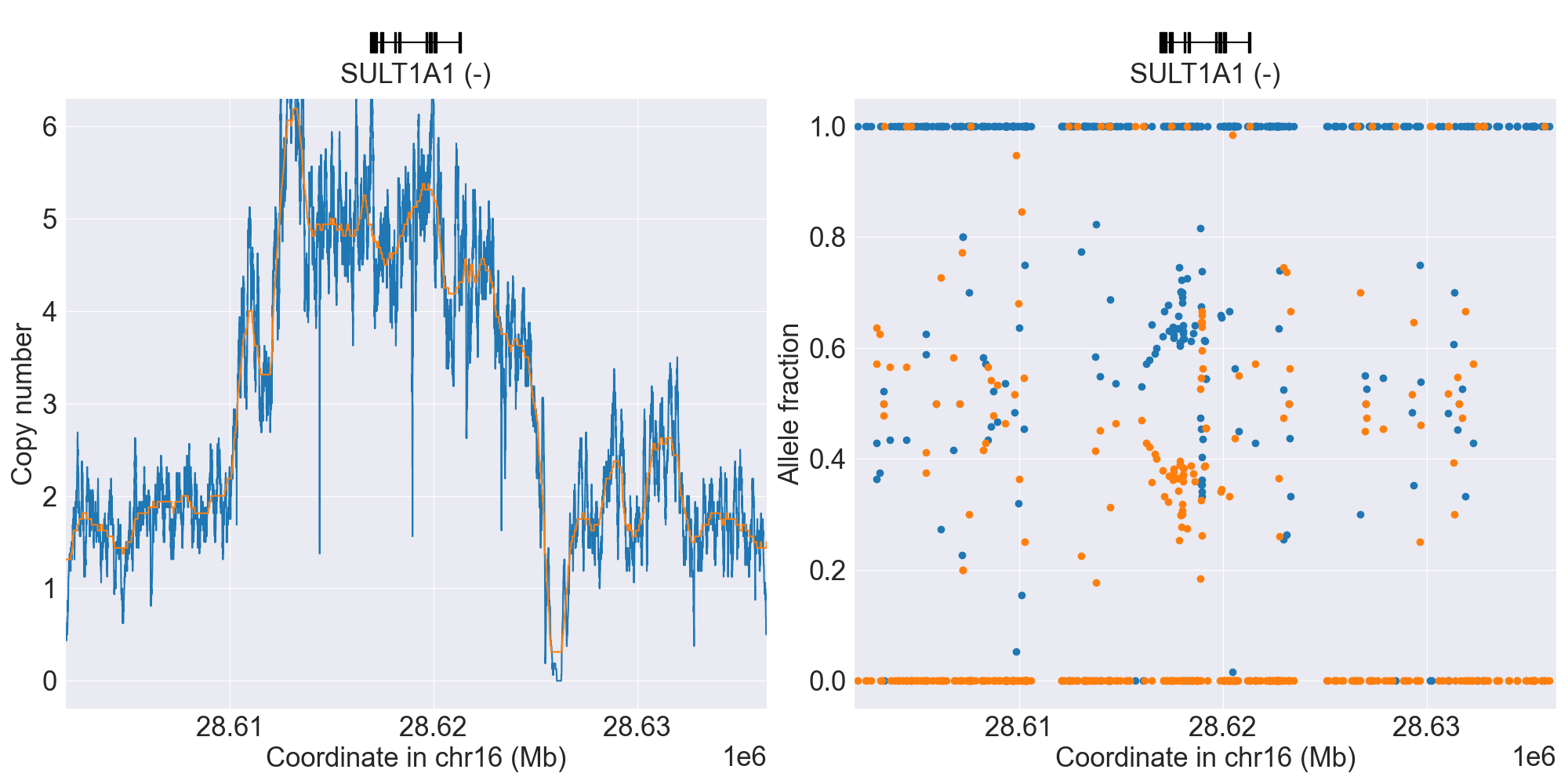
SV summary for SULT1A1
Below is comprehensive summary of SV described from real NGS studies:
SV Alleles |
SV Name |
Genotype |
Reference |
Gene Model |
GRCh37 |
GRCh38 |
Data Type |
Source |
Coriell ID |
Version |
Description |
|---|---|---|---|---|---|---|---|---|---|---|---|
Normal |
*1/*2 |
WGS |
NA06991 |
0.11.0 |
|||||||
*DEL |
WholeDel1 |
*1/*DEL |
WGS |
NA18942 |
0.11.0 |
||||||
*DEL |
WholeDel1Hom |
*DEL/*DEL |
WGS |
NA20874 |
0.14.0 |
||||||
*1x2 |
WholeDup1 |
*1x2/*2 |
WGS |
NA18509 |
0.11.0 |
||||||
*1x3 |
WholeMultip1 |
*1x3/*2 |
WGS |
NA18868 |
0.11.0 |
||||||
*1x4 |
WholeMultip2 |
*1x4/*2 |
WGS |
NA18484 |
0.11.0 |
||||||
*1x3, *2x2 |
WholeMultip2 |
*1x3/*2x2 |
WGS |
NA19143 |
0.11.0 |
||||||
Unknown1 |
Indeterminate |
WGS |
HG01085 |
0.15.0 |
|||||||
Unknown2 |
Indeterminate |
WGS |
0.16.0 |
||||||||
Unknown3 |
Indeterminate |
WGS |
HG03854 |
0.16.0 |
|||||||
Unknown4 |
Indeterminate |
WGS |
HG03742 |
0.16.0 |
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
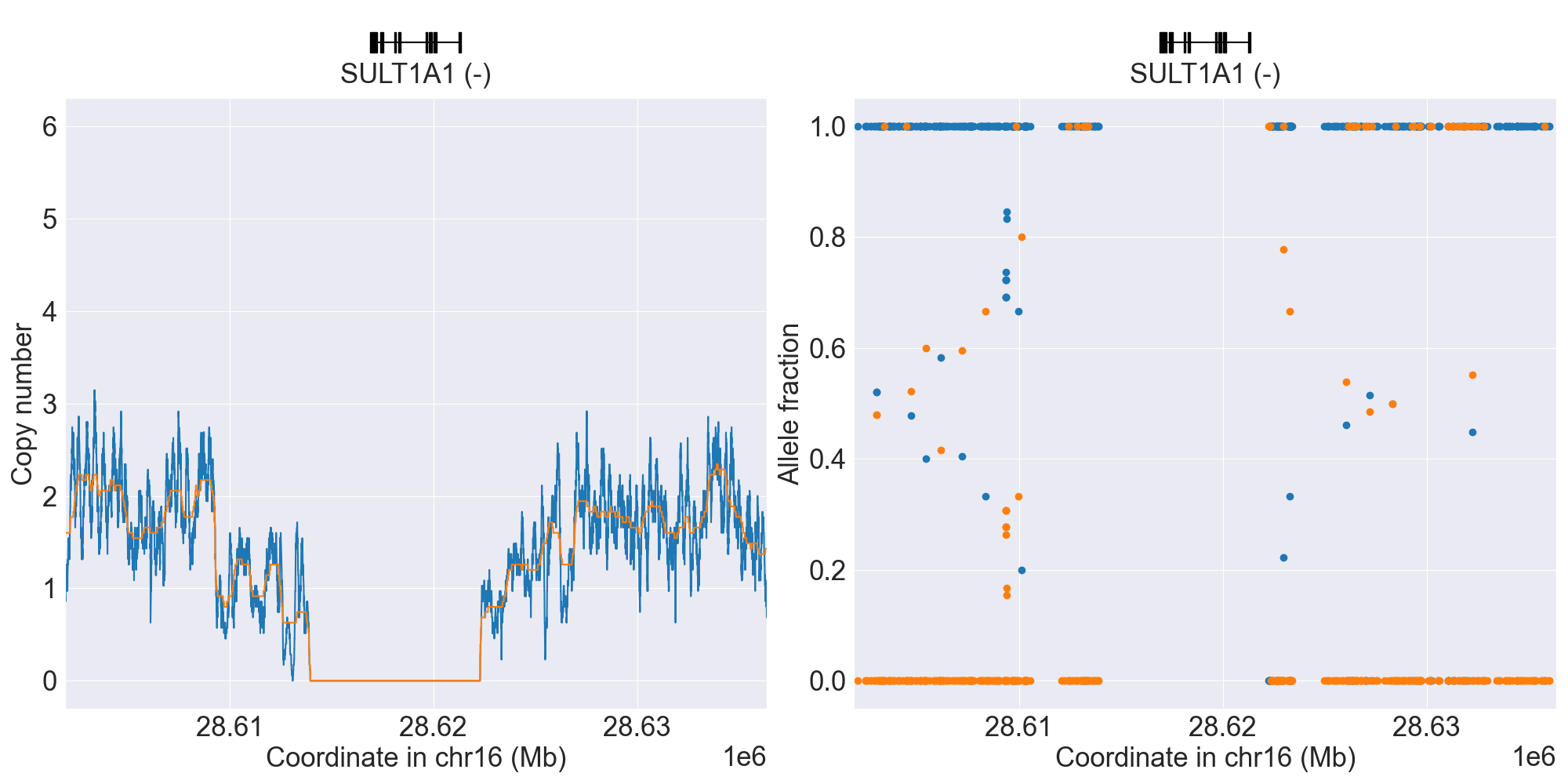
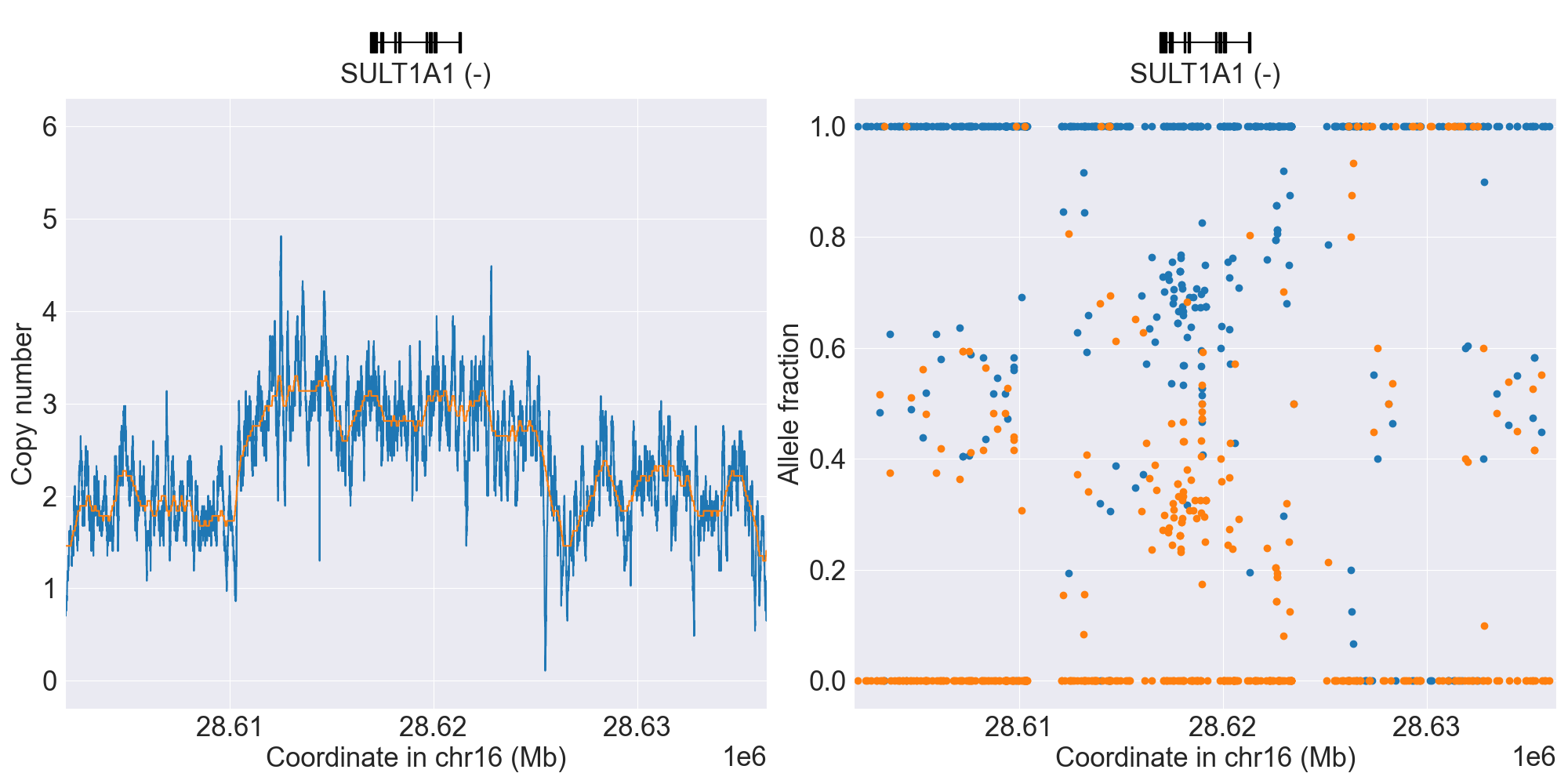
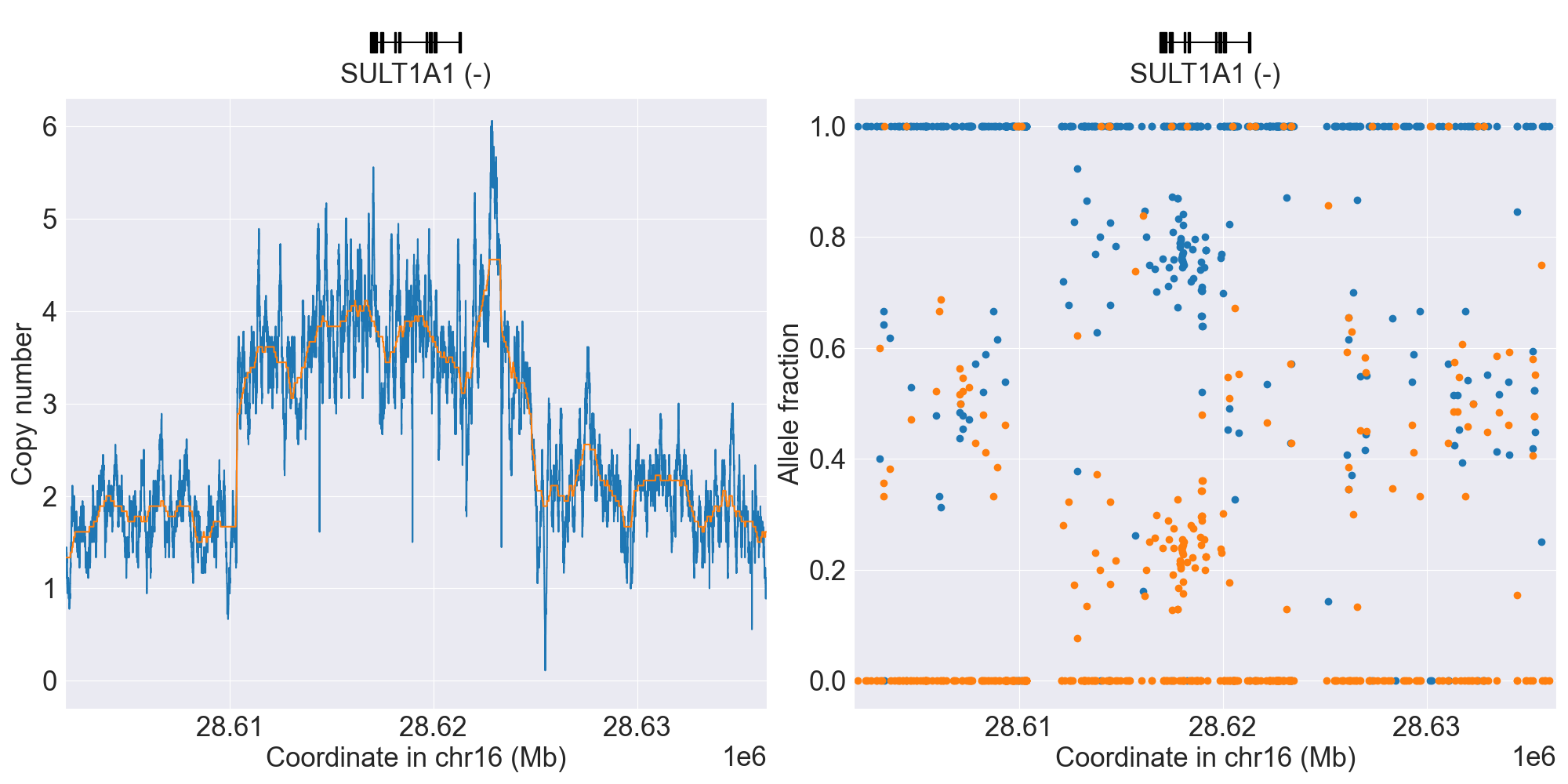
PyPGx was recently applied to the entire high-coverage WGS dataset from 1KGP (N=2,504). Click here to see individual SV calls for SULT1A1, and corresponding copy number profiles and allele fraction profiles.
TBXAS1
Resources for TBXAS1
TPMT
Phenotype summary for TPMT
Diplotype-phenotype mapping is used for phenotype prediction.
Phenotype |
Example |
Priority |
|---|---|---|
Normal Metabolizer |
*1/*1 |
Normal/Routine/Low Risk |
Possible Intermediate Metabolizer |
*3A/*12 |
Abnormal/Priority/High Risk |
Intermediate Metabolizer |
*1/*2 |
Abnormal/Priority/High Risk |
Poor Metabolizer |
*2/*3A |
Abnormal/Priority/High Risk |
Indeterminate |
*1/*18 |
Abnormal/Priority/High Risk |
Recommendations for TPMT
Azathioprine
“Consider an alternate agent or extreme dose reduction of azathioprine for patients who are TPMT or NUDT15 poor metabolizers. Start at 30-80% of target dose for patients who are TPMT or NUDT15 intermediate metabolizers.” (Source: PharmGKB)
Mercaptopurine
“Consider an alternate agent or extreme dose reduction of mercaptopurine for patients who are TPMT or NUDT15 poor metabolizers. Start at 30-80% of target dose for patients who are TPMT or NUDT15 intermediate metabolizers.” (Source: PharmGKB)
Thioguanine
“Consider an alternate agent or extreme dose reduction of thioguanine for patients who are TPMT or NUDT15 poor metabolizers. Start at 50-80% of target dose for patients who are TPMT or NUDT15 intermediate metabolizers.” (Source: PharmGKB)
Resources for TPMT
UGT1A1
Phenotype summary for UGT1A1
Diplotype-phenotype mapping is used for phenotype prediction.
Phenotype |
Example |
Priority |
|---|---|---|
Normal Metabolizer |
*1/*1 |
Normal/Routine/Low Risk |
Intermediate Metabolizer |
*1/*6 |
Normal/Routine/Low Risk |
Poor Metabolizer |
*6/*27 |
Abnormal/Priority/High Risk |
Indeterminate |
*28/*80 |
None |
Recommendations for UGT1A1
Atazanavir
“The CPIC dosing guideline recommends considering advising individuals who carry two decreased function UGT1A1 alleles about a substantial likelihood of developing jaundice, which may cause non-adherence. The dosing guideline recommends that alternative agents be considered if the risk of non-adherence due to jaundice is high. The risk of discontinuation is low and very low for individuals carrying one, or no decreased function UGT1A1 alleles, respectively.” (Source: PharmGKB)
Resources for UGT1A1
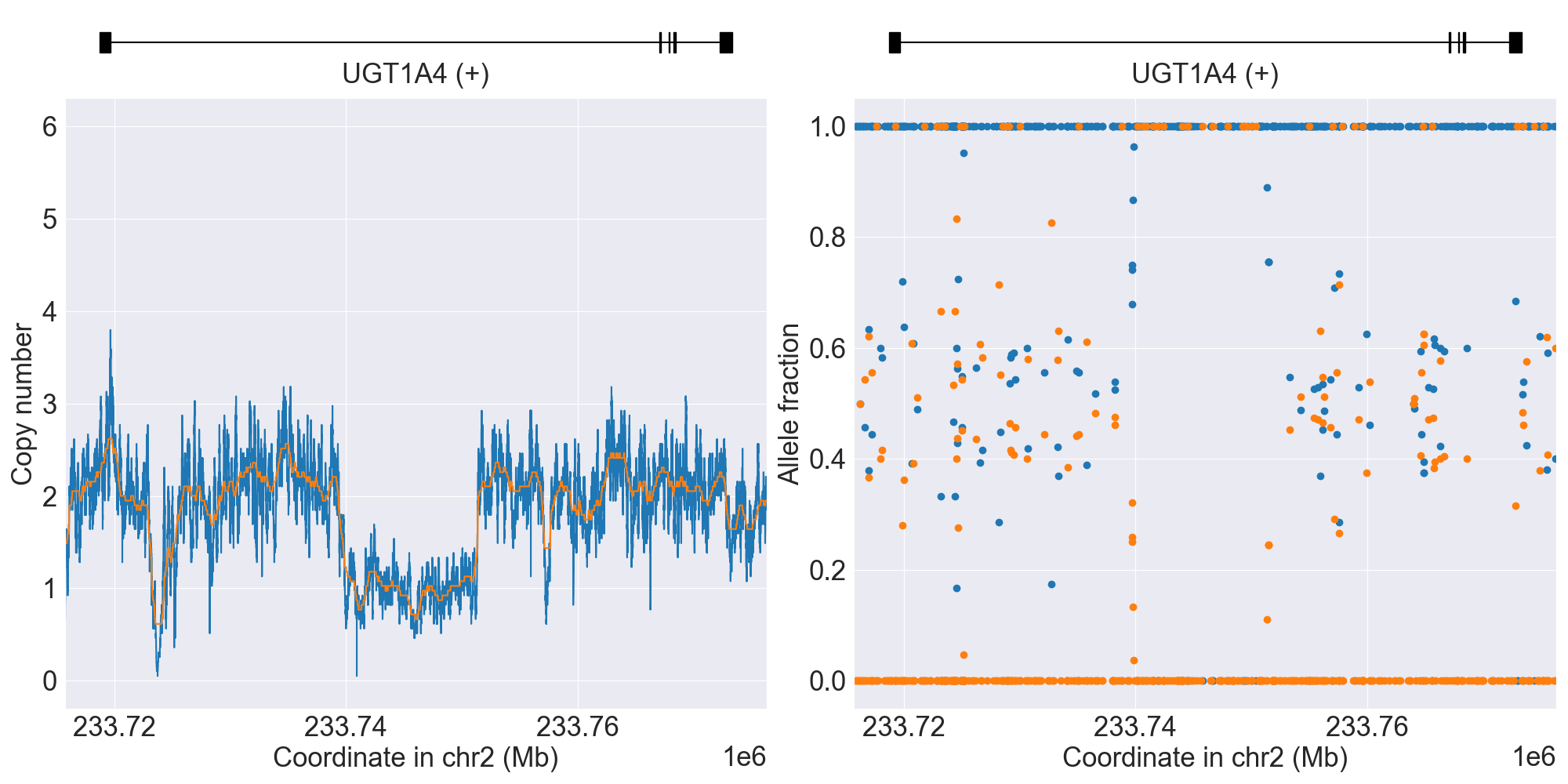
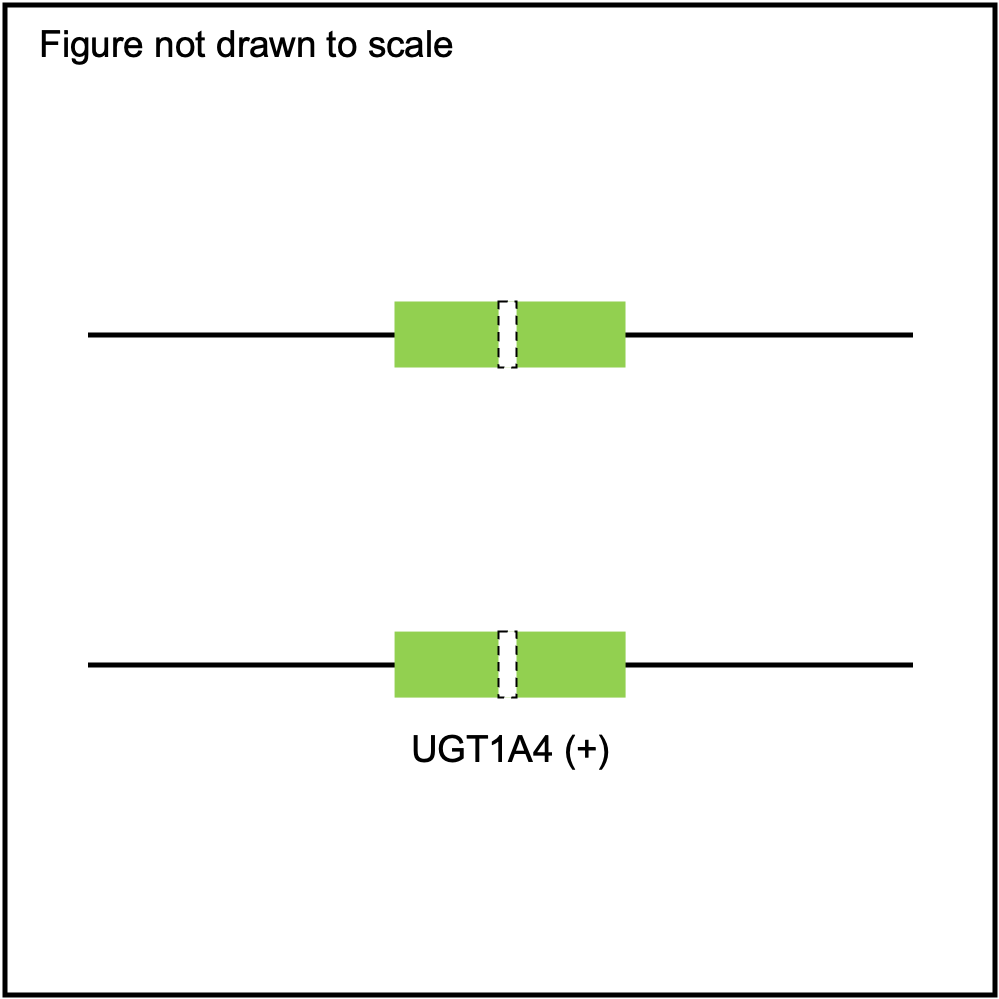
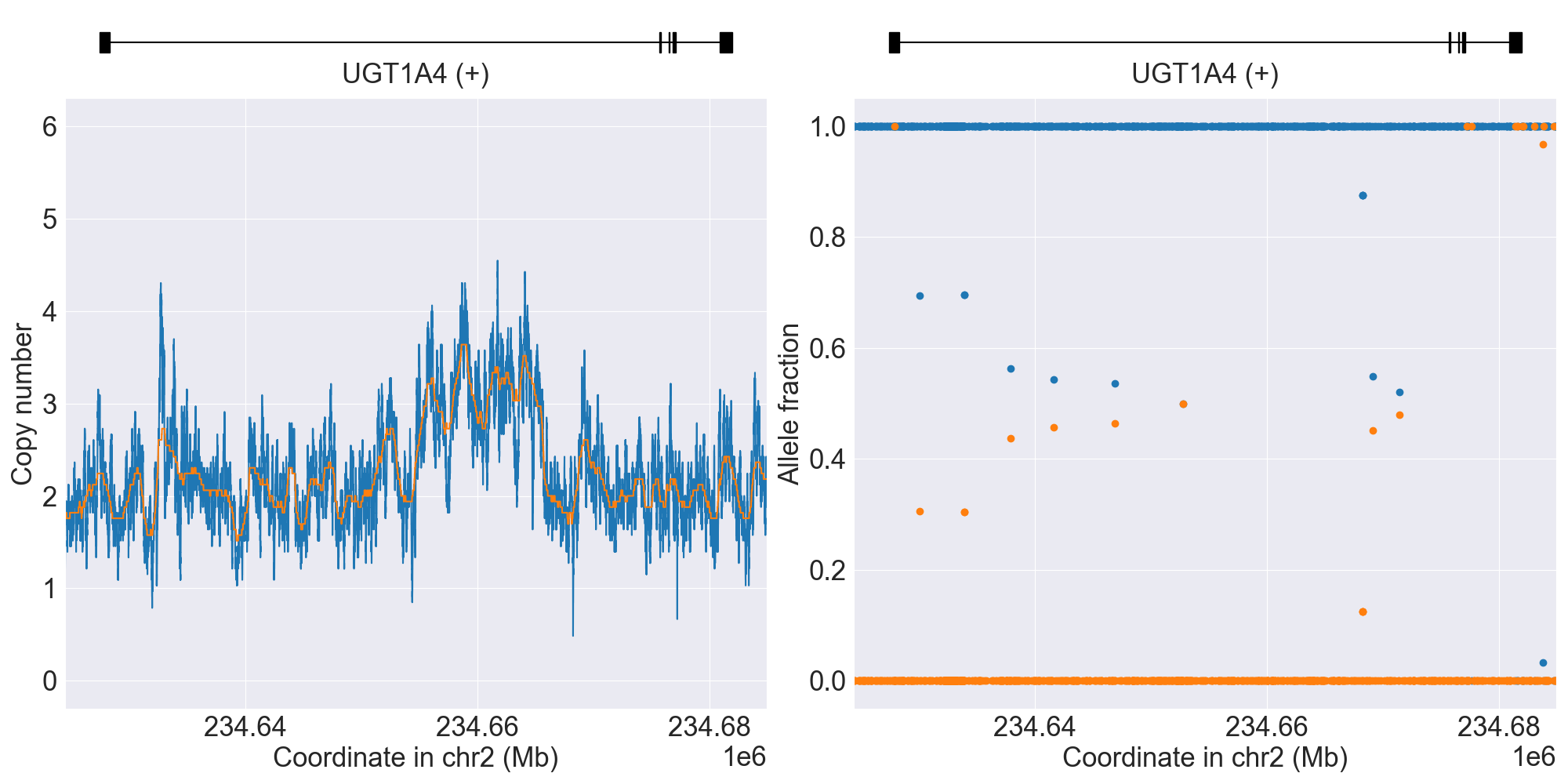
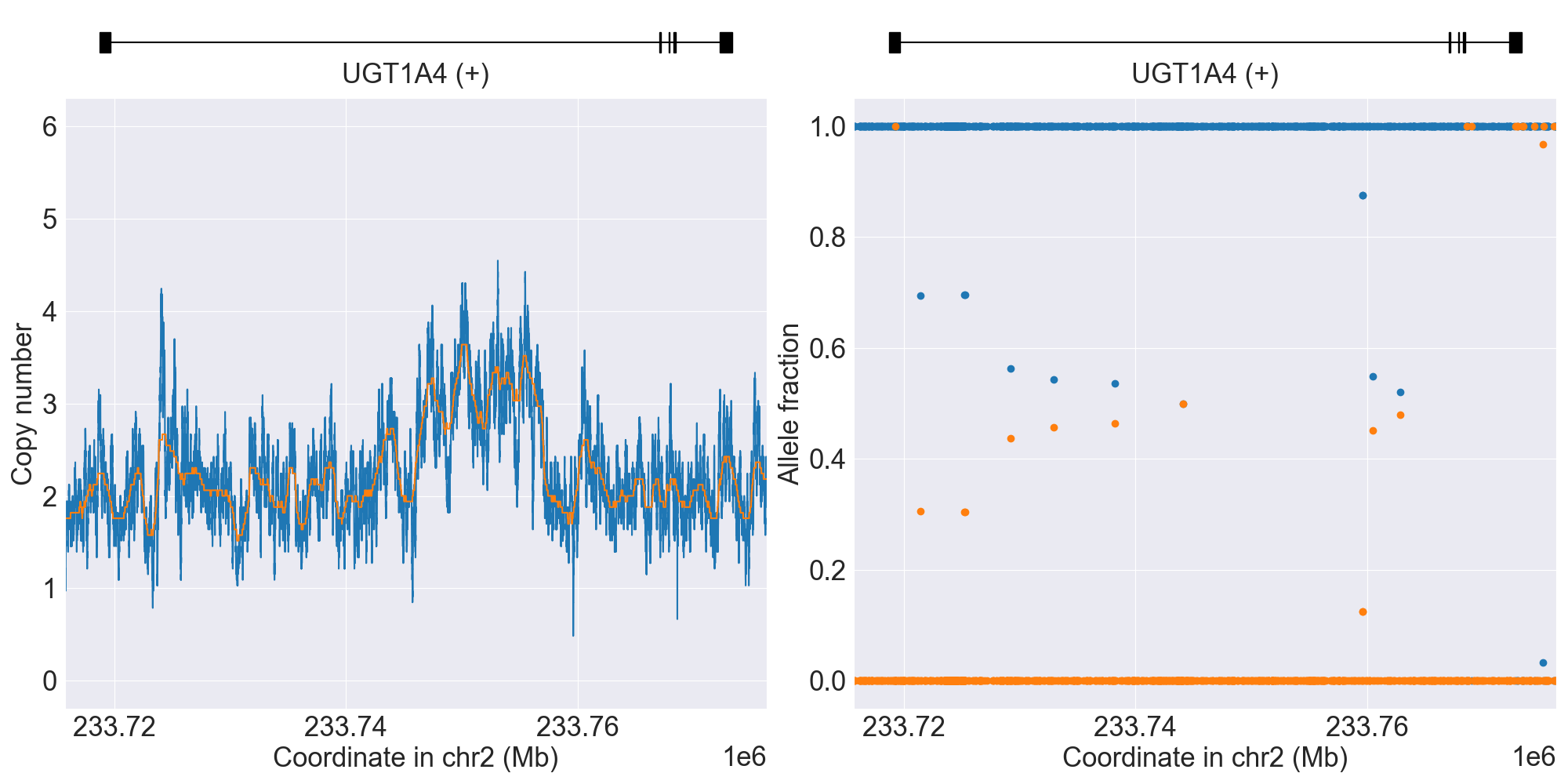
UGT1A4
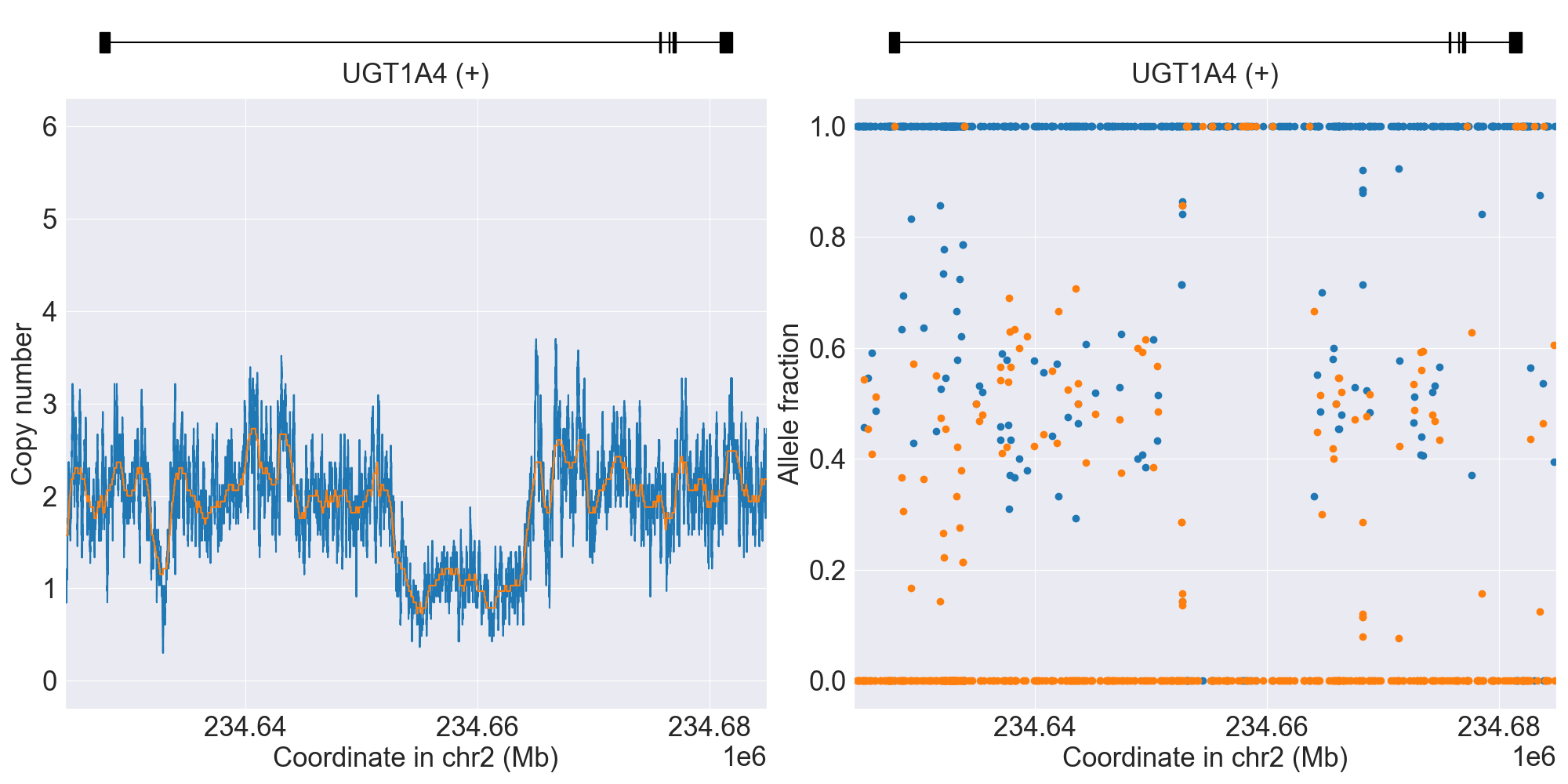
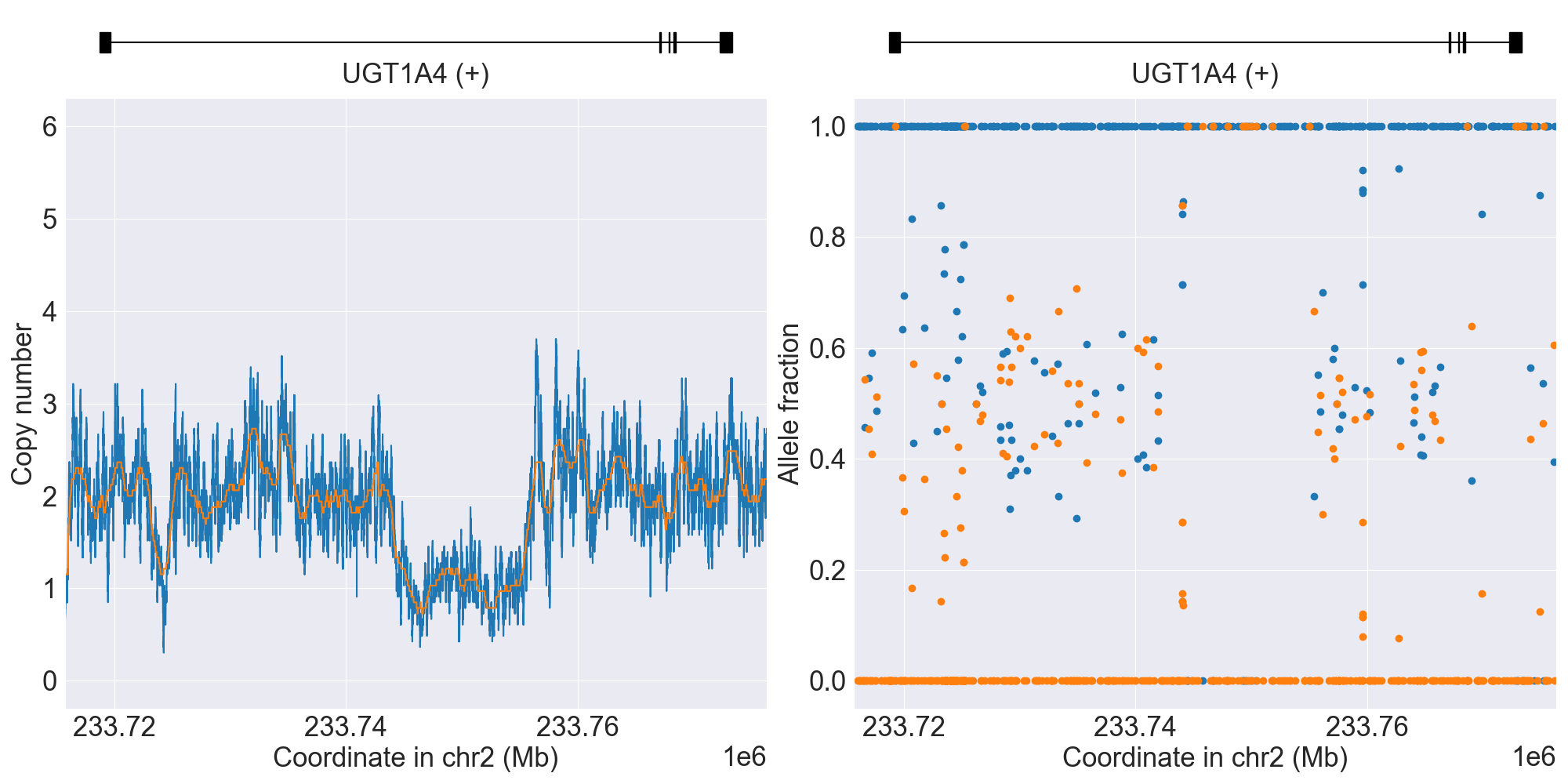
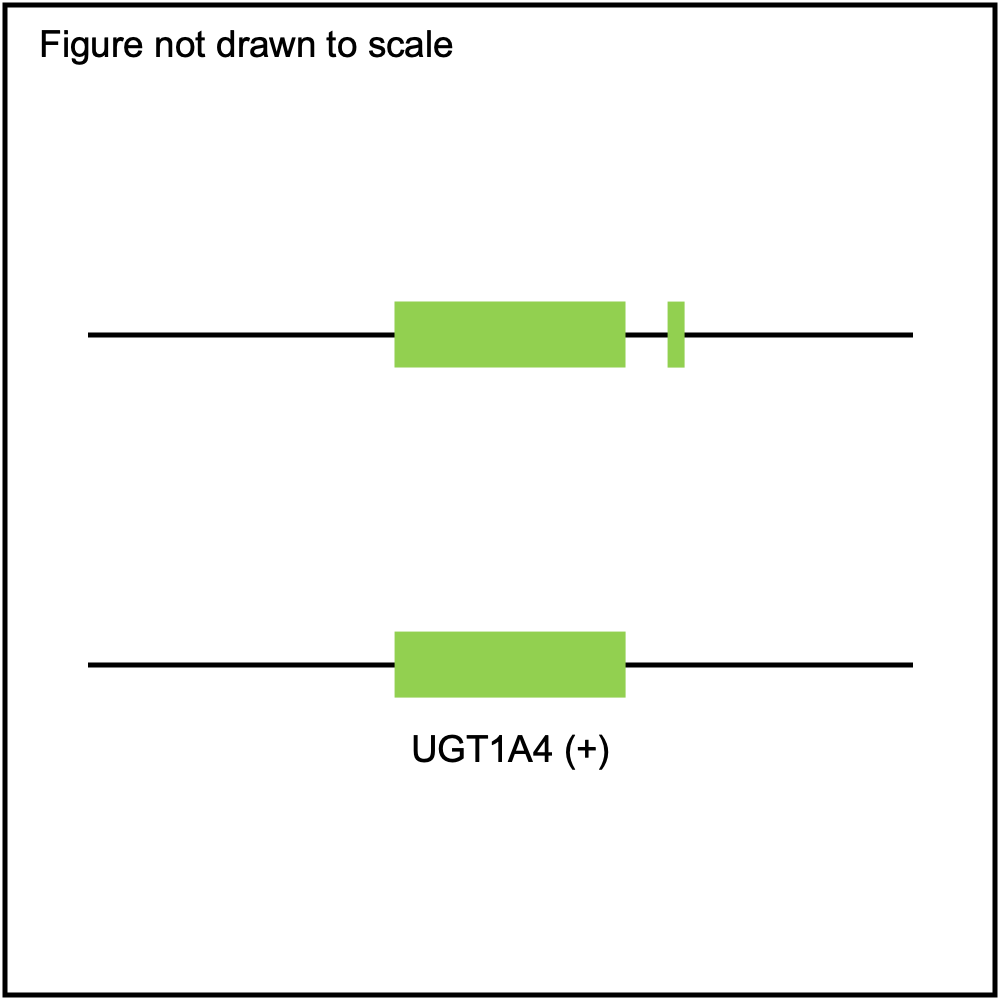
SV summary for UGT1A4
Below is comprehensive summary of SV described from real NGS studies:
SV Alleles |
SV Name |
Genotype |
Reference |
Gene Model |
GRCh37 |
GRCh38 |
Data Type |
Source |
Coriell ID |
Version |
Description |
|---|---|---|---|---|---|---|---|---|---|---|---|
Normal |
*1/*2 |
WGS |
NA11993 |
0.9.0 |
|||||||
*S1 |
NoncodingDel1 |
*1/*S1 |
WGS |
NA19908 |
0.9.0 |
||||||
*S1 |
NoncodingDel1Hom |
*S1/*S1 |
WGS |
HG03479 |
0.16.0 |
||||||
*S2 |
NoncodingDel2 |
*1/*S2 |
WGS |
0.10.0 |
|||||||
*S3 |
NoncodingDup1 |
*1/*S3 |
WGS |
NA18632 |
0.13.0 |
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
PyPGx was recently applied to the entire high-coverage WGS dataset from 1KGP (N=2,504). Click here to see individual SV calls for UGT1A4, and corresponding copy number profiles and allele fraction profiles.
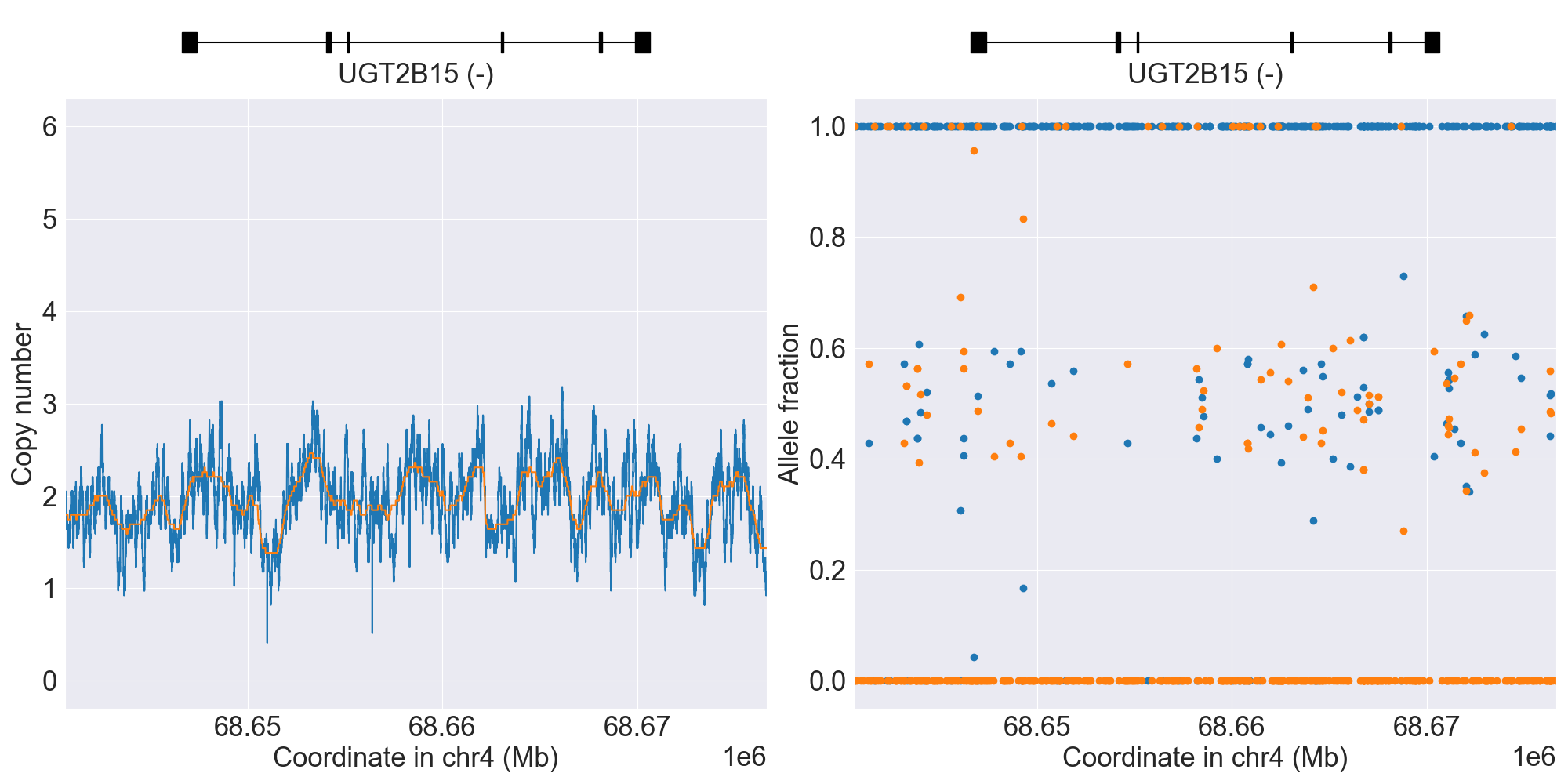
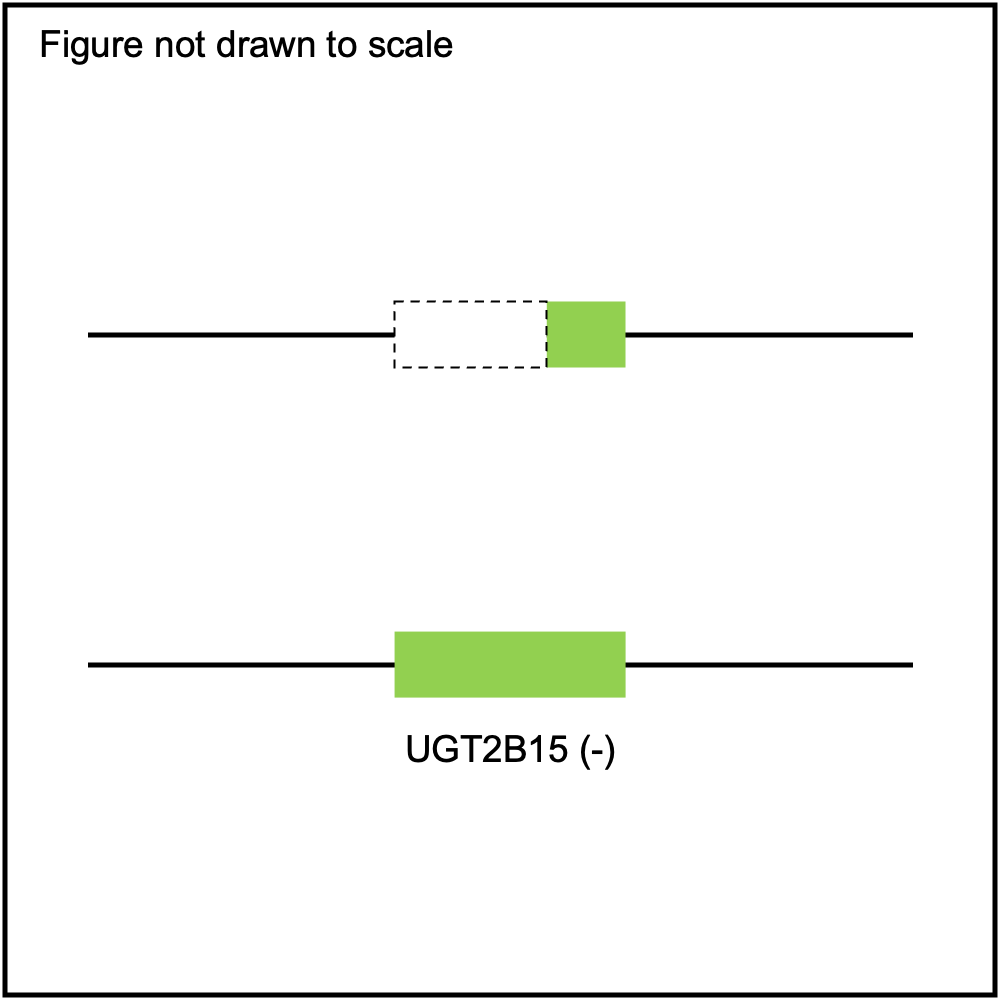
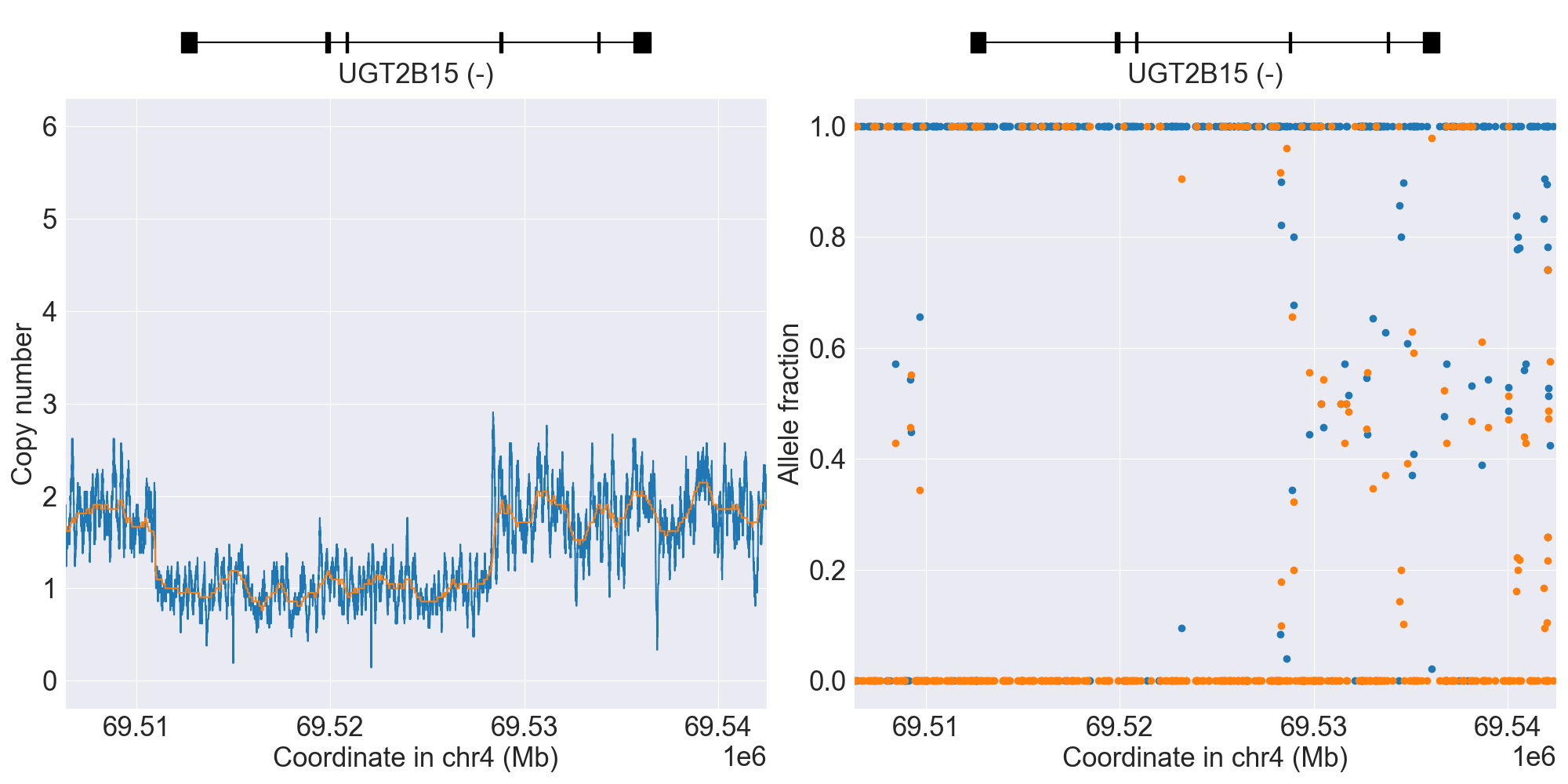
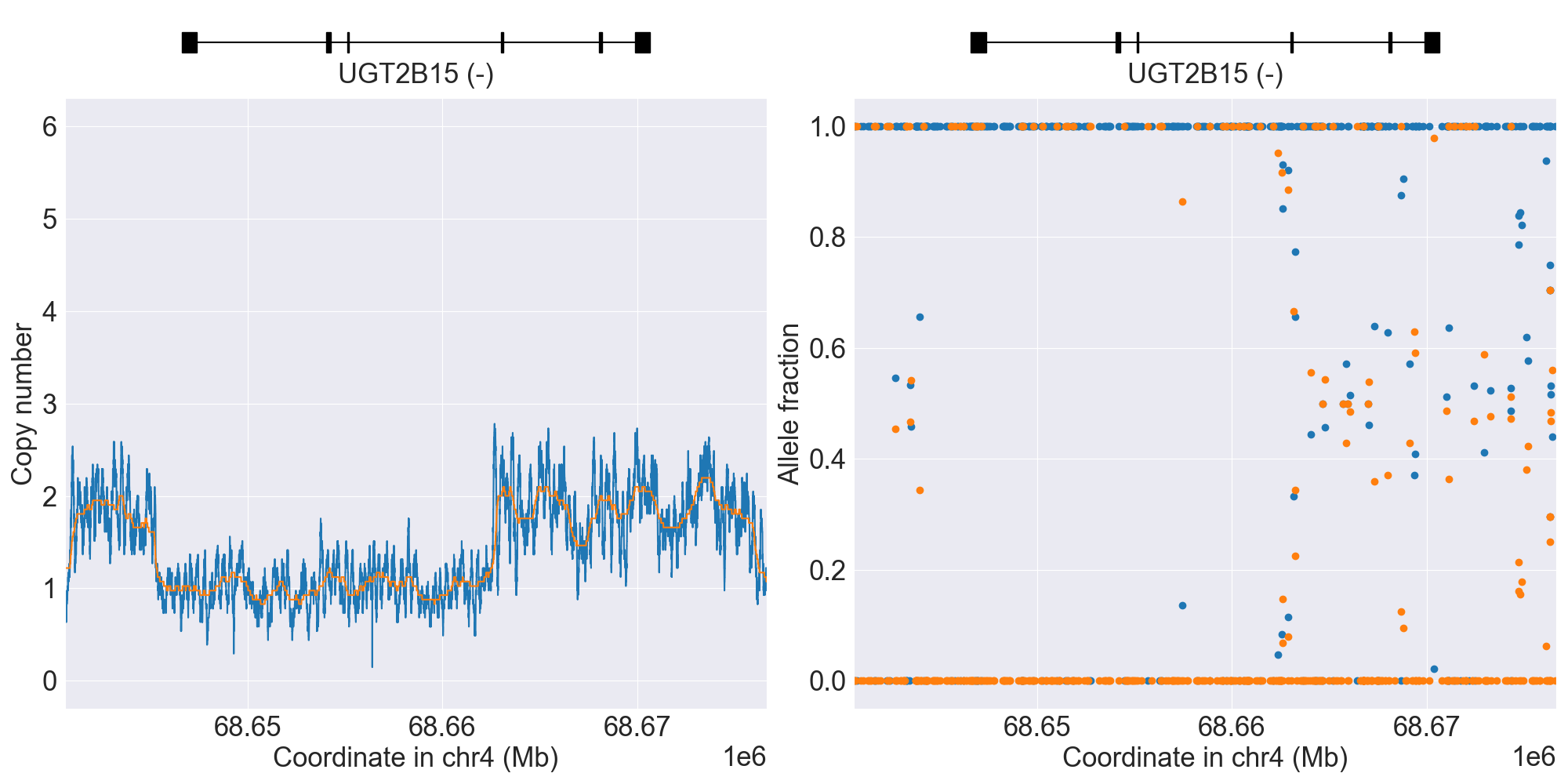
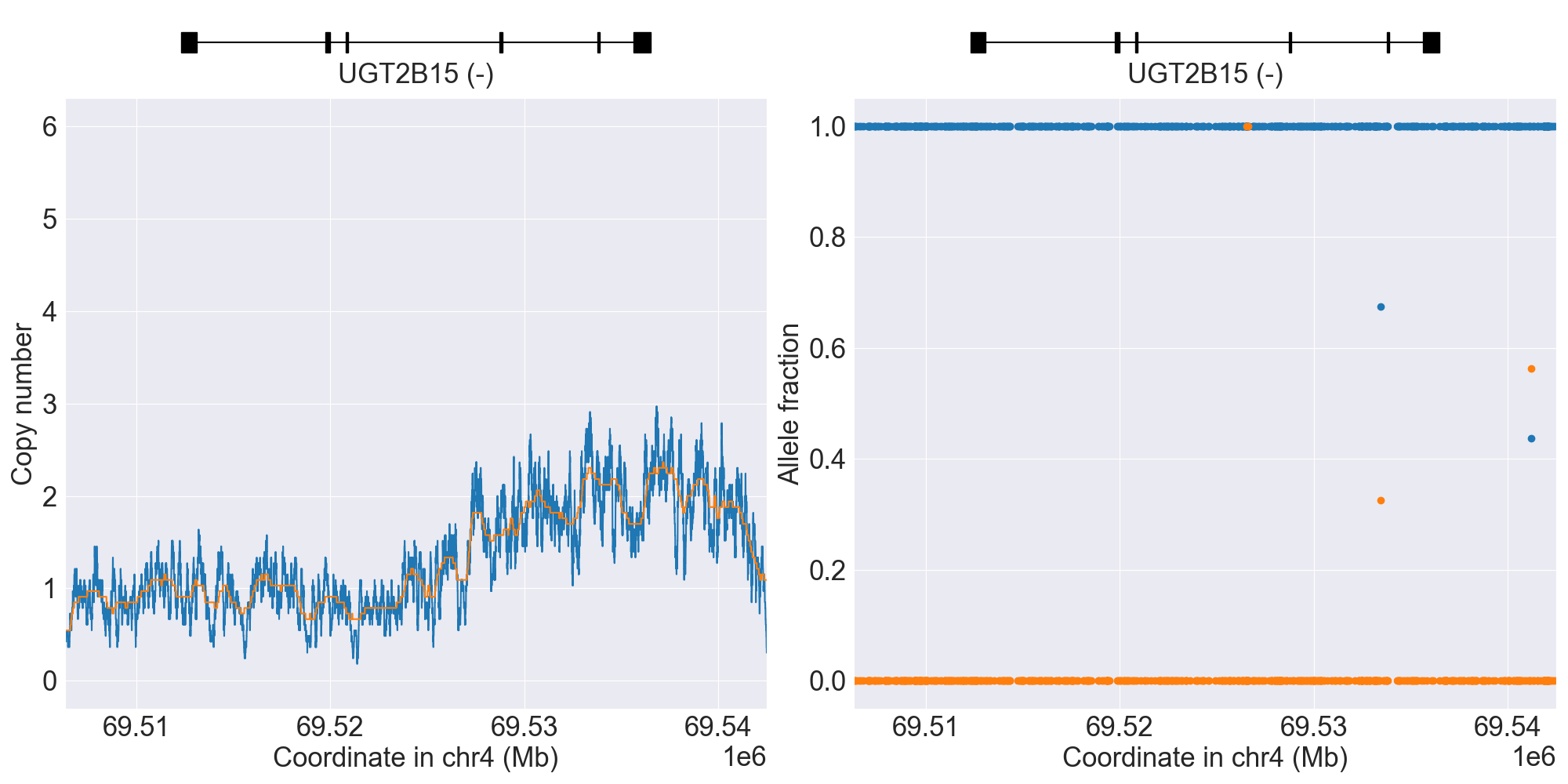
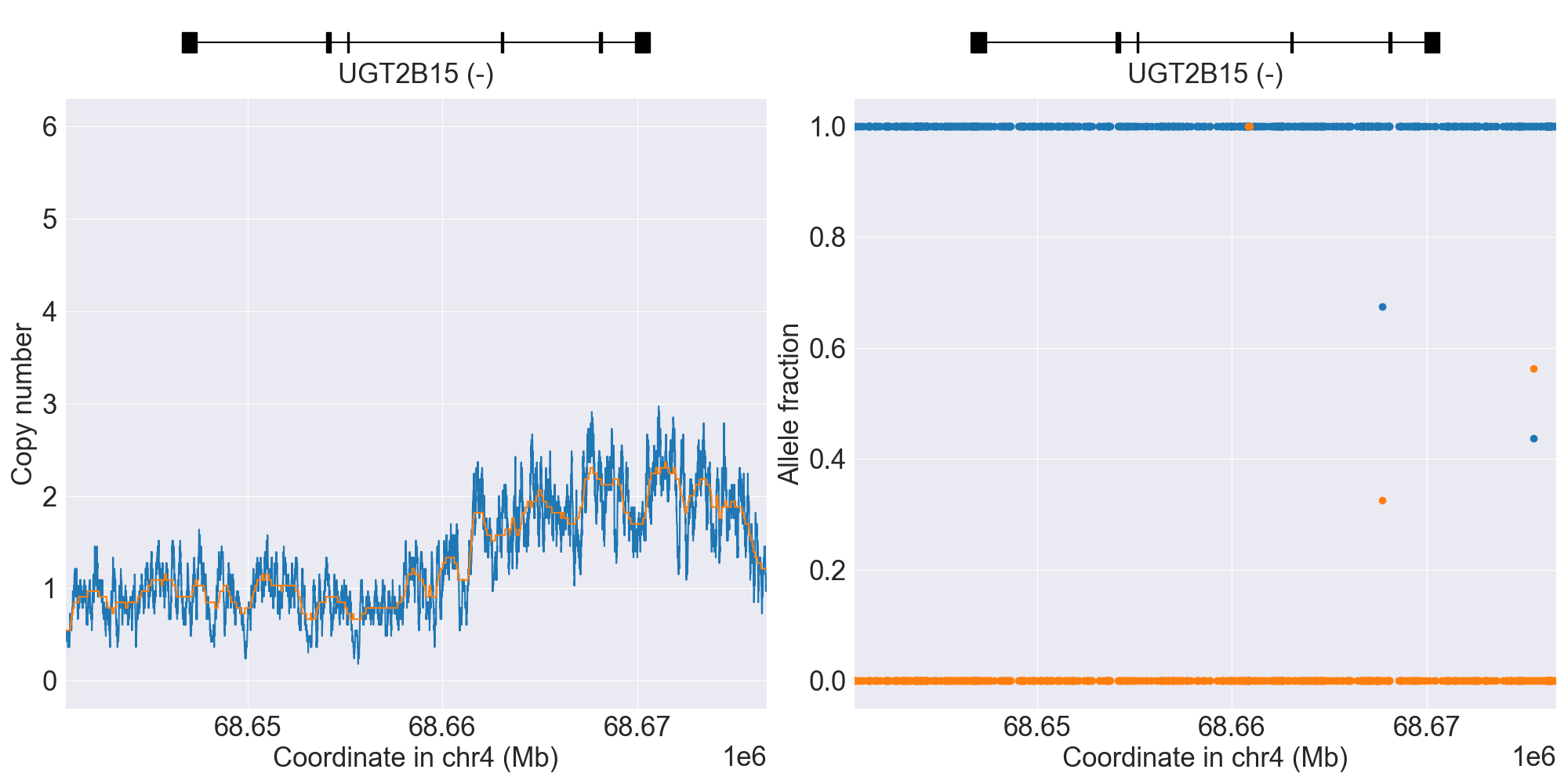
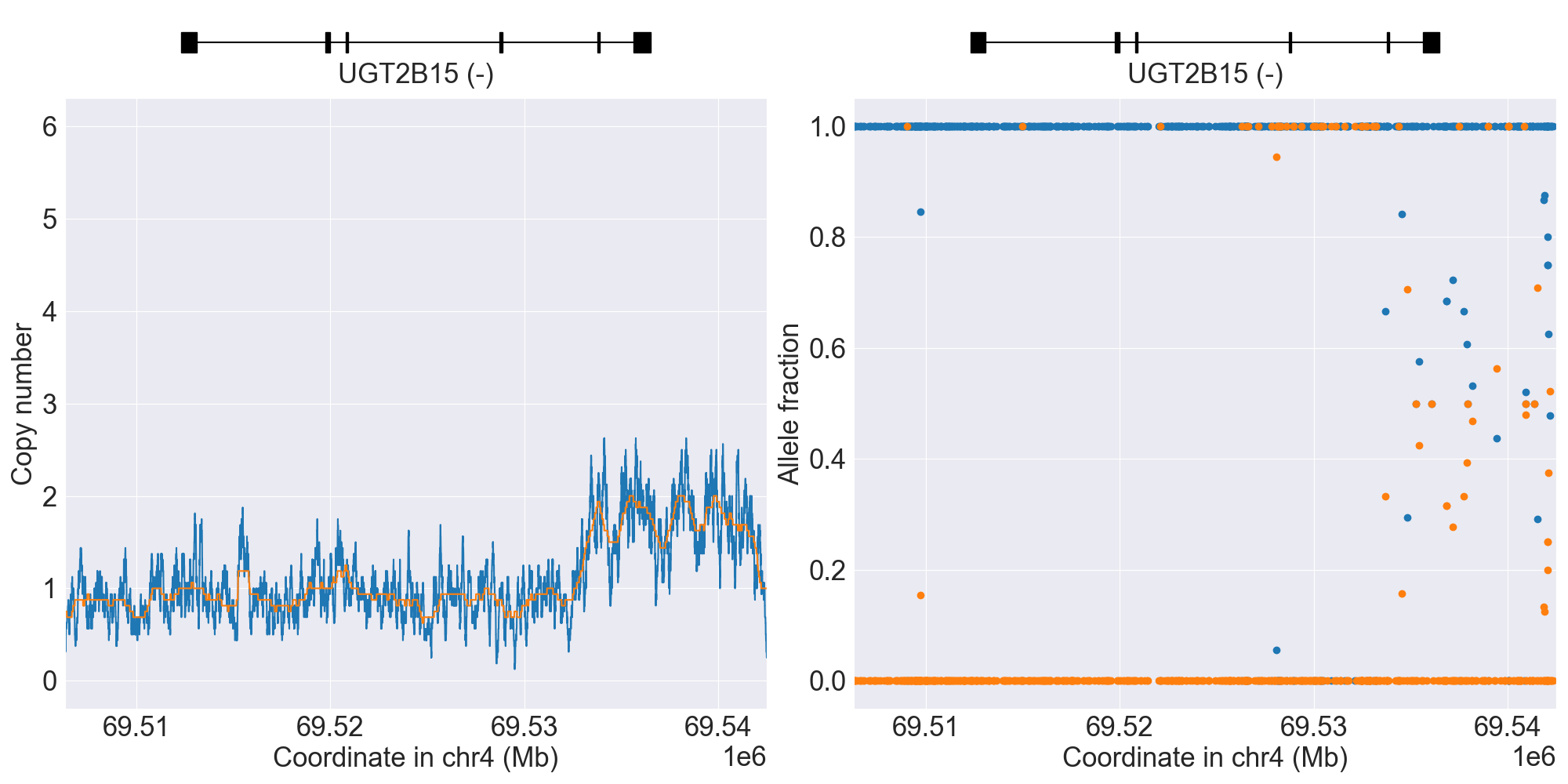
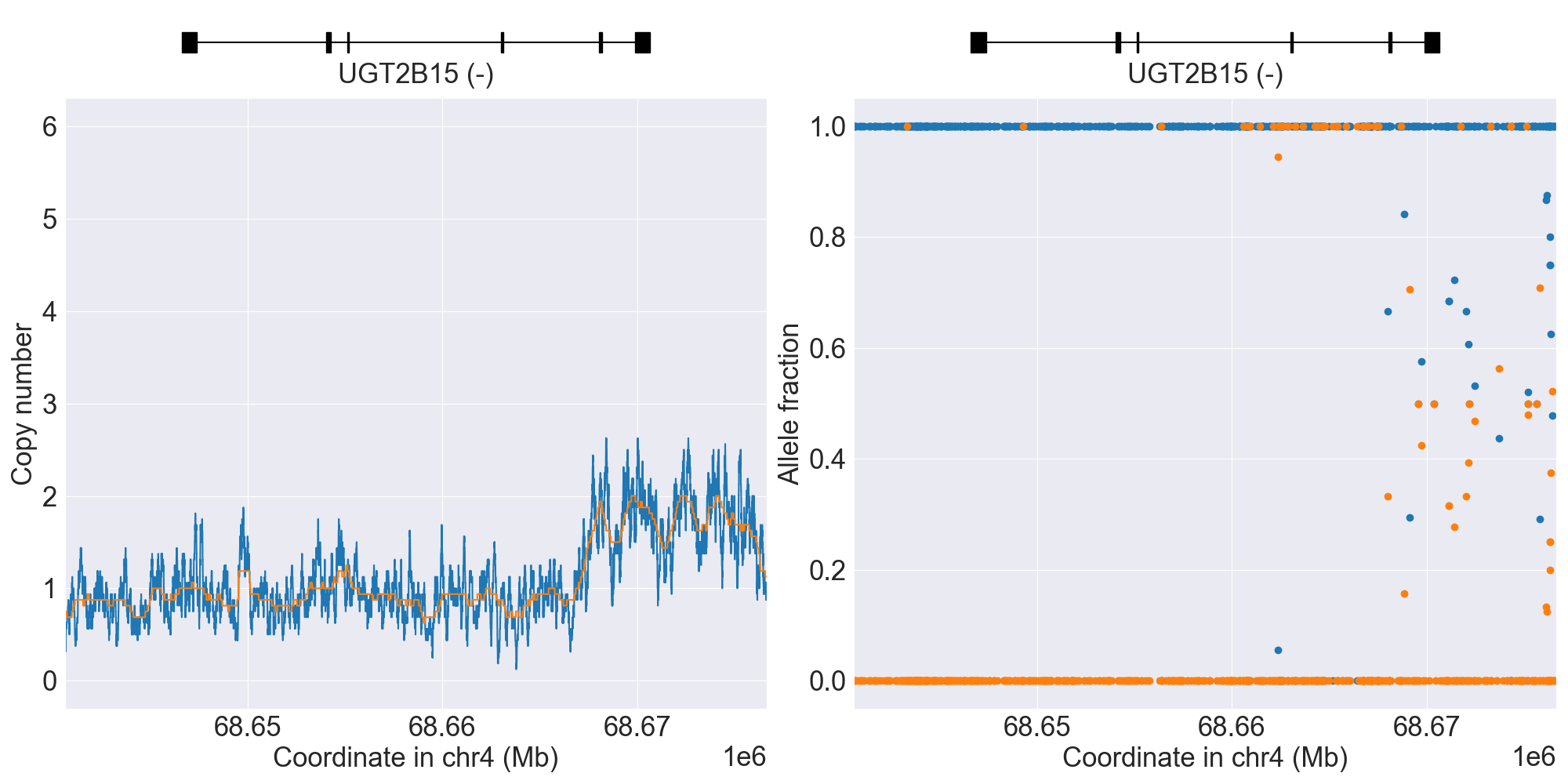
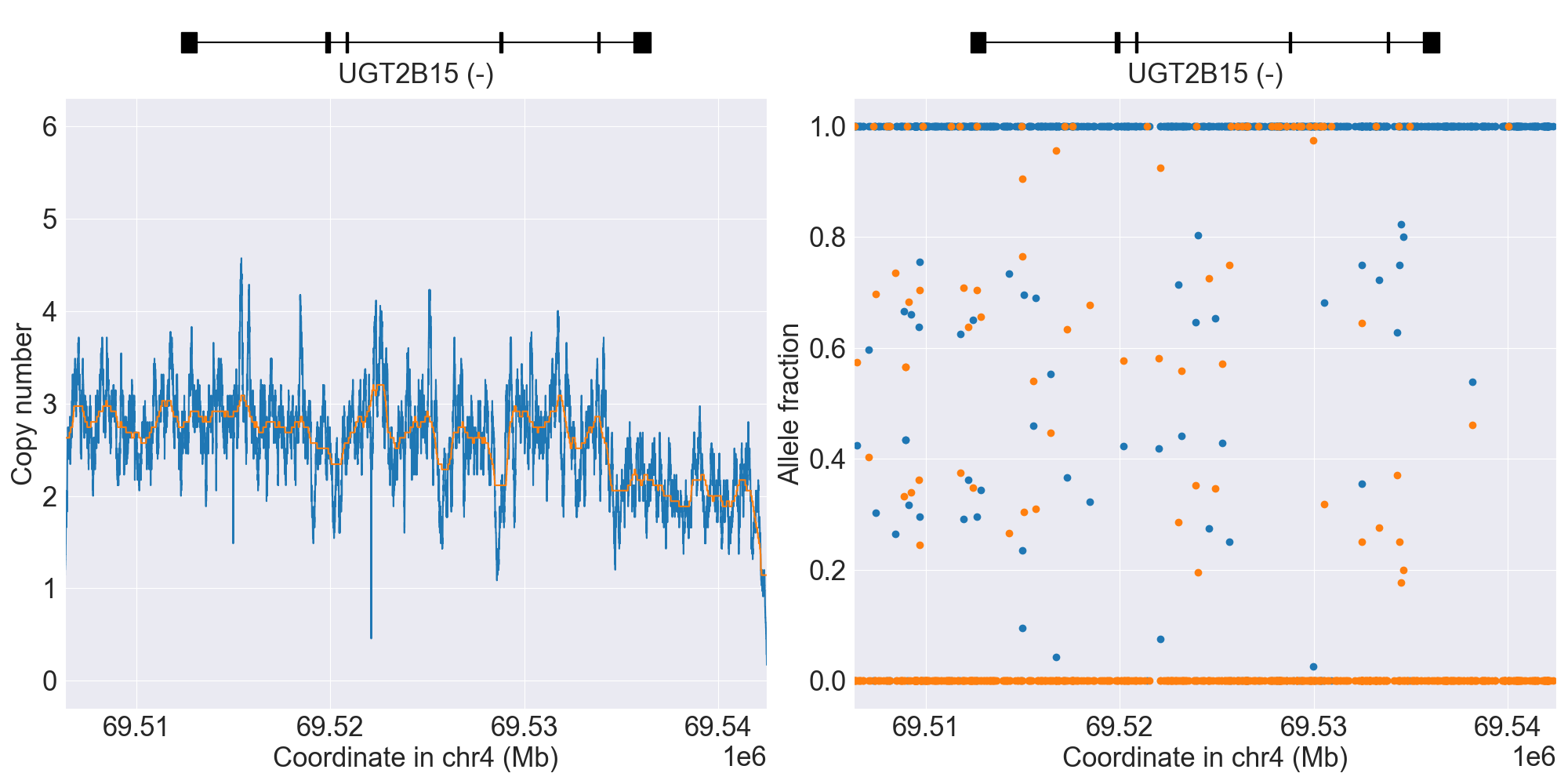
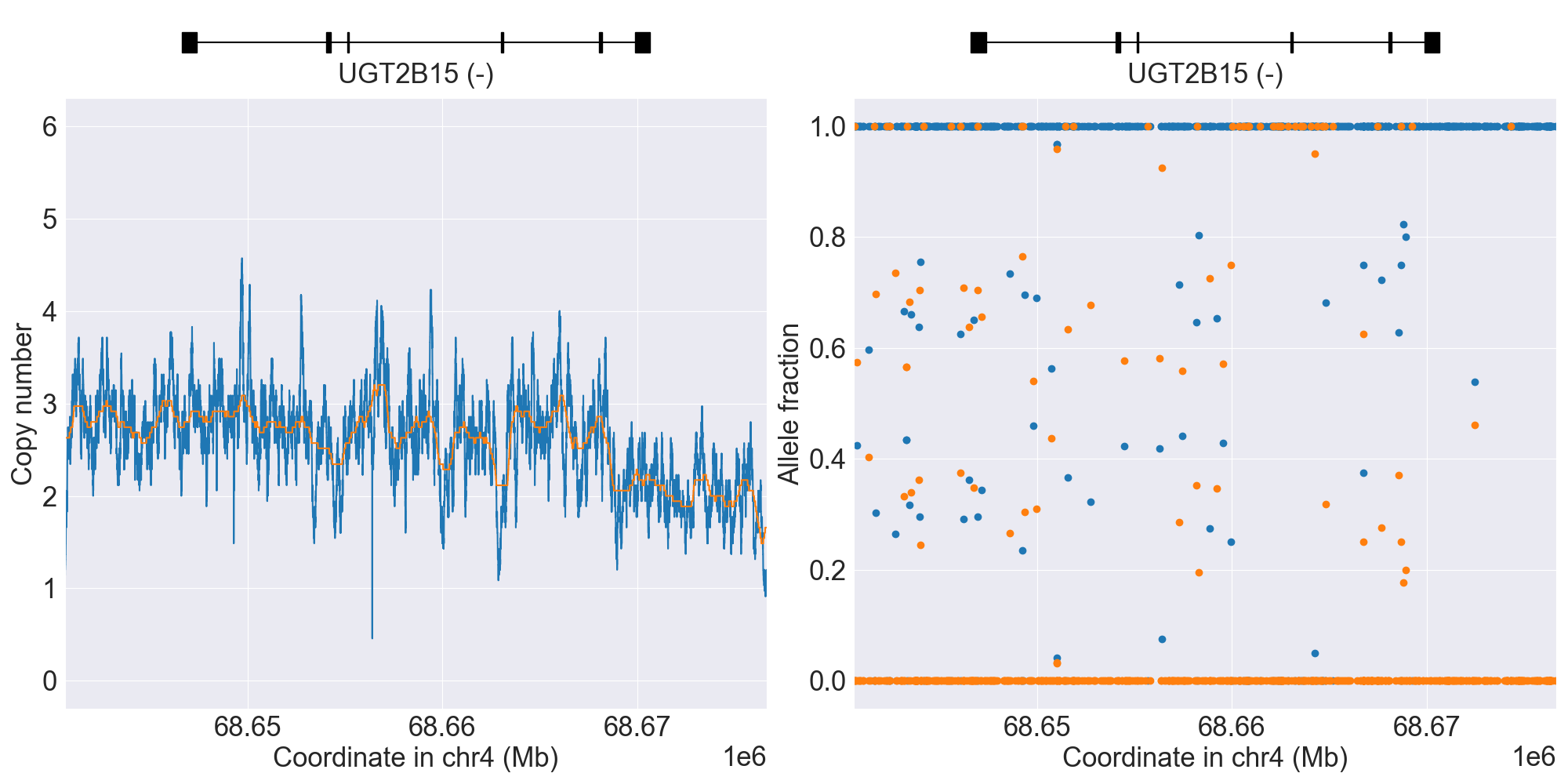
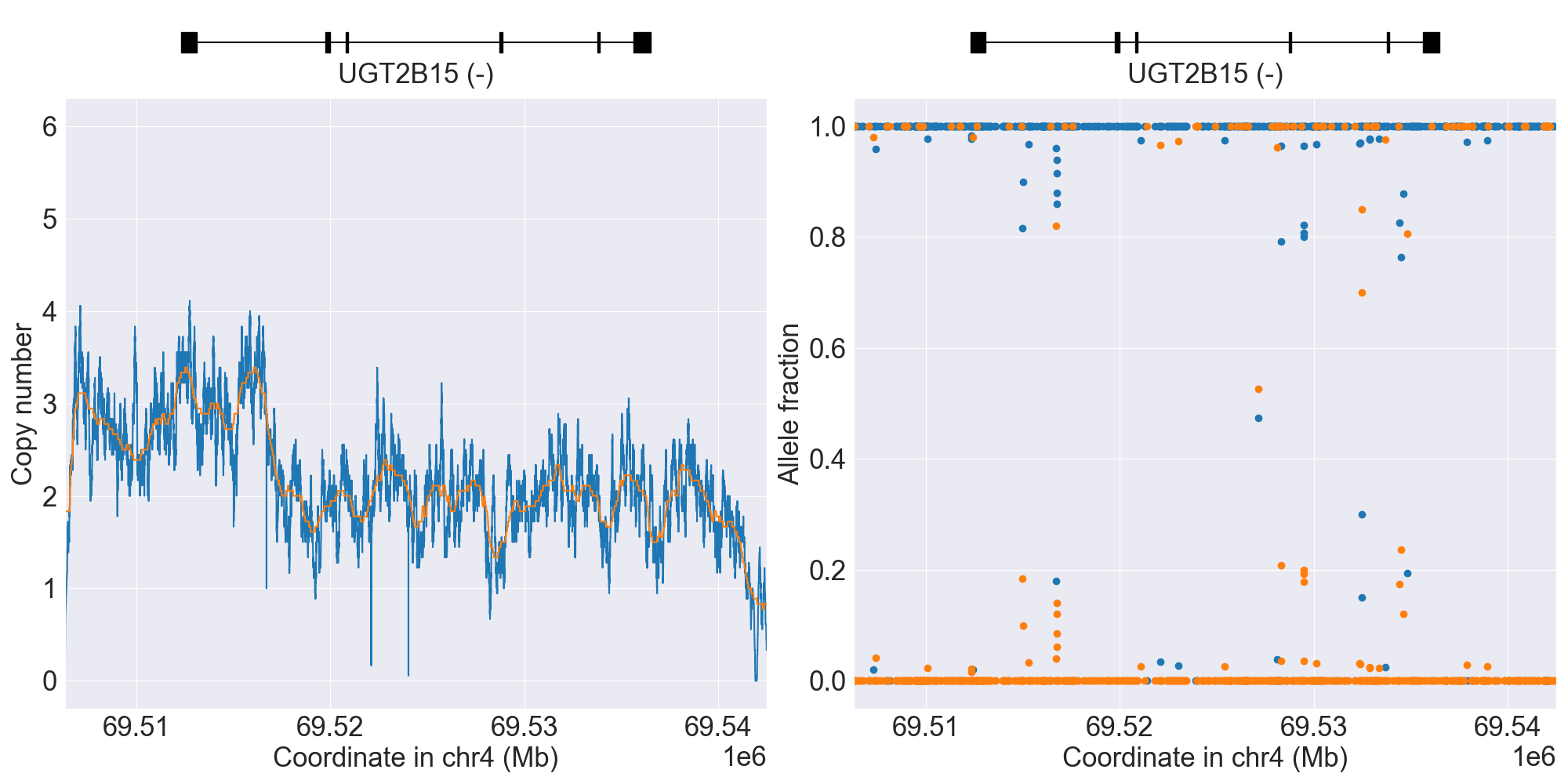
UGT2B15
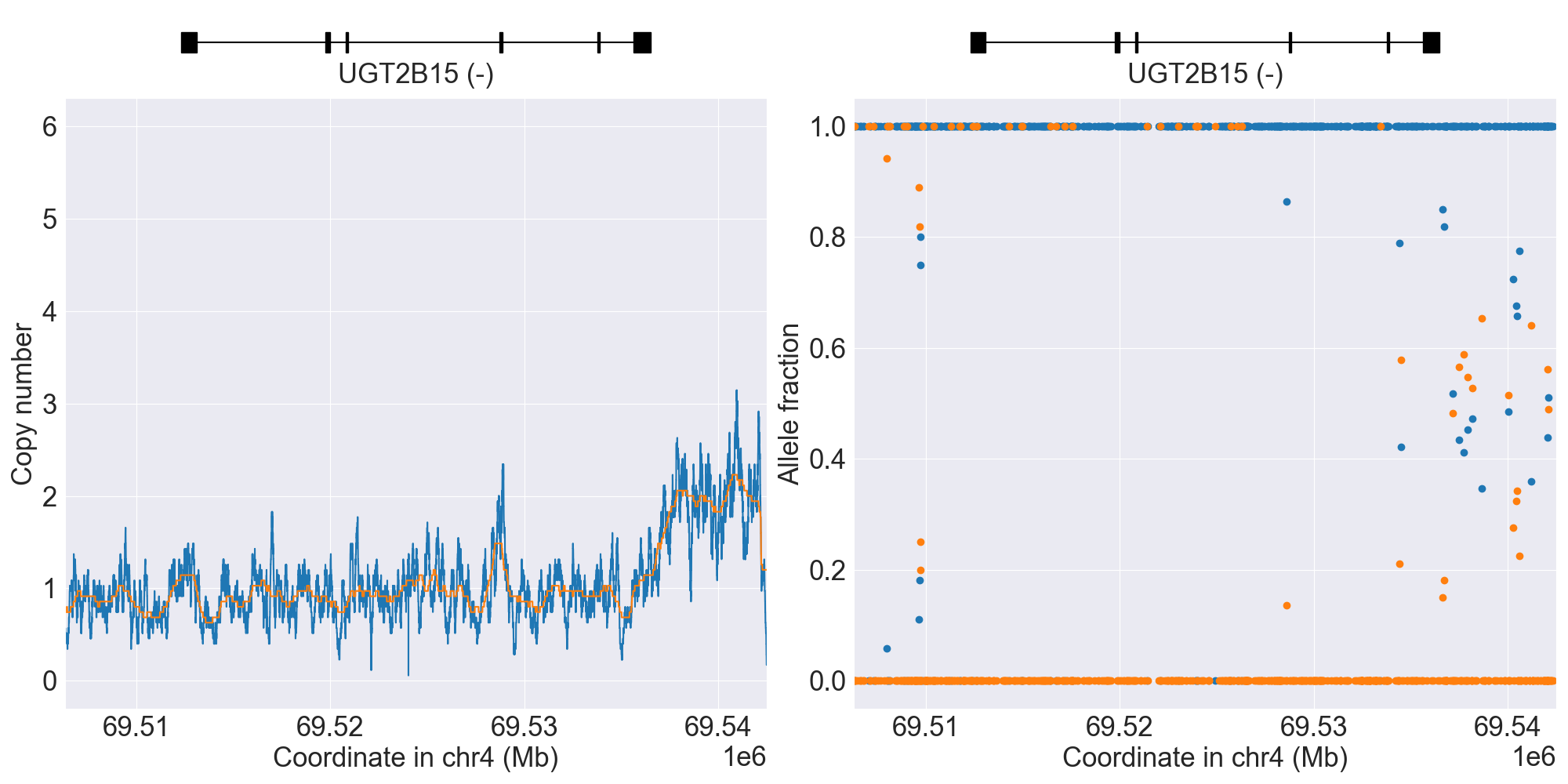
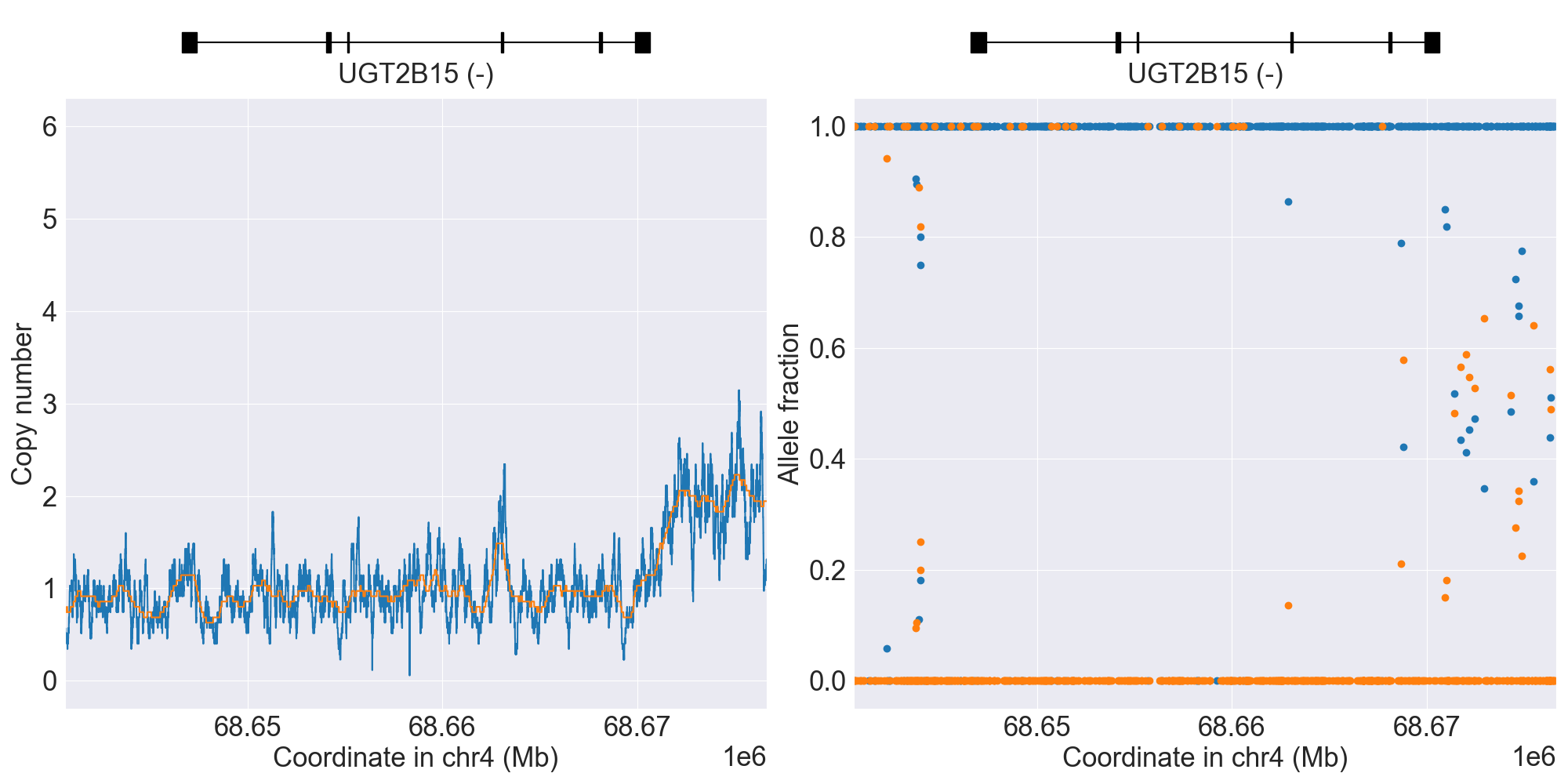
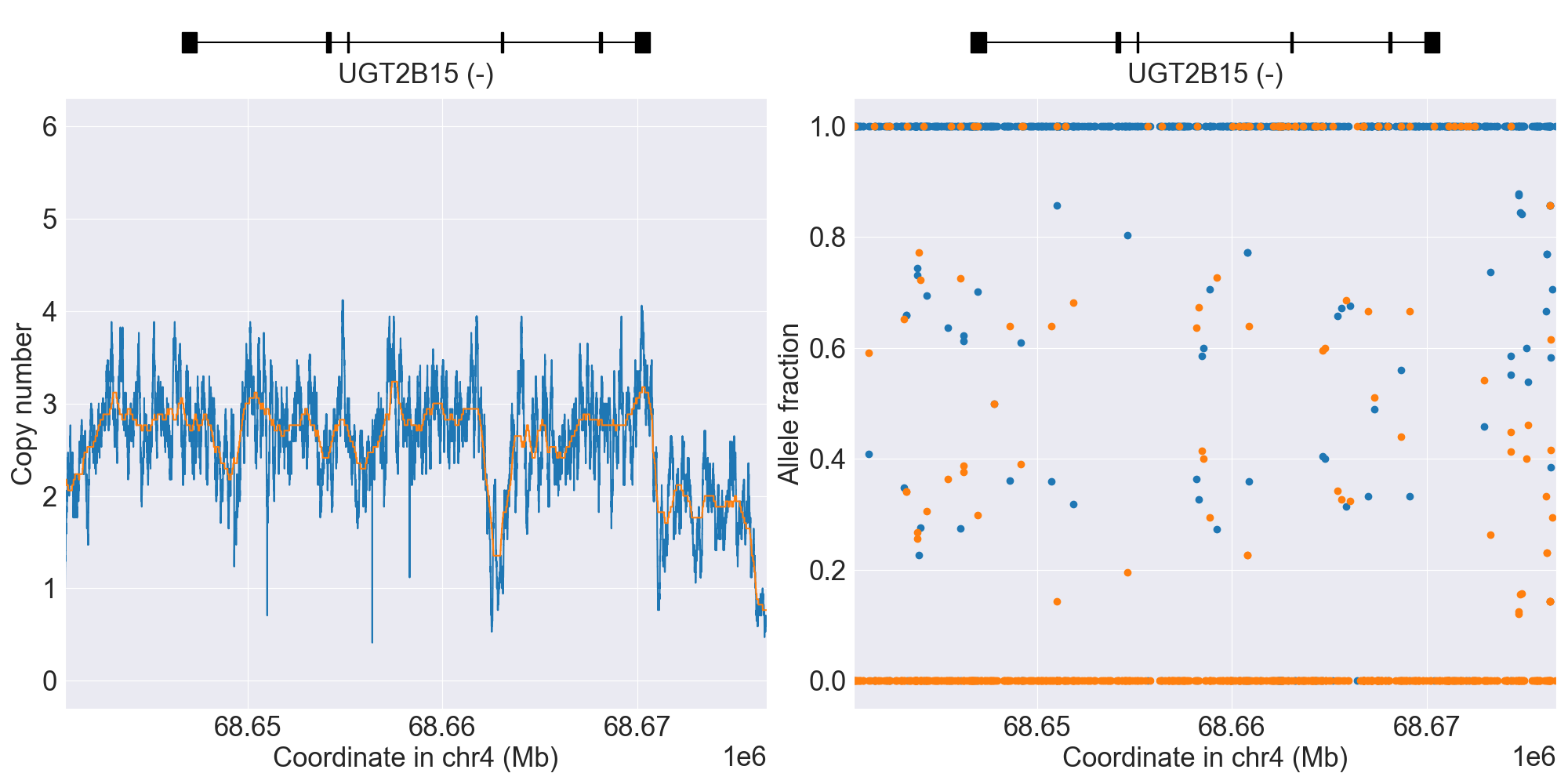
SV summary for UGT2B15
Below is comprehensive summary of SV described from real NGS studies:
SV Alleles |
SV Name |
Genotype |
Reference |
Gene Model |
GRCh37 |
GRCh38 |
Data Type |
Source |
Coriell ID |
Version |
Description |
|---|---|---|---|---|---|---|---|---|---|---|---|
Normal |
*1/*2 |
WGS |
HG00589 |
0.4.1 |
|||||||
*S4 |
WholeDel1 |
*2/*S4 |
WGS |
NA19024 |
0.13.0 |
||||||
WholeDel2 |
Indeterminate |
WGS |
NA19786 |
0.14.0 |
|||||||
WholeDup1 |
Indeterminate |
WGS |
NA19776 |
0.14.0 |
|||||||
*S1 |
PartialDel1 |
*4/*S1 |
WGS |
NA11993 |
0.4.1 |
||||||
*S2 |
PartialDel2 |
*2/*S2 |
WGS |
NA19160 |
0.12.0 |
||||||
*S3 |
PartialDel3 |
*1/*S3 |
WGS |
NA19189 |
0.13.0 |
||||||
PartialDup1 |
Indeterminate |
WGS |
NA20821 |
0.14.0 |
|||||||
PartialDup2 |
Indeterminate |
WGS |
HG03082 |
0.16.0 |
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
PyPGx was recently applied to the entire high-coverage WGS dataset from 1KGP (N=2,504). Click here to see individual SV calls for UGT2B15, and corresponding copy number profiles and allele fraction profiles.
UGT2B17
SV summary for UGT2B17
This gene is known to have an extremely high rate of gene deletion polymorphism in the population and thus requires SV analysis.
Below is comprehensive summary of SV described from real NGS studies:
SV Alleles |
SV Name |
Genotype |
Reference |
Gene Model |
GRCh37 |
GRCh38 |
Data Type |
Source |
Coriell ID |
Version |
Description |
|---|---|---|---|---|---|---|---|---|---|---|---|
Normal |
*1/*1 |
WGS |
NA19178 |
0.4.1 |
|||||||
*2 |
WholeDel1 |
*1/*2 |
WGS |
NA18855 |
0.4.1 |
||||||
*2 |
WholeDel1Hom |
*2/*2 |
WGS |
NA18617 |
0.4.1 |
||||||
*S2 |
PartialDel2 |
*1/*S2 |
WGS |
HG03127 |
0.16.0 |
||||||
*S3 |
PartialDel3 |
*1/*S3 |
WGS |
NA20886 |
0.14.0 |
||||||
*2, *S1 |
WholeDel1+PartialDel1 |
*2/*S1 |
WGS |
NA19160 |
0.12.0 |
||||||
*2, *S2 |
WholeDel1+PartialDel2 |
*2/*S2 |
WGS |
NA19189 |
0.13.0 |
||||||
*2, *S3 |
WholeDel1+PartialDel3 |
*2/*S3 |
WGS |
NA21090 |
0.15.0 |
{kind=link}
{kind=link}
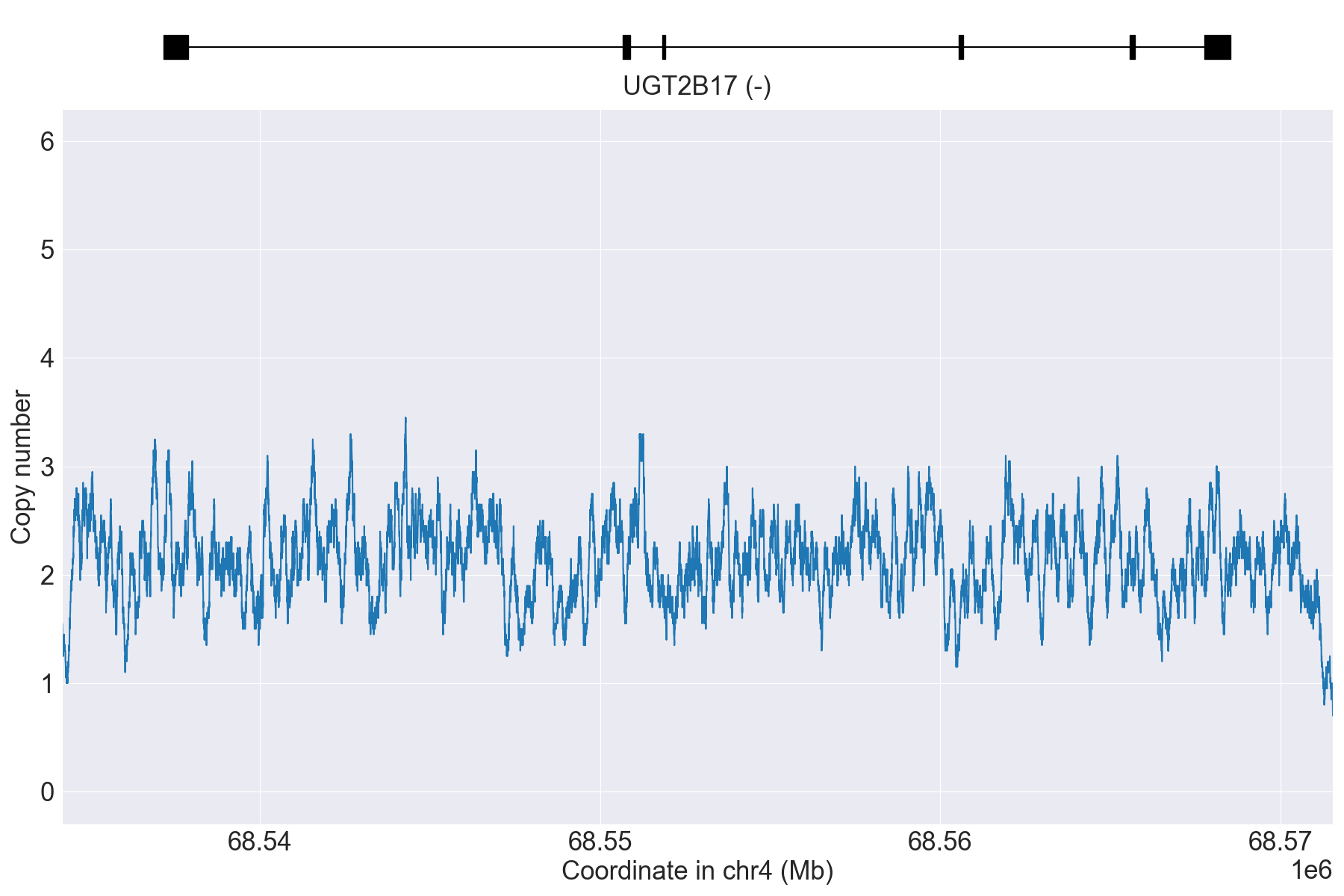{kind=link}
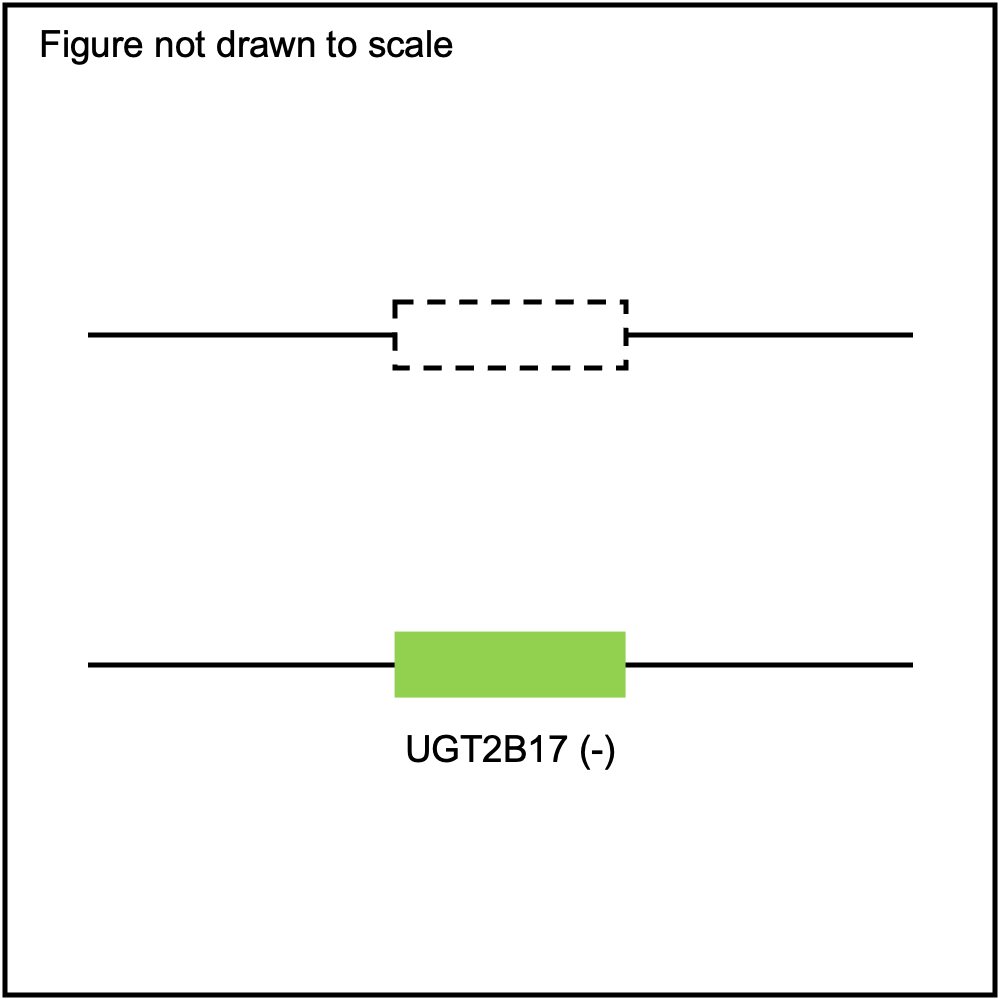{kind=link}
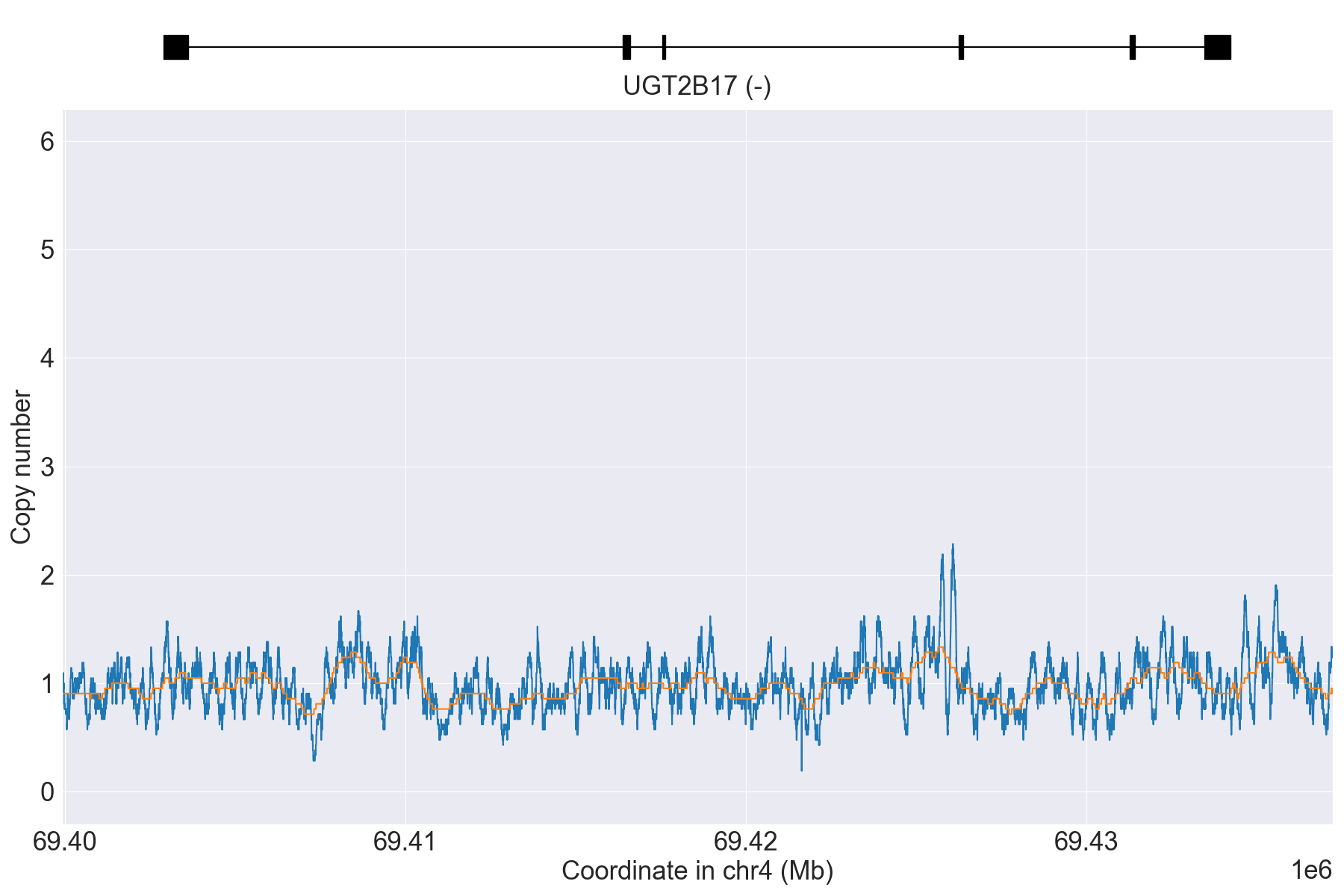{kind=link}
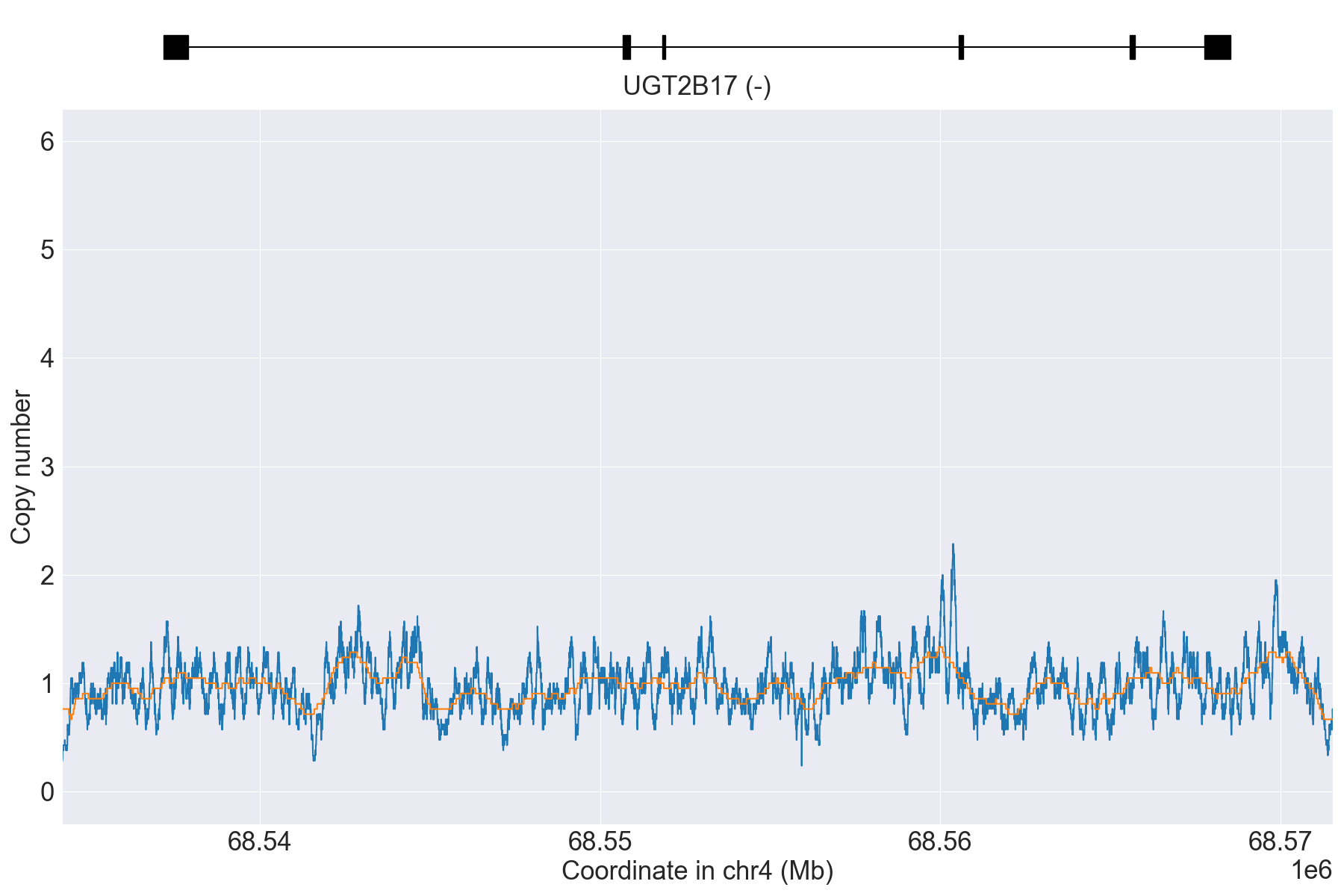{kind=link}
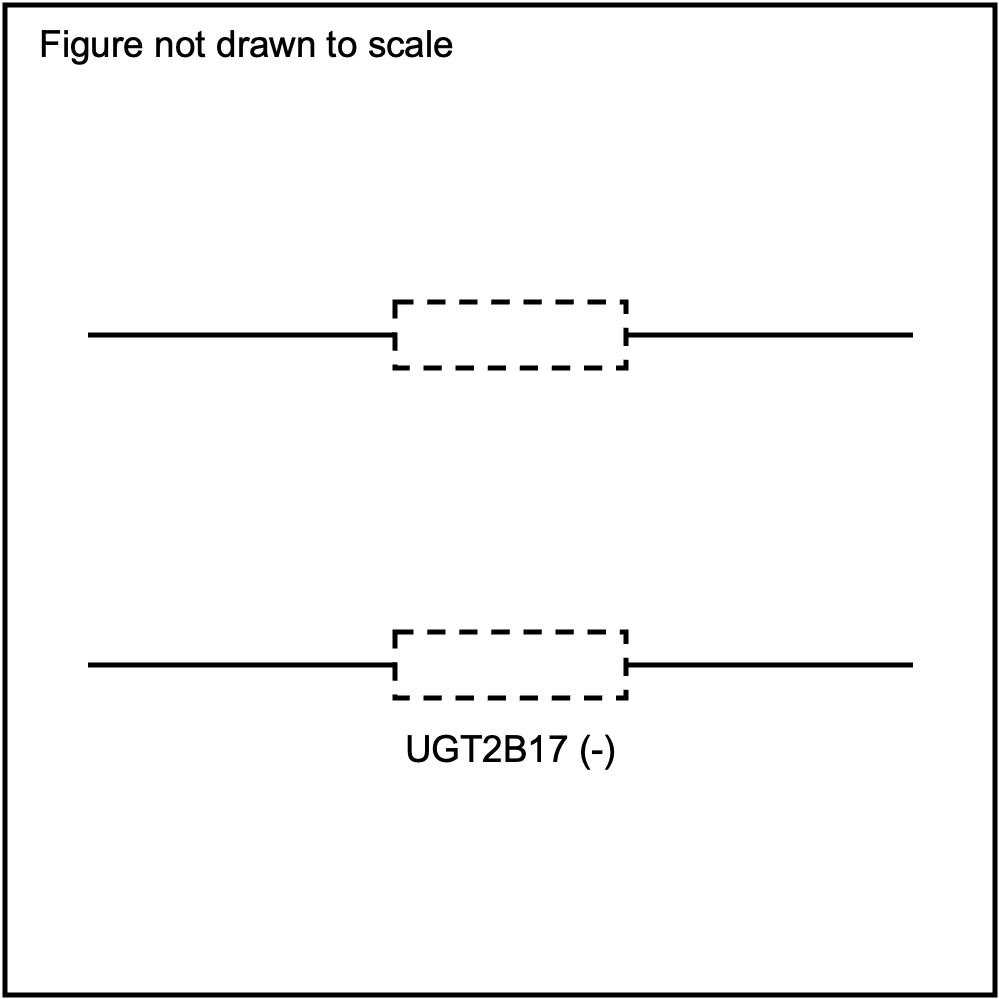{kind=link}
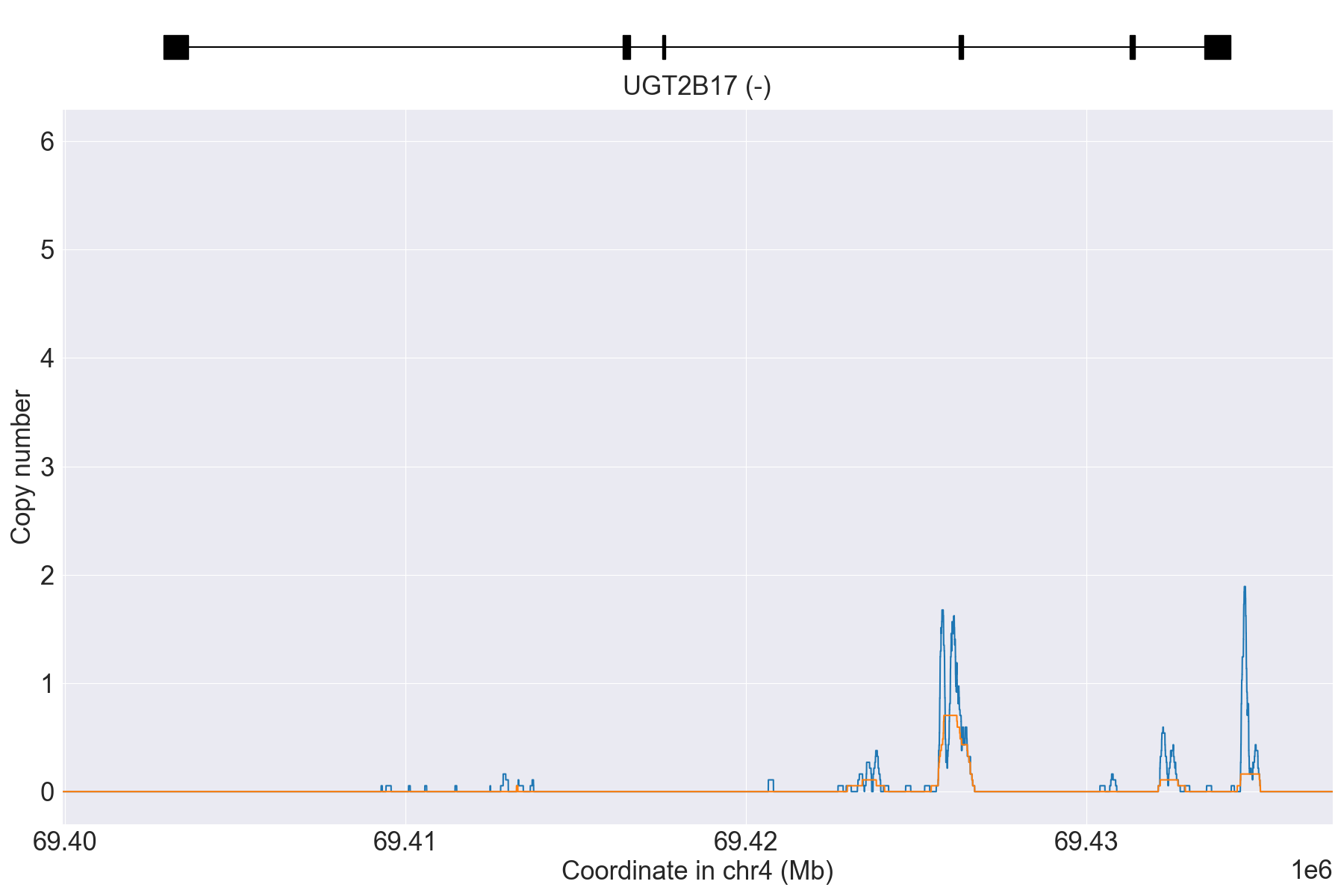{kind=link}
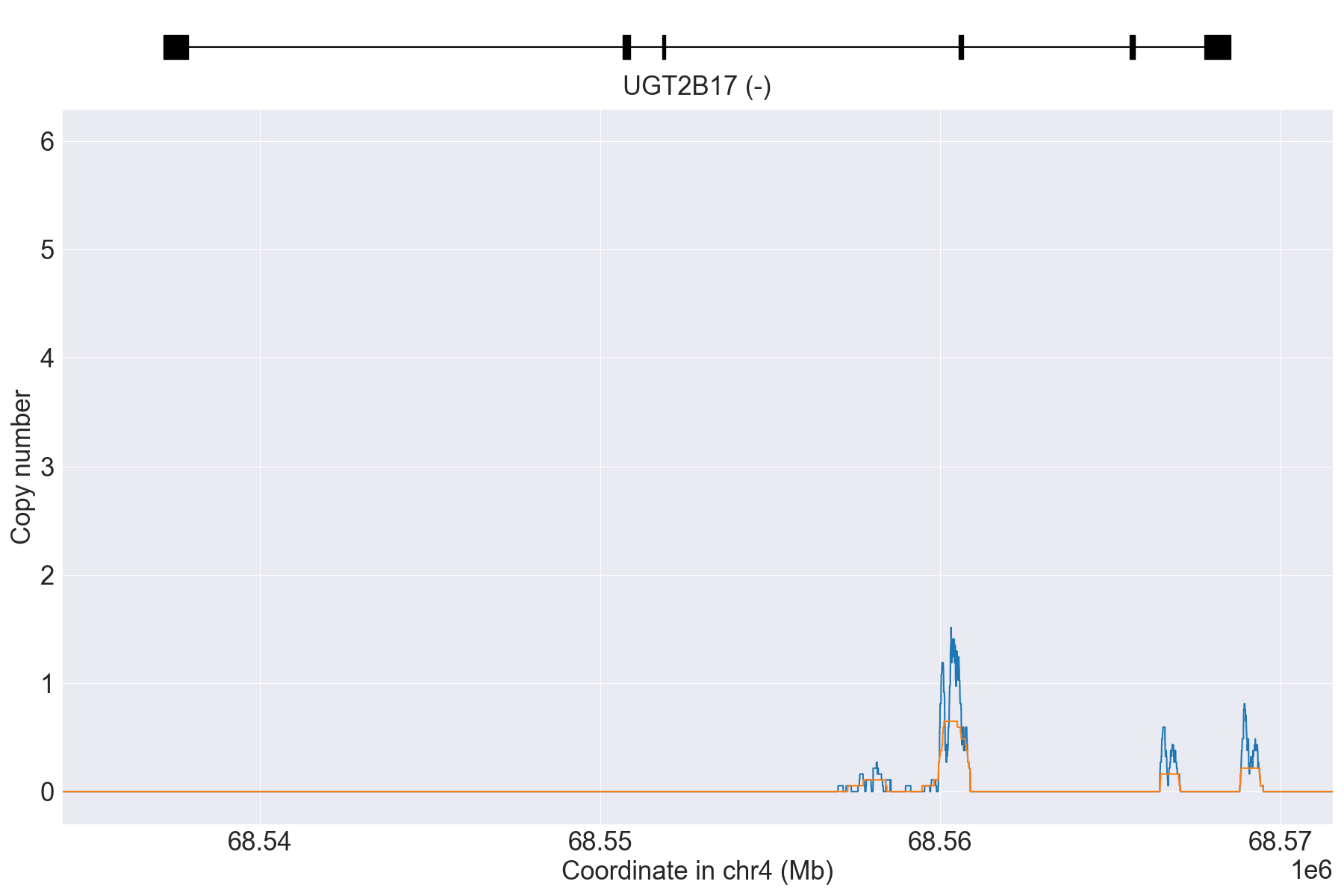{kind=link}
{kind=link}
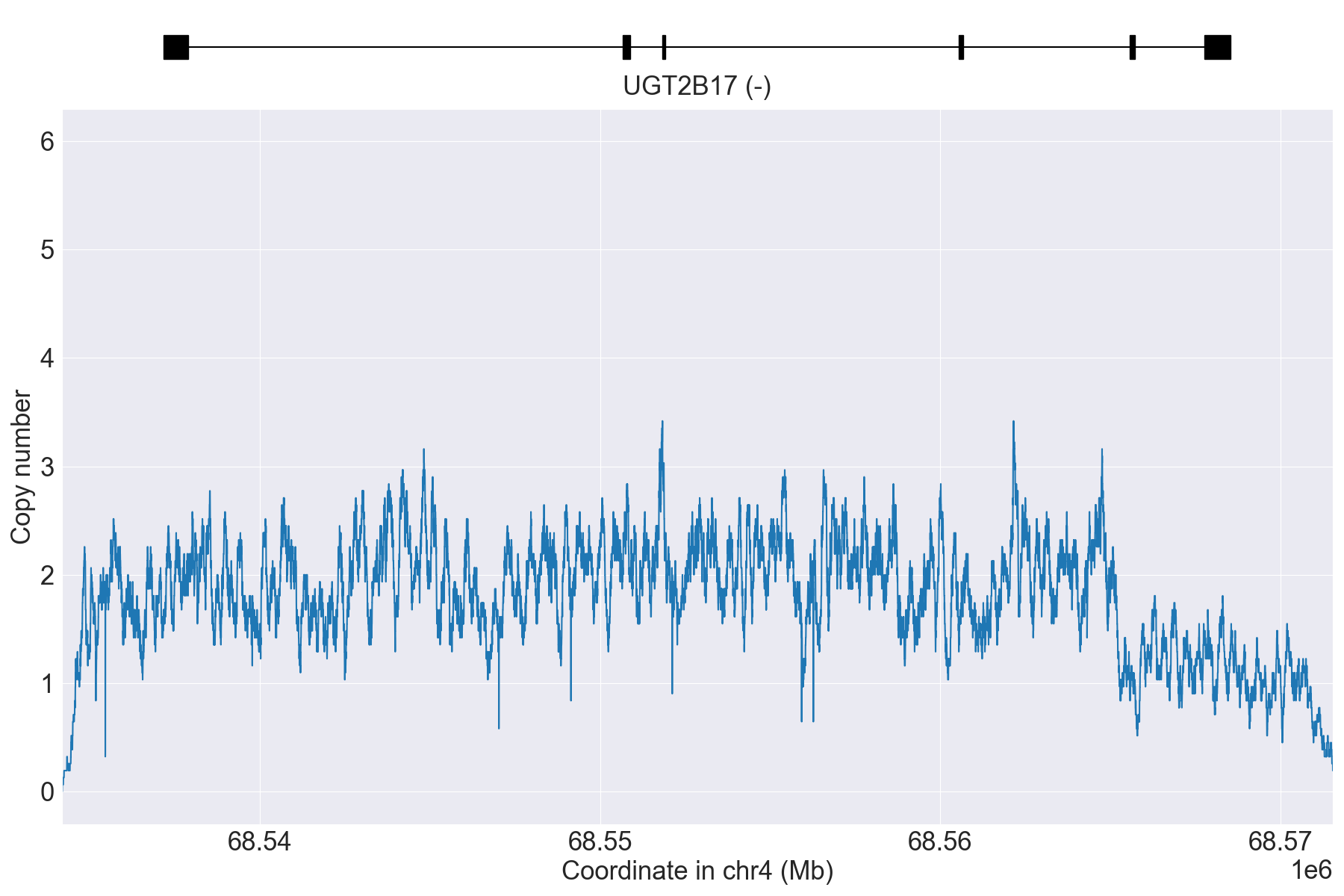{kind=link}
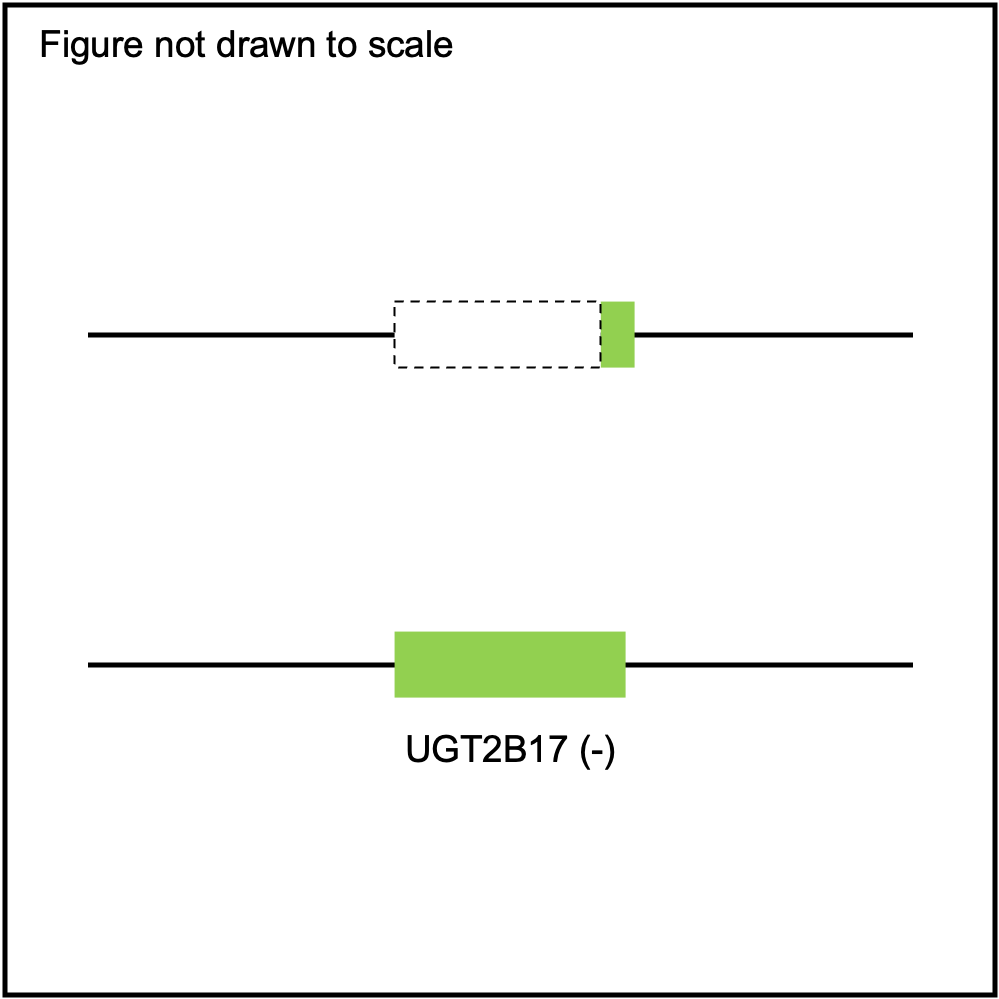{kind=link}
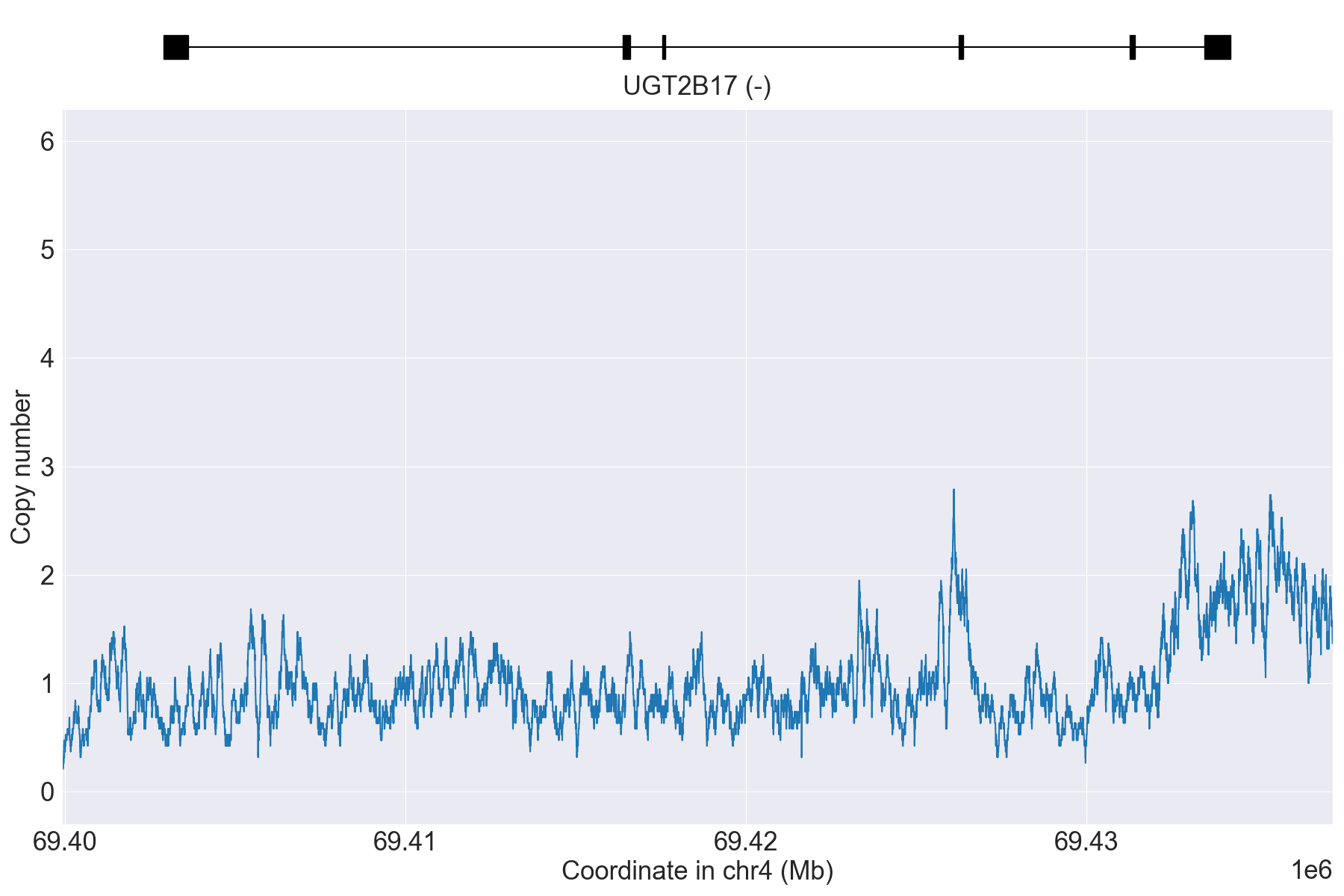{kind=link}
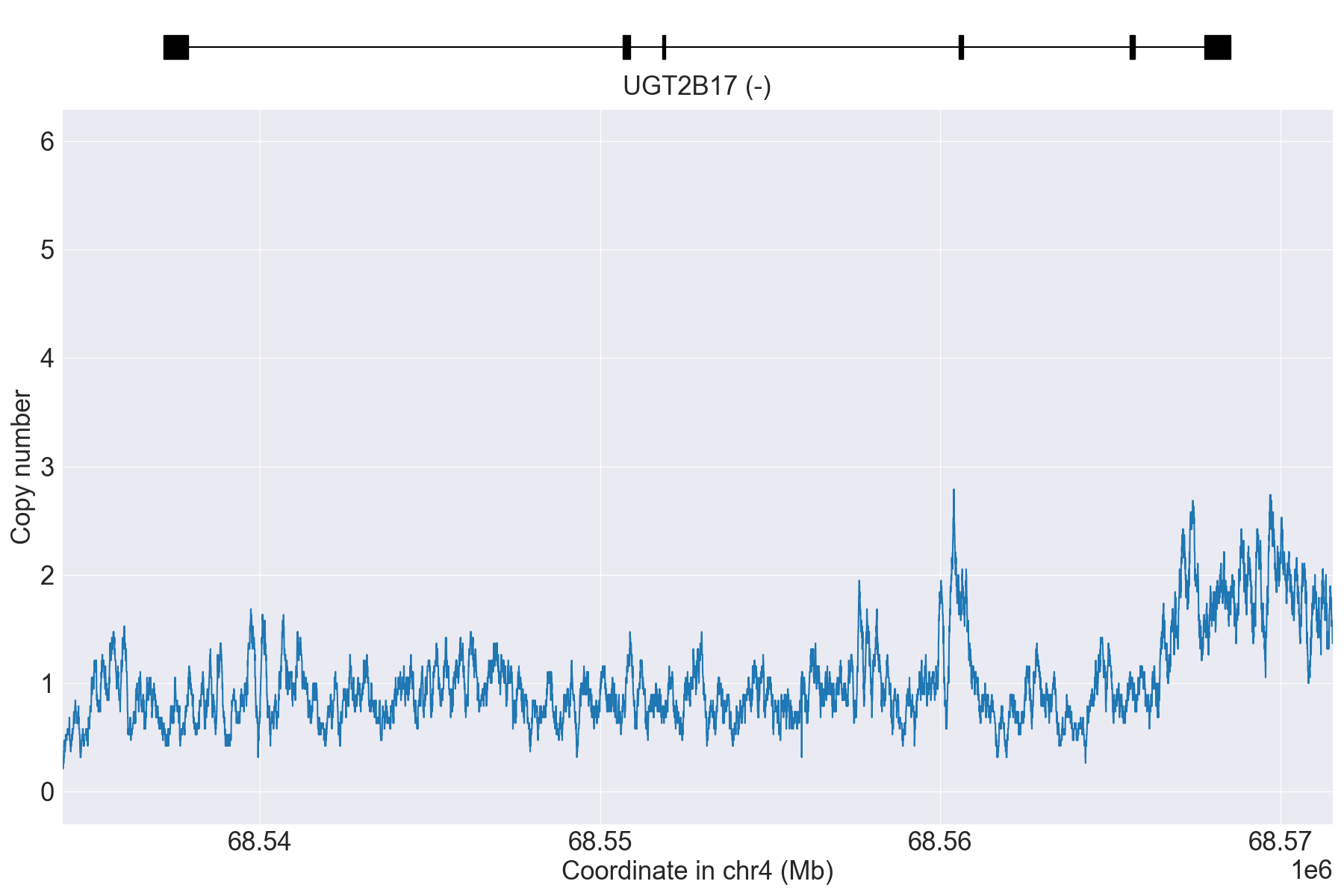{kind=link}
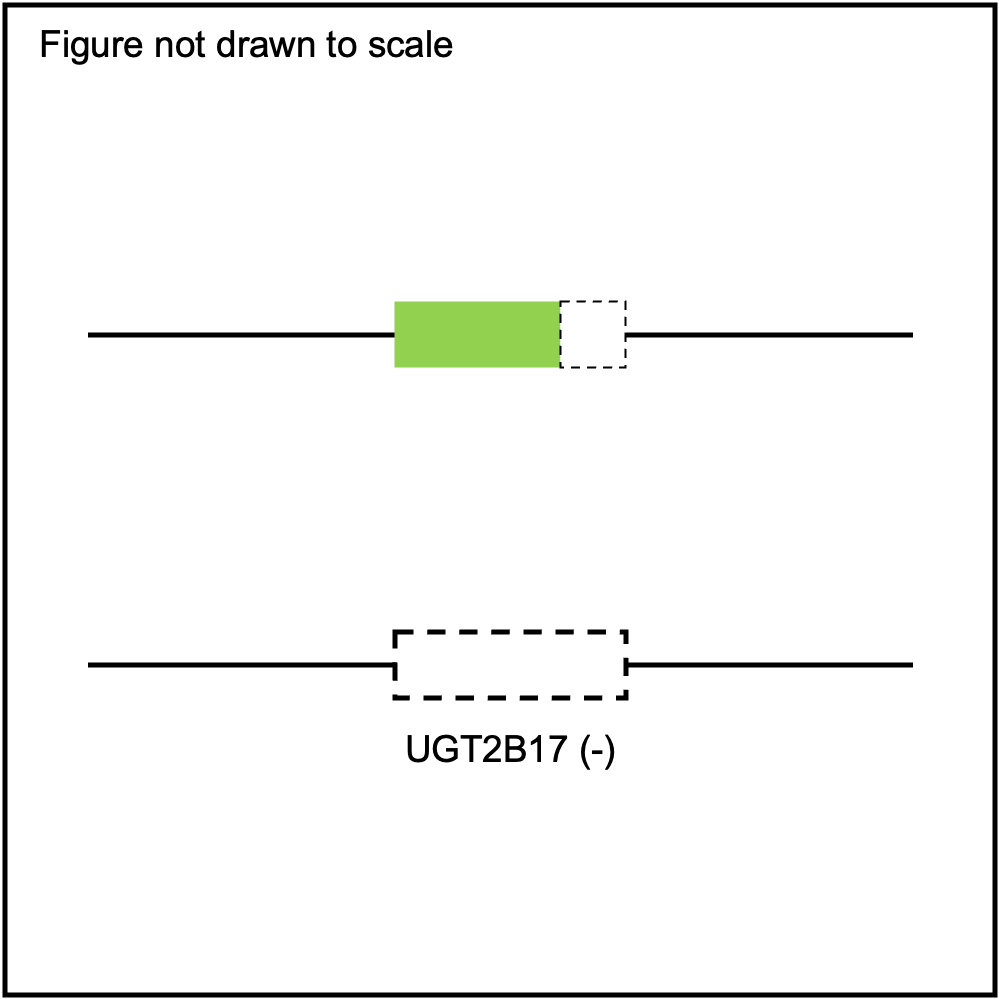{kind=link}
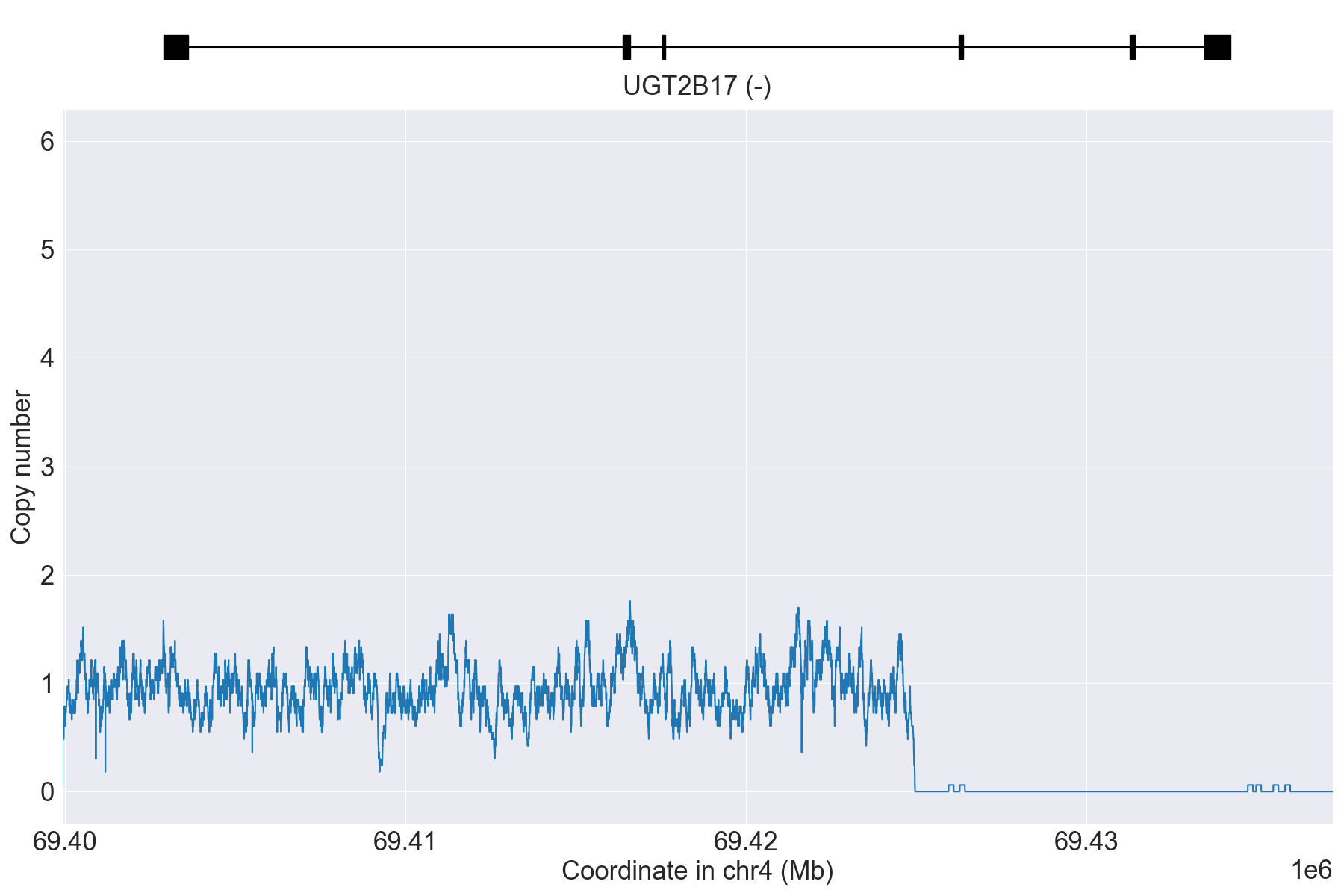{kind=link}
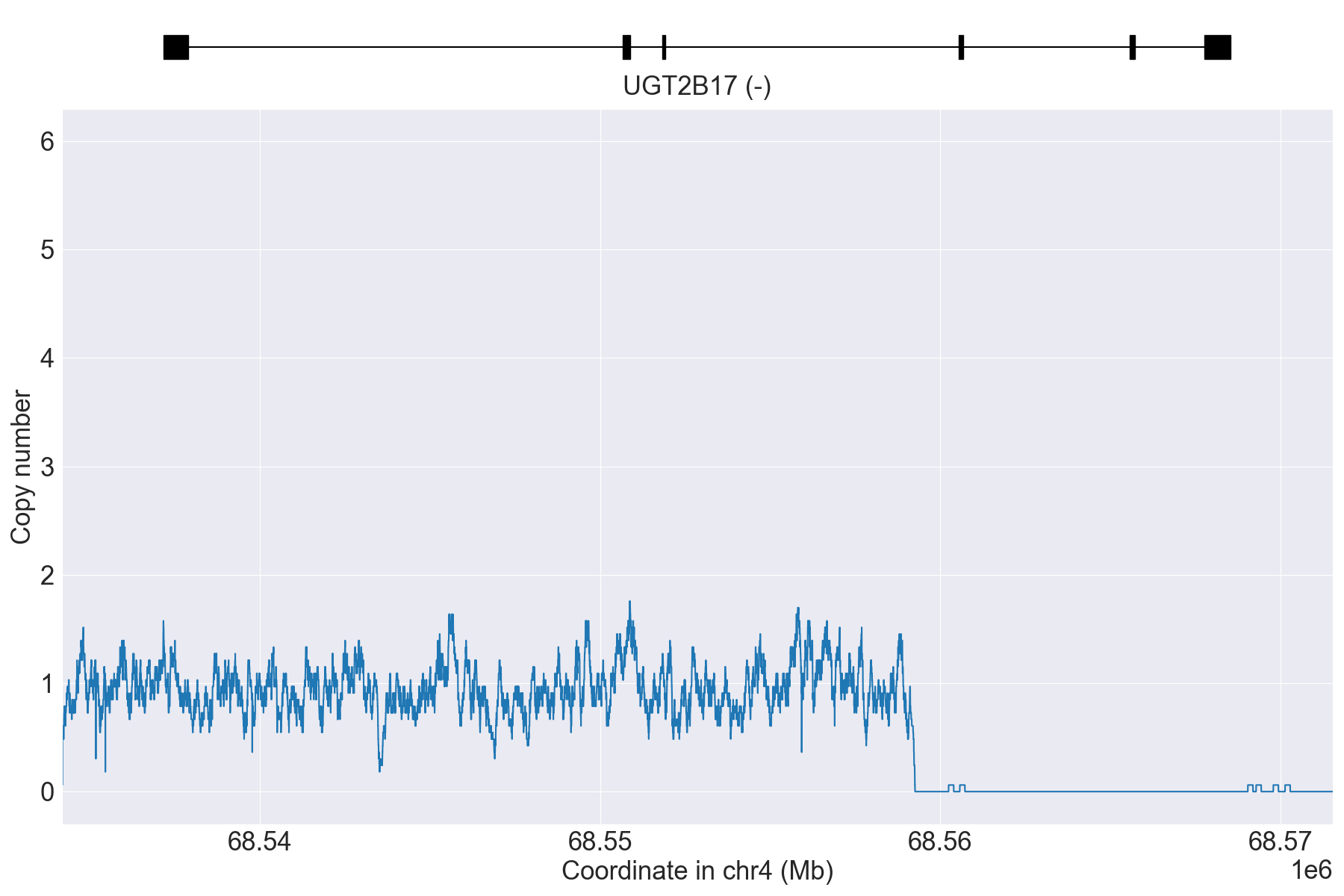{kind=link}
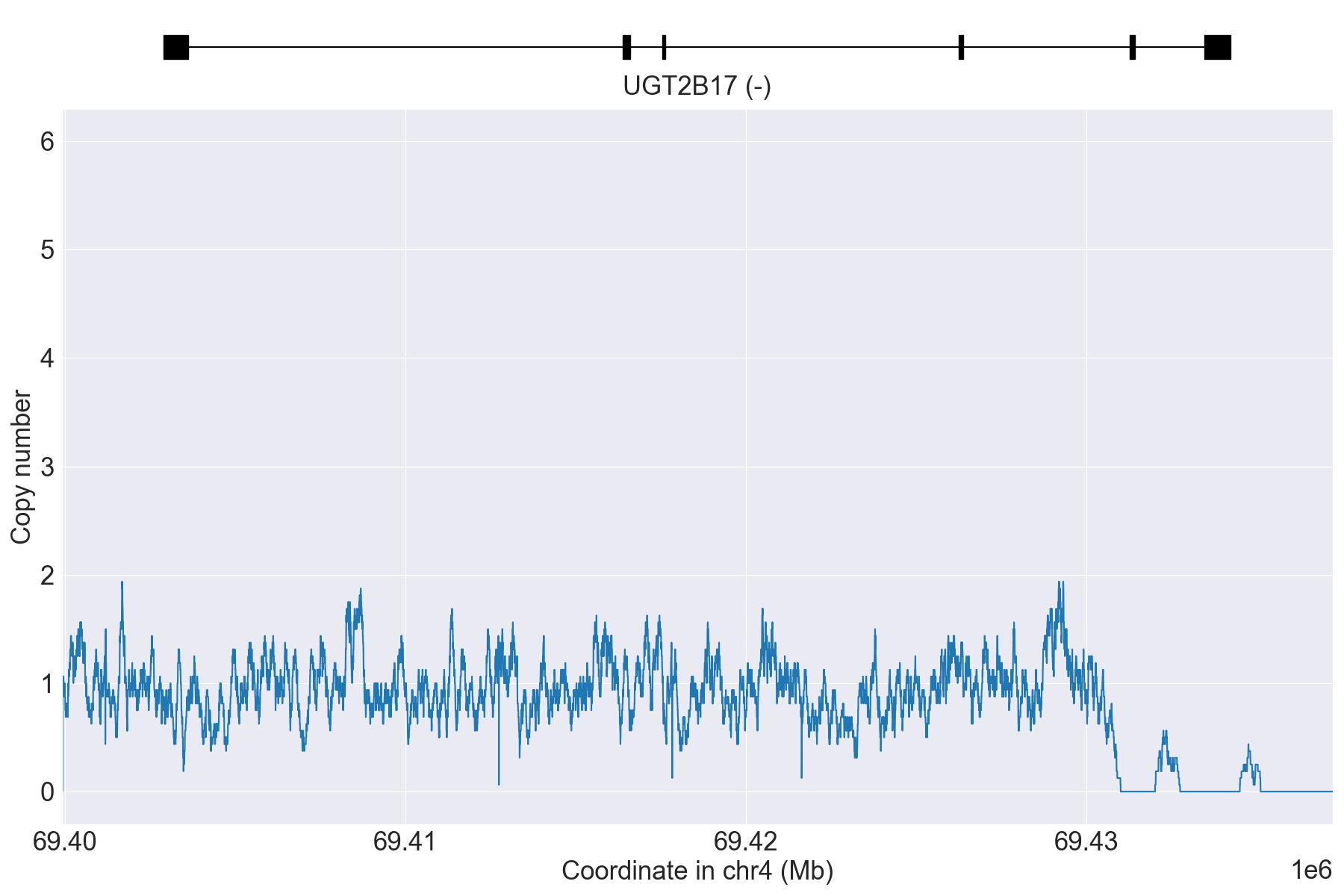{kind=link}
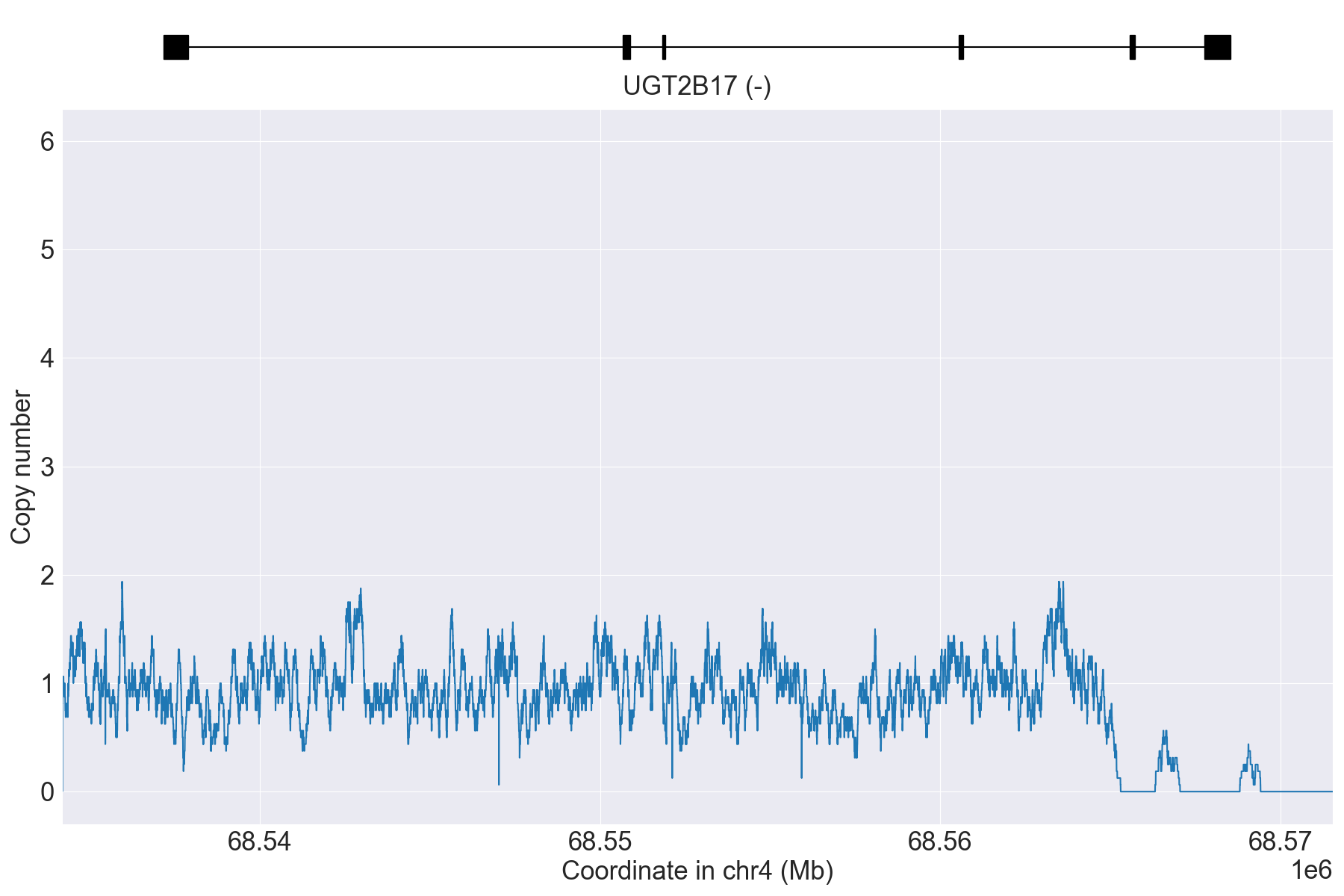{kind=link}
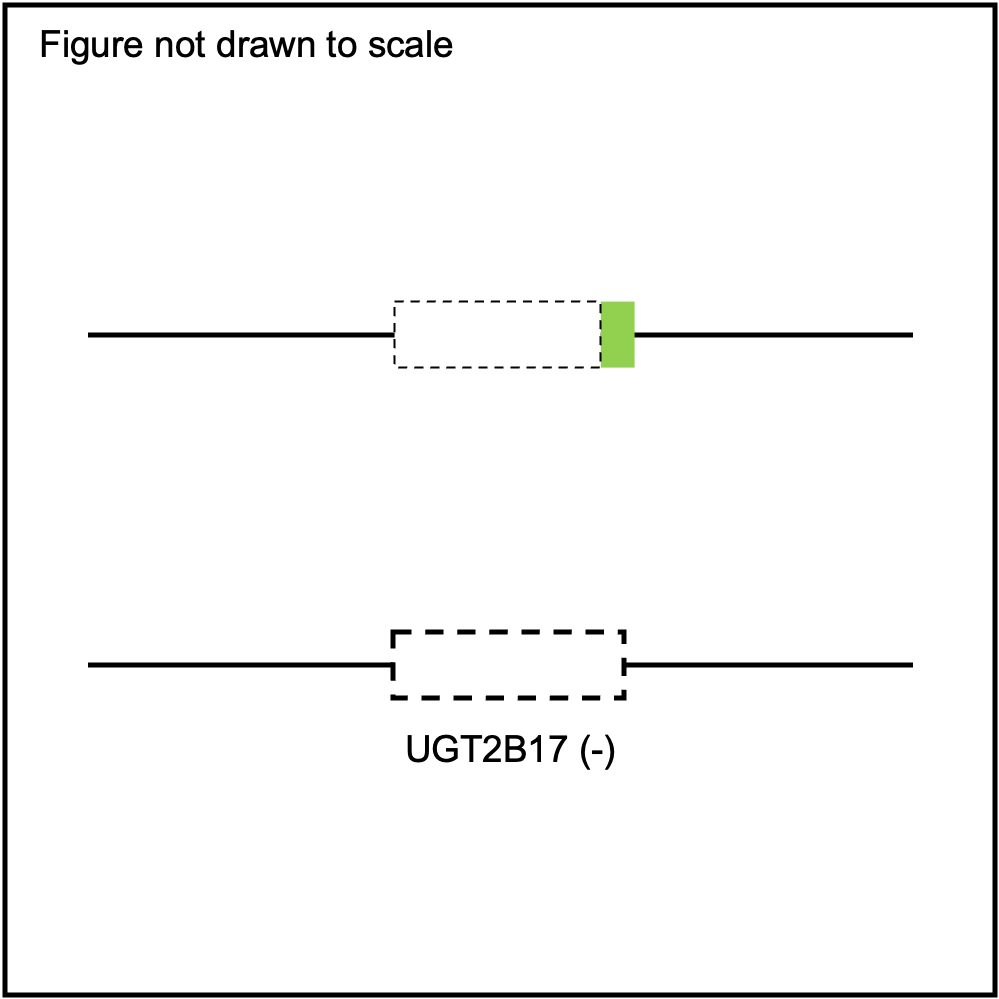{kind=link}
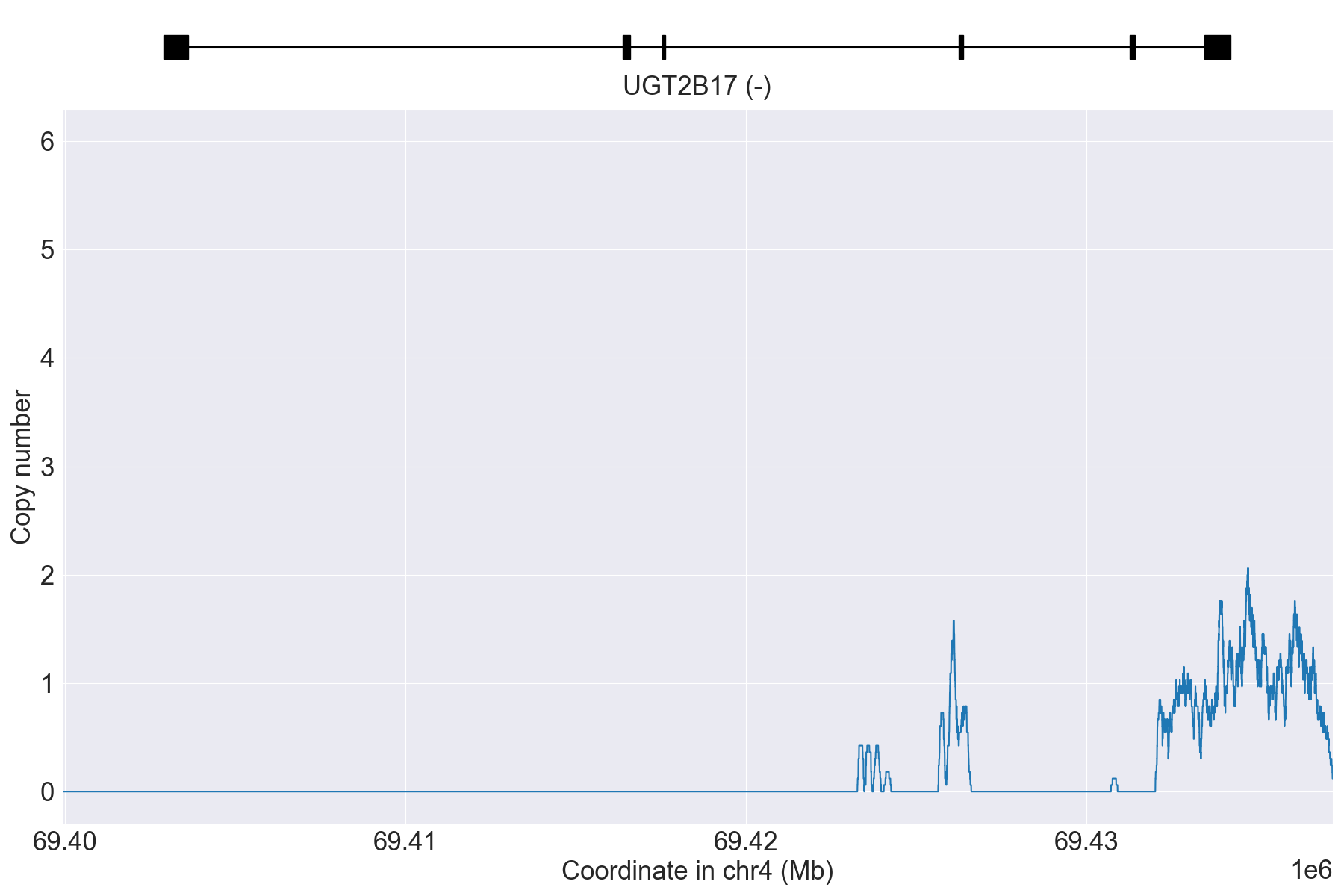{kind=link}
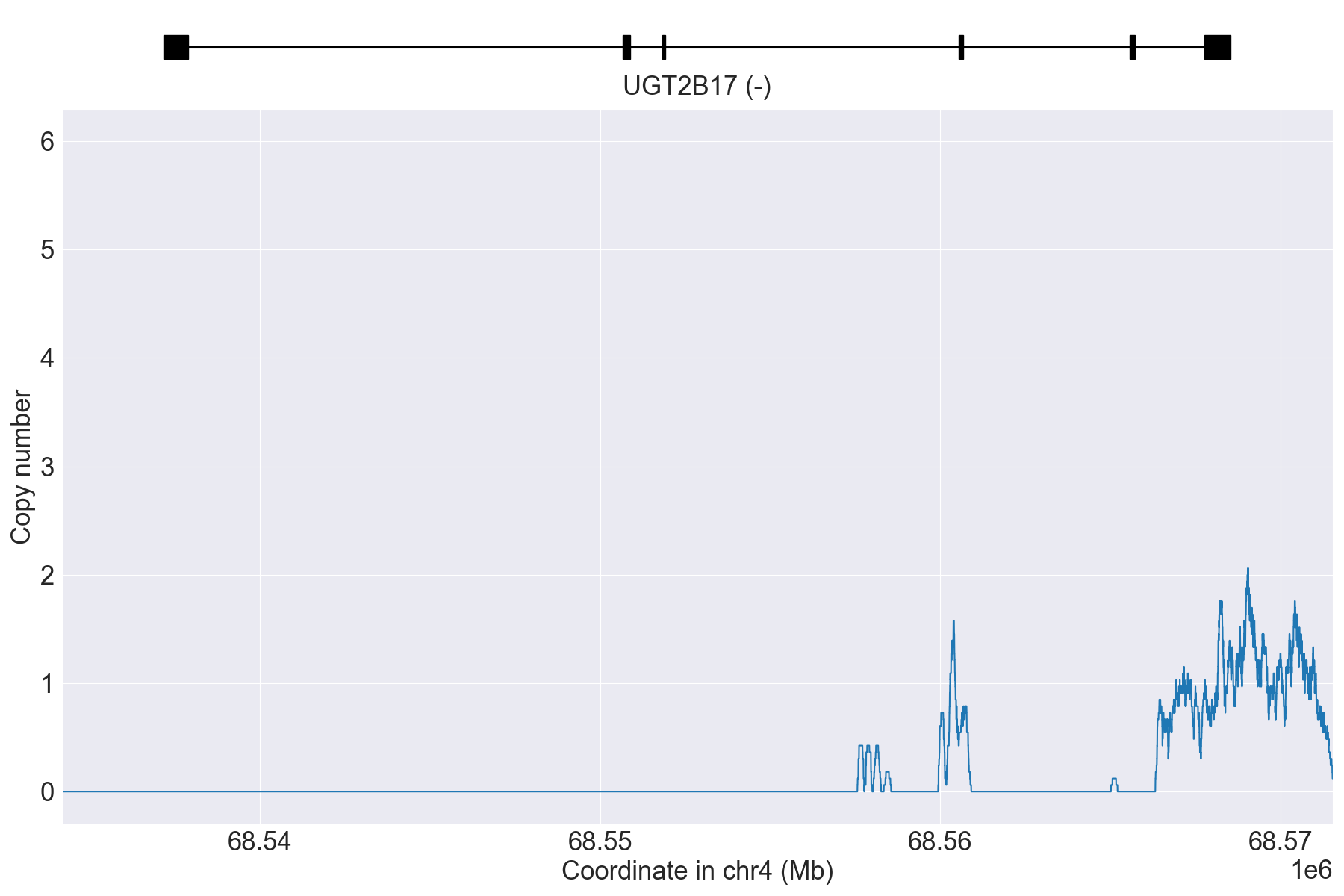{kind=link}
PyPGx was recently applied to the entire high-coverage WGS dataset from 1KGP (N=2,504). Click here to see individual SV calls for UGT2B17, and corresponding copy number profiles and allele fraction profiles.